
Abstract


The Integrated Care Pathways 2010 conference (ICP 2010) was held at the Cavendish Conference Centre, London, on 23-24 June 2010. A report about this conference has been published in this current issue. In this section we will focus on a number of topics, using a selection of abstracts from ICP 2010.
The patient journey across boundaries: Aneurin Bevan Health Board's approach to pathway development using Map of Medicine
Joanna Dundon
Aneurin Bevan Health Board, Planning, Informing Healthcare, part of NHS Wales Informatics Service, Implementation Directorate, Torfaen, UK
Objectives: These were as follows:
Demonstrate the use of Map of Medicine as a clinical pathways tool to develop a whole systems approach to patient journey for chronic obstructive pulmonary disorder (COPD), stroke, normal pregnancy and arthroplasty;
Use of the whole systems approach to develop and design processes for clinical governance and best practice, workforce development, infrastructure of services and target delivery;
Use of variance indicators to measure improvements and change in practice at various points along the pathway to enable tracking of movement/saving of resources.
Methods: As part of a Clinical Futures Programme across Gwent (covering five localities in South East Wales), a pathway development project was set up to bring together all parts of health and social care to look at four pathways using Map of Medicine: arthroplasty (hip), COPD, normal pregnancy and stroke. A joint board at executive level across the organization was established to ensure the delivery of this pathways work. The project is also linked to the strategic/corporate planning processes across the organizations - Clinical Futures, Public Health Wales Programmes, primary/community care planning, workforce planning, clinical governance structures and information and finance processes. The workstreams for the four pathways set up included public health, acute care clinicians (medical, nursing and allied health professionals), primary care, ambulance service, social care partners, patients, information teams, clinical governance, workforce modernization and finance representation. The work-streams were chosen to represent high cost and volume patients, high (re) admission to secondary care and to consider relevant changes in practice by bringing all professionals together. An audit of data obtained from information systems has been conducted to map against the current pathways. A consultation process with all stakeholders then ensured a change to the pathway in line with detailed discussions with clinical and managerial input. Performance indicators were built in at appropriate nodes for a re-audit to identify changes in practice across all aspects of the pathway.
Results: Each pathway had a different challenge: arthroplasty - admission and discharge; COPD - management of patient in community not within secondary care leading to service redesign; normal pregnancy - keeping patients on the midwifery-led pathway and using All Wales labour pathway for variance tracking.
Improvement and changes can only come from clinical sign-up to changes in the patient journey across the elements of the pathways. This needs to be identified through a clear involvement process and evidence-based links to NICE guidelines, Royal College Guidance, National Service Frameworks, Annual Operating Framework targets, Access 2009 (waiting times) targets, and so on.
The project plan identified implementation processes and timescales for development and delivery of the pathways across the health board, communicating widely at all types of meetings and visits to wards, followed by re-audit six months later. Any changes will be made to the pathway on the Map and available for all to see.
One of the main aims of the project and probably the most difficult was to identify and capture the outcome/ variance assumptions through changes in the patient journey. This can only be measured once the pathways are implemented and in use for a period of time. However, a Benefits Realization Framework has been developed, which identifies the proposed changes in the pathway process and also enables benefits for patients, staff and the organization that can be tracked through the relevant nodes of the pathway through the Map of Medicine. There are a range of direct and indirect outcome measurements and benefits that have been built into the pathways for taking forward this approach:
Patient-centred impacts - improve patient decision-making, improve patient experience; organizational impacts - reduce admissions, readmissions, inappropriate referrals, unnecessary tests and steps, length of stay pathway design discipline, communications across care settings, consistence of care, capability to achieve national and local targets, improved utilization of financial and staff resources, reduce direct costs, reduce duplication of services, etc.
Conclusions: The visual journey created using the Map as a tool:
Enabled agreement of care of the patient across the whole patient journey through collaboration of changes in the pathway between health and social care professionals;
Aimed to keep people out of hospital care and within primary, community and home care with the relevant professionals delivering care at the point of need. This can be achieved through changes in admission and treatment processes, through changes in clinical/referral guidelines education and support and referral to alternative care before secondary care process;
Ensured that by having an essential robust communication process to ensure the sign-up across all organizations and professionals. Critical to this success and delivery of the pathways is clear leadership and dedicated staff at a relevant level to enable focus for the delivery of the work programmes;
Ensured that the process was patient-centred and improved the patient's journey through all the various services;
Ensured that the boundaries of care needed discussion and debate but ultimately the patient should be at the centre;
Ensured that clear user/patient involvement strategies were built into the beginning of any project process, although the inclusion of patients at different times of the project process will vary depending on the service being discussed and the current agreement on how that service should be delivered across professionals. A judgement on when involvement is necessary and relevant needs to be made as the project progresses.
The relationship between clinical audit and care pathways
Robin Burgess
Healthcare Quality Improvement Partnership (HQIP), London, UK
Background: Clinical audit and care pathways are closely related. Clinical audit provides a means of in-depth analysis of the degree to which practice matches agreed evidence-based standards, and inspires and measures the implementation of action plans to address any failings identified. Care pathways provide a mechanism for conducting a form of continuous clinical audit as part of routine recording of care activity, gathering and using data to drive service improvements quickly and effectively.
Conclusions: Clinical audit should be used to set the baseline against which the care pathway should record data, and to assess the utility of the care pathway and its continuing effectiveness. National audits of the implementation of care pathways at the local level can help ensure that standards are met over time and to show patterns of variation not apparent from local audit. Good examples include national audits of implementation of the Liverpool care of the dying patient pathway. Healthcare Quality Improvement Partnership (HQIP) has published guidance on the relationship between clinical audit and care pathways, written by Mary Pearce, ‘Guide to carrying out clinical audits on the implementation of care pathways’ (HQIP 2010).
Children and young people, emergency and urgent care pathways
Kath Evans, Venkat Reddy and Christine McDermott
NHS Institute for Innovation & Improvement, Children & Young People Emergency Care Pathway, Coventry, UK
Objectives: In National Health Service (NHS) England, more than 25% of all patients seen in emergency departments are children. This equates to more than three million children every year. There are a particularly high number of cases presenting with respiratory problems, fever, accidental injuries, diarrhoea and vomiting, abdominal pain, fits and fainting. These common illnesses and injuries account for 85% of all emergency activity.
It is known that Accident and Emergency (A&E) departments often struggle to see patients waiting within a reasonable timescale. In some Trusts, as low as 4% of children presenting to A&E actually require admission to hospital, and in others 24% are admitted, the average proportion being 20%. So most children are sent home after being treated in A&E.
Emergency and Urgent Care for Children and Young People is one of the high volume care pathways focused on by the NHS Institute for Innovation & Improvement in its Delivering Quality & Value Programme. The NHS Institute launched a Focus on Emergency and Urgent Care for Children and Young People in 2008. This guidance features 19 characteristics found to be key to delivering high quality and value care in this area. It offers case stories with suggested measures to help NHS teams with continuous improvements for children and young people.
There is also a toolkit with guidance, a DVD, a poster and teaching plan to help the NHS and schools engage children and young people in improving local health-care services. This toolkit has been developed with children and young people, in collaboration with national stakeholders including The Royal College of Nursing and teachers involved in health and social care courses. It has been tested as part of the Delivering Quality and Value Rapid Improvement Programme.
Methods: Trusts and primary care trusts (PCTs) from each strategic health authority region in England were invited to join the Rapid Improvement Programme to work with the NHS Institute's Emergency and Urgent Care for Children and Young People Team. Thirty-nine applications were received in all; ten collaborative hospital and PCT applications were successful, one in each strategic health authority region.
During 2009/2010, the Emergency and Urgent Care for Children and Young People team have been working with the successful trusts to improve the quality and value of care provided to children and young people, by transforming care pathways and processes within short timescales.
The sites are focusing on pathway development of five high-volume clinical presentations and are developing whole system pathways for:
The management of the febrile child;
The child with gastroenteritis;
The infant/child with bronchiolitis;
The child with asthma;
The child experiencing a head injury.
Results: The results are shown in Figure 1.

Results of the National Rapid Improvement Programme © NHS Institute for Innovation and Improvement 2010
Conclusions: The results of whole system pathway reform aim for total impact of a 25% reduction in admissions and a 25% reduction in zero length of stay, estimating significant savings in the future.
Rapidly improving hip fracture pathways
Elizabeth Aitken*, Philip Roberts† and Kate Hall‡
*Department of Medicine for Elderly, University Hospital Lewisham, London; †NHS Institute for Innovation and Improvement, Coventry, UK
Background: Hip fractures typically occur due to a fall in an older person. The numbers of hip fractures has been rising by 2% annually from 1999 to 2006 and is predicted to continue to rise. Ten percent of people will die within the first month after a hip fracture and at one year one-third have died.
In 2006, the NHS Institute for Innovation and Improvement published a Focus On Document that highlighted the large variation both in the length of stay and mortality after hip fracture. High performing Trusts and less well performing Trusts were studied, and the care pathways reviewed, to produce indicators that improved quality and value of care to these patients. These findings were then tested in other sites to ensure reproducibility. This document was adopted by only a few Trusts and so the Department of Health commissioned the NHS Institute to develop a programme to implement the pathway. One Trust in each strategic health authority was selected to participate in the Rapid Improvement Programme.
The aims of the programme were:
Share national data on variation of care for patients admitted with a fractured neck of femur;
Provide participating trusts with a full insight to the key findings in the Focus On Document;
Provide each trust with a practical knowledge of the pathway supporting toolkit;
Increase awareness of best practice in the care of patients admitted with a fractured neck of femur;
Time for networking, discussion, debate and planning;
Encourage adoption, change and establish regional networks to spread learning.
Methods: NHS Institute staff worked with the selected Trust over a period of 12 weeks. The Trusts were challenged to look at the pathway of care for hip fracture and to identify the problem areas. A multiprofessional team and steering group were established and objectives and timescales were agreed. As part of the assessment the team ‘walked the patient pathway’.
Representatives from the multidisciplinary team walked from the emergency department to the discharge lounge, questioning staff on the way and the processes used in the care of hip fracture patients. The team gained valuable insight into the current pathway and bottlenecks and led to new ways of thinking and understanding the roles of each department.
Issues specific to the pathway were identified and three or four key issues were selected for work during the programme term.
Results: The main issues identified in all trusts were:
Fast-track to the appropriate ward from the emergency department;
Early involvement of the geriatrician and anaesthetist;
Optimization of patients for theatre within 48 hours;
Mobilization postsurgery;
Early conversations with Social Services & Primary Care regarding discharge;
Collection of data to understand where there were bottlenecks.
Many generic solutions were found and included:
Standardization of patient information and the setting of an estimated date of discharge;
Dedicated unit or area for admission and ongoing treatment of patients with hip fracture. All the team understand the pathway and works to a common goal;
In order to facilitate rapid admission, Trusts have established an ambulance service pre-alert in association with fast-tracking through the Emergency Department;
Anaesthetic guidelines for hip fracture surgery have ensured a consistent approach and reduced wait for theatre;
Trials of senior orthogeriatric review have been used, resulting in business cases for permanent appointment;
Review of theatre lists has led to establishment of daily trauma lists (including weekends) or dedicated slots for hip fractures allowing patients to access theatre more rapidly;
Seven-day therapy input and training of non-therapy staff to ensure patients are mobilized over weekends and bank holidays;
Key measures for improvement have allowed teams to identify on a weekly basis where the pathway needs to be reviewed;
Key factors for success in all Trusts are people recognizing the need and desire to change;
The use of metrics and getting baseline data and continuing to collect data to demonstrate progress through the project;
Ensure there is a robust structure and plan that is realistic and try small changes.
Please seeTable 1 for more information.
Results of the Hip Fracture Pathway project
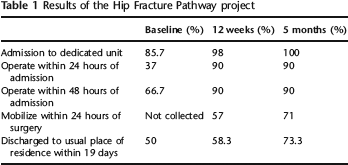
Conclusions: Improvements in fractured neck of femur care is possible in a short time period, with significant improvements being seen in all sites. A number of tools have been designed, including an estimated date of discharge tool, nutrition protocol, anaesthetic guidelines and mobility predictors. Key measures for improvement have shown Trusts areas where they need to improve and have allowed them to see how quickly change has resulted in improvements. These are now available for all NHS Trusts to use. Using the principles of the key characteristics of the Focus On Document, with development of pathways of care, results in significant improvements in hip fracture care that all Trusts should consider as a clinical governance priority.
Restricted, foreign national, mentally-disordered offenders’ pathways through psychiatric secure services in the UK
Bradley Hillier and Paul Gilluley
West London Forensic Service, Southall, UK
Background: Changes in Home Office policy direct that non-UK national, restricted, mentally-disordered offenders (MDOs) must be considered for deportation. A recent study suggests that there may be significant numbers to whom deportation criteria may apply within secure psychiatric services in the UK. The ensuing process for consideration for deportation of restricted MDOs can be lengthy, costly and is often not considered within the patient's care pathway at present. This can considerably affect the care pathway envisaged in a patient's rehabilitation.
Aims: This study aims to clarify the current pathways for non-UK national restricted MDOs; to identify the points in the current processes that lead to blockages; and to discuss the possibilities for improving the pathways through secure psychiatric care for this patient group.
Methods: Information was obtained from the MDO team at the United Kingdom Borders Agency and the Ministry of Justice to establish the current pathways and deportation criteria for non-UK national MDOs. A literature search was carried out to establish current practice. Experiences of colleagues liaising with various Embassies were also recorded.
Discussion and conclusions: At present there are no clear pathways for non-UK national MDOs through secure psychiatric services that take potential deportation into consideration. Blockages occur at numerous points in both deportation and repatriation processes. It is proposed that consideration for deportation should occur earlier to allow this to be incorporated in the patient's care plan; any legal process should run concurrently with medical treatment to inform the onward care pathway towards rehabilitation, repatriation or deportation.
Developing an integrated pathway for assessing and managing risks associated with mental health problems using the GRiST mental-health risk and social care assessment tool
Christopher Buckingham*, Ann Adams†, Eleanor Gilbert† and Laura Vail†
*Computer Science, Aston University, Birmingham; †University of Warwick, Warwick Medical School, Coventry, UK
Objectives: The objectives of the GRiST Research Programme are:
To develop a web-based decision-support system based on clinical expertise to support the assessment and management of risks associated with mental health problems, i.e. an e-pathway;
To develop different versions of GRiST to enable users in any health and social care context (including clinicians, support staff, carers and service users) to speak a common risk language, and thus communicate and act on risk information more effectively across multiple boundaries;
To promote: safety for all; self-management and empowerment for service users; and to provide a clear audit trail for NHS Trusts to demonstrate the relationship between patients’ risk profiles, clinicians’ risk judgements, management plans and outcomes of care.
Methods: The model of risk that underpins the GRiST decision-support system (www.galassify.org/grist) was developed based on analysing 46 in-depth interviews with multi-disciplinary clinicians who regularly undertake risk assessment of patients with mental health problems. Each clinician's account of the factors they take into consideration when assessing risk was used to create a mind map representation of their risk knowledge, using the Freemind software package. These were validated with each clinician. Individual mind maps were subsequently integrated to produce very detailed representations of the factors the whole sample of clinicians consider when assessing the risks of suicide, self-harm, harm to others, self-neglect and vulnerability. The identified risks emerged from the data analysis. The net result was a large, hierarchical model of risk, with observable indicators of risk at the lowest level, connected to the high-level risks through a series of intervening concepts. For example, inability to sleep and loss of motivation are connected to the high-level risk of suicide through the intervening concept of depression.
The data collection interface for GRiST was developed through pruning the model through a series of focus groups and on-line consensus building exercises undertaken with a panel of over 100 clinicians. The Working Age Adults’ version of GRiST has subsequently been piloted and taken up as routine practice in two NHS Mental Health Trusts, where it has been validated now by thousands of clinicians.
Customized versions of GRiST have subsequently been developed for older people, young people, primary care improving access to psychological therapies (IAPT) services and a self-assessment version for service users.
These have been developed through interviews and iterative focus group discussions with relevant clinicians and service users. These are being piloted in three Trusts.
Moving GRiST on from being simply a risk data collection tool to becoming a decision-support system has involved interviews and on-line tasks with expert clinicians. These activities have captured clinicians’ views about the relative influences of individual risk factors, and about the contribution of each factor to maximum risk.
Results: There are now three validated versions of GRiST in routine use in NHS practice (working age adults [18-65 years], older adults, and children and adolescents versions), which provide a mechanism for collecting systematic and structured information to give detailed service user risk profiles across the lifespan. These support clinicians’ risk judgements. The service user version of GRiST will be demonstrated at the British Science Festival and launched in the Autumn of 2010, along with the IAPT version. This means that GRiST spans the entire patient care pathway from community to primary, and then secondary mental health care. It is also suitable for use in other frontline agencies which interface with these, e.g. the police, housing associations, prisons, the criminal justice system and accident and emergency departments.
Conclusions: There is a large and growing clinical demand for GRiST, which has shaped the direction of the research programme. Ongoing and future work focuses on connecting risk assessments and judgements to risk management planning and care packages. There is a good fit between the GRiST risk judgement scores and mechanisms in current use for determining which care clusters patients are allocated to. However, GRiST offers a much simpler and indeed an immediate way of achieving this linkage. Mechanisms in current use are complex and time-consuming to administer. This represents the final part of the integrated care pathway GRiST offers to people with mental health problems.
As the use of the GRiST web-based tool grows, so too will the database of anonymous risk profiles and associated risk judgements that GRiST collects. The decision-support system will contain sophisticated data analysis and pattern recognition tools, which will analyse the information in an ongoing way. This will generate detailed understanding about the relationships between risk information and risk judgements, trends and any inequalities associated with decision-making about risk. The database will also support improved risk prediction and offers the possibility of continuous feedback for improving the GRiST pathway.
Development and implementation of a gender specific psychological treatment pathway in low secure services
*Raphael Healthcare, The Farndon Unit, Nottinghamshire; †Raphael Healthcare, Head Office, Prescot, UK
Objective: To develop a psychological individualized gender-specific forensic treatment pathway, focusing on current best practice.
Method: This has been achieved by the following:
Joining key organizations;
Utilizing existing skills base;
Needs analysis of gender specific areas;
Accessing current best practice guidelines and training;
Accessing most current literature and studies;
Comprehensive admission assessment utilizing clinical rationale and evidence base;
Delivery and assessment of key psychological interventions.
Results: The following results were found:
In women's low secure services the understanding of personality is often overlooked;
The identification of previous trauma is paramount to any psychological intervention;
Patients in these settings often have limited recognition and understanding of emotions;
There is often a deficit in problem-solving skills with this patient group;
The need for a multileveled treatment pathway for successful treatment.
Conclusions: As the development and delivery of the service has progressed we have found the following:
A need for a robust admission assessment procedure;
A collaborative working approach with patient and multi-disciplinary team;
A need for an individualized treatment pathway;
Working to a strict timeframe for assessment feedback formulation;
The need for a pathway by initial Care Programme Approach at the 12-week period;
Development and implementation of a multitiered treatment pathway which is individualized to meet patient needs.
Developing a new assessment unit with patient-directed pathways for the acutely unwell oncology patient
T Chapman, J Ward, T Ahmed, C Benson and J Hofland
The Royal Marsden NHS Foundation Trust, Fulham Road, London, UK
Background: The Royal Marsden Hospital provides chemotherapy as an outpatient procedure. A proportion of patients who present to the unit are too unwell to receive their therapy, yet are unable to go to a walk-in assessment area, as there is not one in the trust. The objective is to introduce a clinical area for safe and early assessment of these patients, with directed pathways in place to ensure timely delivery of best care.
Method: Acute admissions over the previous 12 months were analysed and revealed 1602 patients requiring urgent admission following complications of their therapy; a significant number were for neutropenia and sepsis, ascities, spinal cord compression, diarrhoea, vomiting and thromboembolism. To help achieve clinical engagement, each major clinical problem was taken on by an individual specialist registrar tasked to develop a patient pathway. This is achieved using a lean’ mentality, ensuring that any test and assessment is done with minimum time consumption and in as few steps as possible to allow treatment to start promptly and safely.
Results: The pathways are being rolled out, allowing need for further admission, early discharge from hospital, time to treatment and need for higher-level care to be evaluated, along with the patient's appreciation of quick assessment in a centralized point of access.
Conclusion: The Royal Marsden recognizes the importance of early assessment and treatment of the acutely ill oncology patient. The clinically developed patient-directed pathways could potentially reduce length of stay, morbidity and mortality through early intervention for these patients.