
Abstract
Electronic health records (EHRs) that include computerized provider order entry (CPOE) have the potential to reduce medical errors and adverse drug events, improve health outcomes and reduce health care costs. The success of CPOE is dependent upon the development of standardized evidence-based order sets and care pathways that are developed and used by clinical providers. However, development is dependent upon the engagement and clinical expertise of health care providers who are busy caring for patients and may not have the time or resources to devote to order set development. This paper describes one academic institution's experience in adopting a new EHR that includes CPOE and the efforts to stimulate the development of order set content throughout all clinical sections and departments. Based on this experience, specific recommendations and guidance to facilitate the development of evidence-based order set and care pathway content are described in the article. Through the use of the described strategies and techniques, over a three-year period the institution developed, approved and implemented 495 order sets authored by 141 different providers and well exceeded the established goals of the committee and institution.
Project presentation
In 2008, Dartmouth-Hitchcock Medical Center (DHMC) determined that the implementation of a new electronic health record (EHR) that included computerized provider order entry (CPOE) was needed to improve patient care at its teaching hospital and associated community practices. DHMC is an academic medical centre located in Lebanon, New Hampshire, USA. The hospital has a 396-inpatient bed capacity and serves as a major tertiary-care referral site for northern New England. In 2009, DHMC had approximately 24,000 inpatient discharges and 1.7 million total outpatient visits.
While DHMC already had an internally developed and supported EHR that included access to provider notes, laboratory, pathology and radiology results, it was decided that adoption of a new EHR was needed in order to implement CPOE. Use of CPOE with clinical decision support systems has been shown to reduce medical errors and adverse drug events, improve health outcomes, reduce health care costs and improve management of certain chronic conditions. 1–5 The success of a CPOE system is dependent on the clinical community's willingness to develop easy to use, evidence-based, standardized order sets and care pathways.
Care pathways have been defined as ‘a complex intervention for the mutual decision-making and organization of care processes for a well-defined group of patients during a well-defined period’ with an aim to ‘enhance the quality of care across the continuum by improving risk-adjusted patient outcomes, promoting patient safety, increasing patient satisfaction and optimizing the use of resources’. 6 A meta-analysis of published studies of care pathways found that care pathways reduced in-hospital complications compared with usual care. 7 A key component to care pathways includes evidence-based order sets adapted for local use that explicitly direct the care for patients with specific diagnoses, conditions or therapies, and standardizes clinical care processes that occur in both the outpatient and inpatient settings.
The challenge to obtaining maximum return on any CPOE system is the creation of a robust set of order sets and care pathways, developed from an active author community that are reviewed and revised on a regular basis. To facilitate this effort, DHMC formed an Evidence Based Order Set (EBOS) committee comprised of physicians, nurses, pharmacists and members of the informatics group. Their goal was to increase the development of orders sets and care pathways throughout the institution. Over the course of two years, the EBOS committee worked with each clinical section to identify key admissions, procedures, medications and diagnoses to create order set content for the new EHR.
The EBOS committee developed strategies and techniques to stimulate content development throughout all clinical sections in the institution. Implementation of these strategies resulted in a dramatic increase in the quality and quantity of submissions. The following is a summary of the lessons learned by the committee on how to attract and engage providers, clinics and inpatient units in the development of high-quality standard order sets and care pathways.
An initial ‘gap analysis’ is critical in identifying which order sets and care pathways need to be created
At the outset, one of the goals of the EBOS committee was to develop standard evidence-based order set content for 80% of the most common diagnoses and procedures for each clinical section. Clinical providers, who are often focused on the complexity of providing care for individual patients, can be unsure of the most common procedures or diagnoses that they see on a regular basis. As a result, clinical providers may not have an idea of where to start their efforts in order set and care pathway development. One way to focus their energy is to identify the most common diagnoses and procedures encountered in their sections and determine which ones currently are not covered by existing order sets or care pathways. In addition to the most common diagnoses and procedures, special attention should be given to more rare, but higher risk conditions, such as chemotherapy or paediatric dosing that would benefit from standardized care. This list of common procedures and diagnoses was then compared with the current paper order sets that had been previously developed and implemented in the clinical setting. A ‘gap analysis’ was performed that identified the common procedures and diagnoses that were not associated with current order set content.
This ‘gap analysis’ is critical to ensuring that limited resources are not spent on creating order sets that will not be widely used or on ones that already exist. The initial analysis can be developed by individuals who have access to this information, such as practice managers or section chiefs, and then provided as a guide to content authors. This list should be looked at as a recommendation and starting point only, as it is ultimately up to the user community as to what order sets they want to build and will use in the future. Once the analysis is completed, specific care providers with the clinical knowledge and expertise can be quickly identified to author the order set content.
Although the focus was on common diagnoses and procedures within a particular specialty, order sets that are used by multiple specialties throughout the institution (i.e. orders for medications such as heparin and insulin continuous intravenous infusions that have associated nursing and lab orders that are used by patients with different diagnoses) should be included in the analysis as well and assigned ownership to one clinical section for regular review and revisions as needed.
Senior-level ownership of order set development needs to be communicated to all levels of the organization
At the beginning of the process, it was somewhat difficult to engage frontline clinical providers as they were often too busy providing direct patient care and frequently did not have protected time to work on order set content. Assigning ownership of the effort to senior leaders and administrators within each clinical section was critically important as they would then provide the time and resources to the busy clinicians to develop order set content.
The President of DHMC, the chair of the EBOS committee and other senior leadership presented the need for order sets to the senior physician and administrative leaders at the institution, and followed up with personalized letters and emails to convey their importance. They made it clear that the creation of this content was a requirement that should take precedence during the EHR planning and building phases. These presentations and letters had a great impact and resulted in significantly increased participation throughout all specialties in the institution.
Tracking each section's progress was communicated via the development of a ‘dashboard’. Using the gap analysis as a starting point, the dashboard allowed senior leadership to quickly determine which sections were actively engaged in the development process and which ones needed more encouragement or assistance with participation.
The order set approval process should be efficient and require minimal time requirements from providers
Standardized order sets and care pathways must go through an approval process prior to use to ensure that all orders are clear, safe, effective, compliant with institutional policies, and when possible evidence-based. At DHMC, any order set that included medications needed review and approval through the Pharmacy and Therapeutics (P + T) Committee. Prior to the current initiative to increase order set content, the P + T review and approval process for order sets was slow, required multiple meetings among many different stakeholders and often took between several months and a year to approve and implement an order set. One of the main sources of delays was that required revisions were identified at a review meeting and then the order sets were sent back to the provider authors. Then the authors needed to make the necessary changes and resubmit the order set for approval. Many authors waited several months to resubmit their order sets and as a result, the approval process for any specific order set took many months. Moreover, requirements, policies and even medical evidence would change during that time, potentially causing further need for revisions. During this protracted process, the authors of the order sets frequently would not know the stage in the approval process and what the barriers would be for final approval and use in patient care. Overall, the approval process was viewed as slow and not transparent. As such, many clinical providers who were interested in developing content to improve patient care did not become engaged in the process.
One of the initial goals of the EBOS committee was to simplify the approval process and minimize the amount of time needed from clinical providers. A single group that included all stakeholders was created so that the author only had to attend a single meeting. The composition of the committee included representatives from the physician leadership, nursing staff, medical records, informatics, quality and patient safety, risk management, pharmacy and the informatics group in charge of EHR implementation. Additionally, any other important representatives that would be critical to implementing an order set such as specific representatives from nursing, radiology, pharmacy or the quality and patient safety department, would be invited to the approval meeting to provide input and an added level of oversight. The order set is reviewed in its entirety at the one meeting so that any necessary changes can be immediately made and approved by the author. An order set that once took months to approve is now approved immediately after the meeting and available for use in four days after uploading to the current EHR.
Standardize and approve common components for order sets and care pathways to promote efficient creation of new content
With the development of order sets throughout the institution, it was discovered that different services have many components and procedures in common. For instance, the admission orders for a cystic fibrosis patient to the paediatric unit are very similar to the admission orders for a cystic fibrosis admission to the adult unit. Similarly, the parameters for nursing notification of a provider are similar for a surgery and a medicine patient. Rather than have each individual author create content independently, we have found that building ‘modules’ of order set content can help facilitate the creation and approval of order sets and care processes, along with standardizing common tasks throughout DHMC.
Common order set modules that were developed included:
Diet Parameters for notification of provider Activity Nursing interventions Antiemetics Venous thromboembolism prophylaxis Postoperative pain management Perioperative antibiotics Urinary catheter management
Through the use of these focused modules, care was easily standardized throughout the institution across many different specialties. At the same time, the build process for authors was simplified and the subsequent time necessary for order set development within the electronic medical record was similarly reduced through standardization of these modules across specialties. Additionally, compliance with institutional and national quality measures was enhanced through standardization of processes throughout the institution.
Have educational material and templates available to providers online
The development of order sets often requires education for content authors on the build, approval and implementation process. Busy clinical providers are often not able to meet during regular hours for educational sessions and create order set content in their spare time, when free from patient care duties. Posting educational resources online to guide clinicians in order set development was found to be extremely valuable. The EBOS committee developed an internal website accessible to all clinical providers that included order set templates and modules, examples of order sets from outside institutions, a current list of active and retired order sets, a ‘style guide’ that outlines standardized protocols and ordering guidelines, sample order set components, policy documents that explain the order set submission and approval workflow, reference guides such as TallMan medication names, and applications that authors can easily use to track the approval status of order sets they submit.
Providers should have access to individuals who are familiar with order set creation to help expedite the process
While having online resources was found to be very valuable in helping clinicians develop order set content, it was still necessary to have personal meetings with clinicians to engage and guide them through the development process. As most of the potential authors had not previously created order sets, it was important to arrange an initial meeting with an individual who had extensive experience in developing and implementing order sets and care pathways at the outset to explain the process, review their proposed content and formatting issues, discuss implementation issues, and expedite the approval process. Members of the EBOS committee typically served in this capacity. Also several ‘build sessions’ were held in the evening hours during which time additional one-on-one help was provided to clinicians along with dedicated time to work on the order set content.
In addition, having a dedicated individual who was responsible for managing and tracking the order set development, approval and uploading process was critical to the ongoing success of the process. It was extremely valuable to have a single point of contact that was available for any author with unresolved issues or questions regarding the submission and approval workflow for new order set content.
Checklists can help in ensuring that all aspects of order set development and approval are performed prior to implementation and use
While order sets and care pathways can be initially designed by a single physician, the specific orders contained within, often involve many different providers and clinical systems in the hospital such as nursing, pharmacy, radiology, physical therapy and respiratory therapy. Order sets must be reviewed by those who will be activating those orders prior to approval and implementation. A checklist that included necessary reviews and approvals was found to be helpful in the development process for content authors. This checklist ensured that all who would be involved with an order set or care pathway had reviewed the content and any necessary approvals or changes were obtained prior to being submitted to P&T for approval. This review process not only ensured that orders were clear and without errors, but also expedited the subsequent approval process and reduced issues with implementation (see Figure 1).
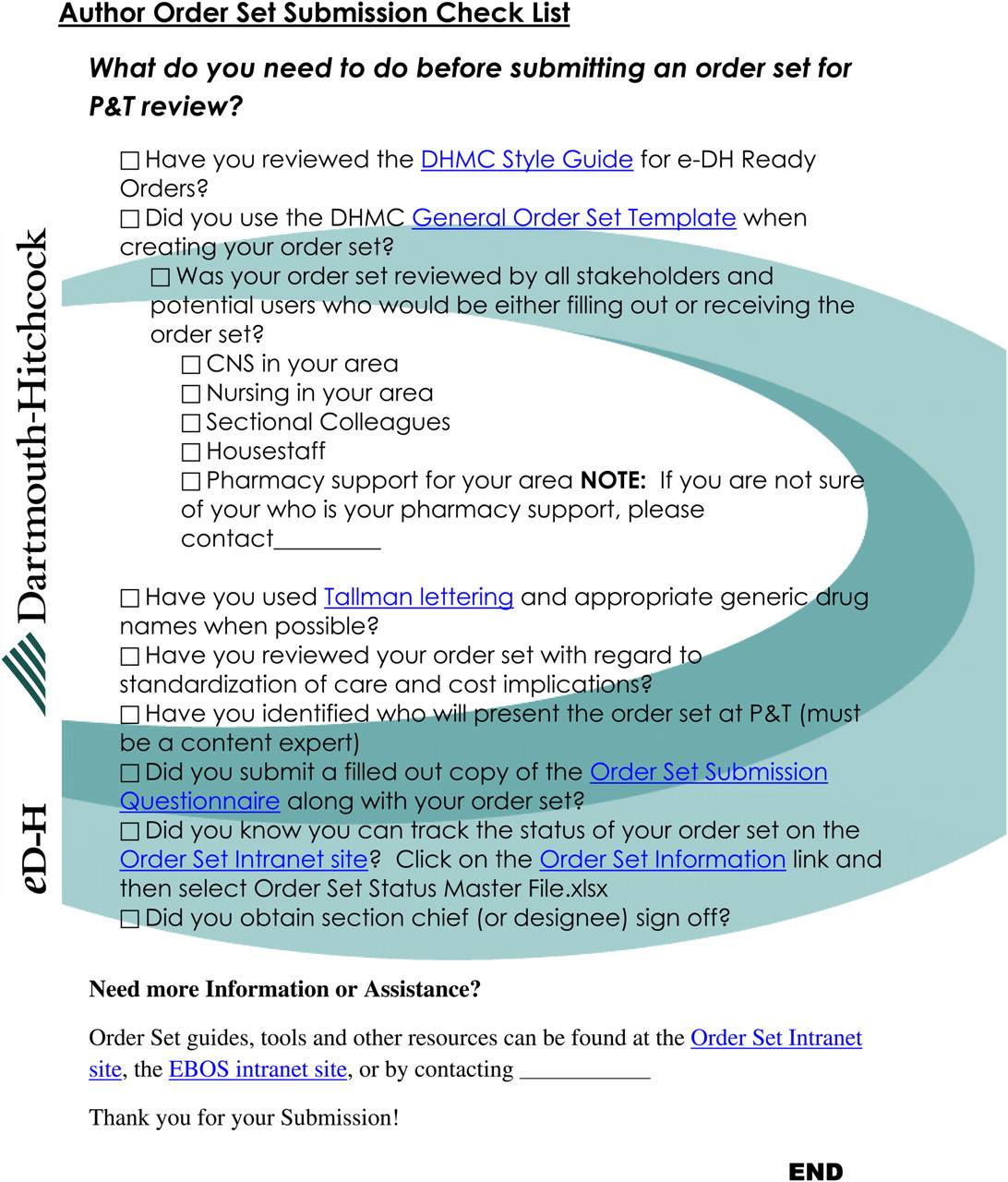
Author order set submission checklist
Conclusion
The above summarizes one academic institution's ‘lessons learned’ from the process to increase standard order set and care pathway development in preparation for a new EHR with CPOE implementation. Over the past three years that the EBOS committee has been active, there have been 495 order sets developed, approved and currently in use that were authored by over 141 providers from 41 different sections throughout the institution and these numbers continue to grow as the work of the EHR implementation continues throughout this year. The goal of 80% of all diagnoses and procedures established at the creation of the EBOS committee was surpassed and the order set content needed for CPOE implementation was provided well ahead of schedule.
Although the focus of this article is on the development and approval of new order set and care pathway content, a critical aspect that needs to be included within the implementation process is ongoing monitoring for intended and unintended effects of the order set content. Regular monitoring of the use of the order sets must occur to ensure that desired outcomes are achieved and unintended effects such as misuse of the order set, patient safety issues or ambiguous orders are addressed in a timely fashion. Furthermore, as scientific evidence and the literature base for the order sets evolve over time, the order sets that are based on that evidence also need to adjust to the changes. A process to revise or update order set and care pathway content should be in place to ensure that needed changes occur on a timely basis.
In conclusion, institutions preparing for implementation of CPOE will need to have a framework in place to facilitate the creation and approval of standardized evidence-based order sets. It is important to have a plan that assesses needs via a ‘gap analysis’, identifies appropriate content authors and enables them to produce high-quality order sets by guiding them through the process. Ensuring senior-level ownership that provides ongoing direct communication and encouragement to individual sections was beneficial. A multidisciplinary committee, such as our EBOS committee, is necessary to direct this process. A dedicated individual to monitor the approval and implementation process and to serve as a resource for content authors was critical to the success that was obtained. The EBOS committee was able to standardize order set development, improve approval efficiency and provide resources to all sections. Moreover, it ensured that all affected institutional constituencies would have direct input into each new order set. Using this strategy, our institution was able to develop and approve all of the needed order set and care pathway content prior to our anticipated ‘go-live’ date for implementation of the new EHR and CPOE.
DECLARATIONS