
Abstract
There is currently no standard in the UK for the management and prevention of bronchiolitis, leading to widespread variation in the management of infants. The authors feel that existing guidelines are not followed as a result of a lack of understanding and motivation to ensure that the necessary services and funding are available to manage patients according to recommendations. This pathway was developed to facilitate the implementation of standardized care for infants with or at risk for bronchiolitis. The integrated care pathway (ICP) for bronchiolitis was developed by a multidisciplinary steering group over the course of four facilitated workshops. During these workshops the steering group defined the ideal patient journey and then detailed each of the steps in the pathway with the information that should be assessed and collected to optimally manage patients. The results of the pathway development process and the ICP itself are the process map, ICP forms and the evidence review including commissioning outcomes. This ICP for bronchiolitis is based on expert consensus, multistakeholder input and a critique of published evidence. The steering group urges health professionals to work together across networks to improve the care for children both at risk for and with bronchiolitis.
Introduction
Scope
A steering group of National Health Service (NHS) professionals developed an evidence-based care pathway for children with bronchiolitis supported by a grant from Abbott Laboratories (North Chicago, IL, USA). This study outlines the process followed by the steering group to reach the full, evidence-based integrated care pathway (ICP), which takes the form of an algorithm and individual forms to guide and document patient care. It is, to our knowledge, the first time this has been done for bronchiolitis following the methodology outlined in this study. The authors believe that the development process for this pathway and its content (which we intend to host in a location where it is accessible to all) will be of substantial interest and relevance to the reader.
Background
Bronchiolitis is a major burden on young children, families and health-care providers in both primary and secondary care; it affects 22% of all infants and results in hospital admission of 2–3% of all infants. 1 Of those admitted, over 2% require intensive-care support and the mortality is 0.2% in all infants admitted. 2 The overall impact of this condition on health-care expenditure is substantial both during the acute illness and subsequently as both short- and long-term respiratory morbidity is well documented following bronchiolitis. 3
There is currently no standardization in the UK for the management and prevention of bronchiolitis, which leads to widespread variation in the management of infants with bronchiolitis both in hospital and, anecdotally, in the community. 4 The authors feel that existing guidelines such as the Scottish Intercollegiate Guidelines Network (SIGN) 5 are not followed due to a lack of understanding of what it is necessary to ‘do’ to change clinical habits and lack of motivation for commissioners to ensure that the necessary funding is in place to manage patients according to recommendations. 6
Clinical care pathways and ICPs are considered to be among the best vehicles for interpreting the evidence base often produced as guidelines and transforming them into improved patient outcomes by highlighting the essential steps from primary care through to secondary care and discharge. They are also useful in highlighting preventive strategies, particularly in high-risk patients. Many programmes and initiatives designed to support the quality, innovation, productivity and prevention (QIPP) objective include the development and implementation of clinical care pathways and ICPs, as their use has been shown to reduce in-hospital complications and potentially length of stay.
As an ICP for bronchiolitis should provide evidence-based recommendations on prevention, diagnosis, investigation, treatment and management (including the most appropriate use of diagnostic, referral and prognostic tools, particularly for those in primary care), it will be of interest to all health professionals in primary and secondary care involved in the management of infants with bronchiolitis including:
General practitioners; Practice nurses; Public health specialists; General and respiratory paediatricians; Neonatologists; Paediatric intensivists; Paediatric and neonatal nurses; Pharmacists; Commissioners.
Implementation of the ICP will support the delivery of ‘best possible’ outcomes for both preventing and treating children with bronchiolitis. There is evidence that clinical care pathways generally improve patient outcomes, including length of hospital stay, complications, documentation and costs.
6
The need to develop an ICP for bronchiolitis was discussed and validated by a series of advisory boards across the UK. The common view held across the members of the advisory boards, who went on to form the ICP Steering Group, was that delivering gold-standard, consistent care to patients with (or at risk of developing) bronchiolitis requires a tool which provides:
Referral pathways from primary to secondary and, for some, tertiary care; Investigations and treatments during the acute illness; Criteria against which all high-risk infants are assessed for prophylaxis.
Aims
This article has been written to share the development process of the ICP for bronchiolitis and the subsequent output – the ICP documentation itself. As the ICP was developed to facilitate the implementation of standardized care for infants with or at risk for bronchiolitis, the authors wish to share the process followed and the key findings that the authors believe may be applied in other therapy areas. The authors’ desire to share the development methodology and the outputs of the project is driven by their aim to see change in practice across the UK and improved outcomes for the health service and end users.
By disseminating the methodology used to develop this ICP (which has been employed to create ICPs in a number of other areas), the authors hope to increase the credibility of the outputs and encourage greater uptake of the ICP.
Methodology
The ICP for bronchiolitis was developed by a multidisciplinary steering group over the course of four facilitated workshops. During these workshops, the steering group defined the ideal patient journey and then detailed each of the steps in the pathway with the information that should be assessed and collected in order to optimally manage patients.
The multidisciplinary steering group comprised the following participants:
Andre Clinchant, Lead Nurse, Children's Community Nursing Service, Musgrove Park Hospital, Taunton, UK; Aung Soe, Consultant Neonatologist, Medway NHS Foundation Trust, Gillingham, UK; Denise Quinn, Advanced Neonatal Nurse Practitioner (ANNP), Neonatal Unit (NNU), Craigavon Area Hospital, Craigavon, Northern Ireland, UK; Emile Armour, Armour Sister/ANNP, Portsmouth Hospitals NHS Trust, Queen Alexandra Hospital, Portsmouth, UK; Jan Hovey, Paediatric Nurse, St Mary’s Hospital, Portsmouth, UK; Fiona Harris, Consultant in Public Health, Surrey, UK; Grenville Fox, Consultant Neonatologist, Evelina Children's Hospital, Guy's and St Thomas’ NHS Foundation Trust, London, UK; Liz Crathern, Programme Manager, Neonatal Care, School of Healthcare, University of Leeds, Leeds, UK; Rachel Hinchliffe, Commissioning Business Manager, Manchester, UK; Stephen Tomlin, Consultant Pharmacist, Evelina Children's Hospital, Guy's & St Thomas’ NHS Foundation Trust, London, UK; Commissioning pharmacist. Charles Unter, Consultant Paediatrician, Maidstone, UK; Phil Chetcuti, Consultant Paediatrician, Leeds, UK; Mike Thomas, General Practitioner and Asthma UK Senior Research Fellow, University of Aberdeen, Aberdeen, Scotland, UK. Steering group meetings, objectives and outcomes
In addition, the following clinicians were engaged in reviewing the ICP content outside the steering group meetings:
During four meetings held as workshops facilitated independently, the steering group worked through the process outlined in Table 1.
Results
The ICP
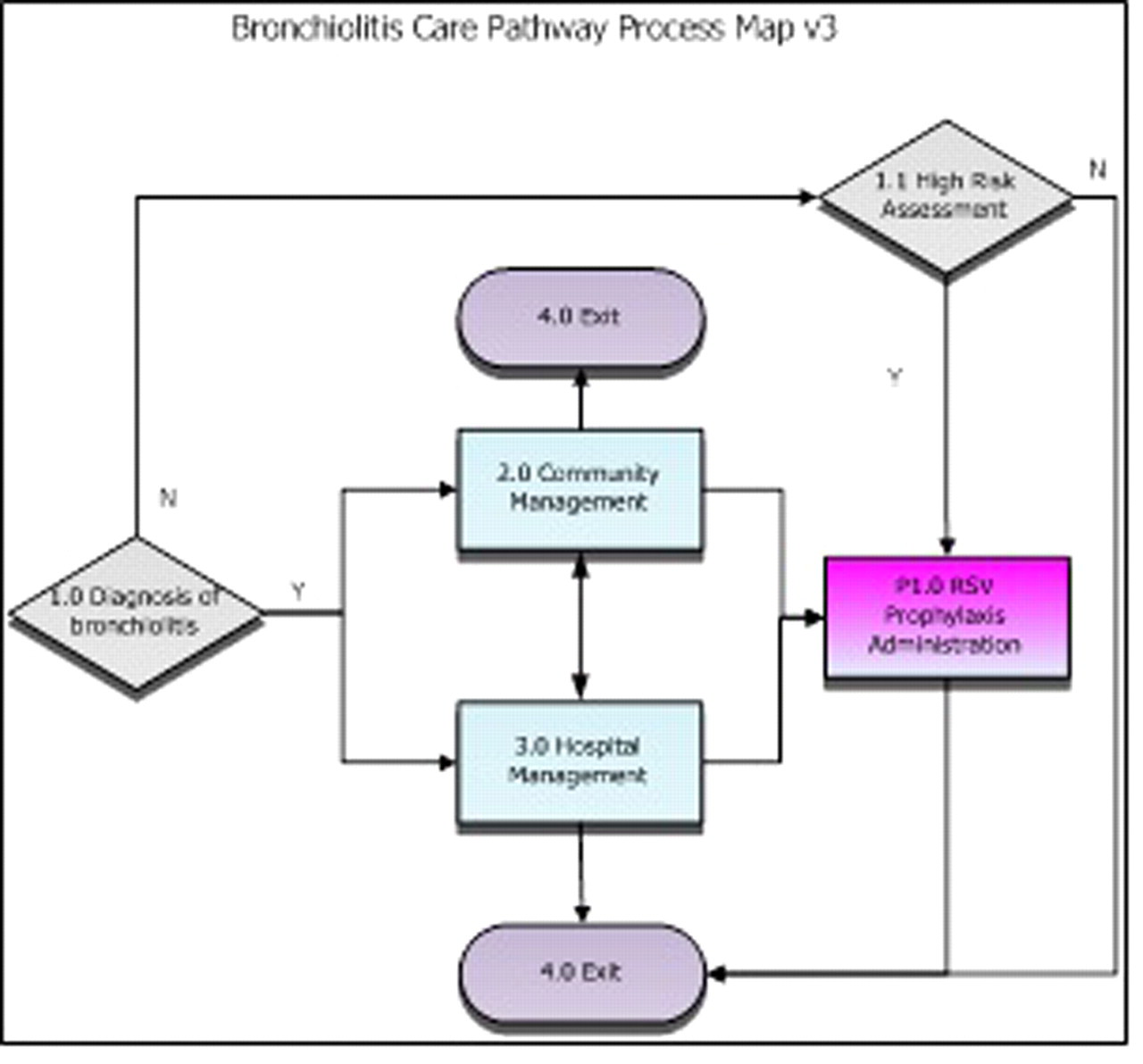
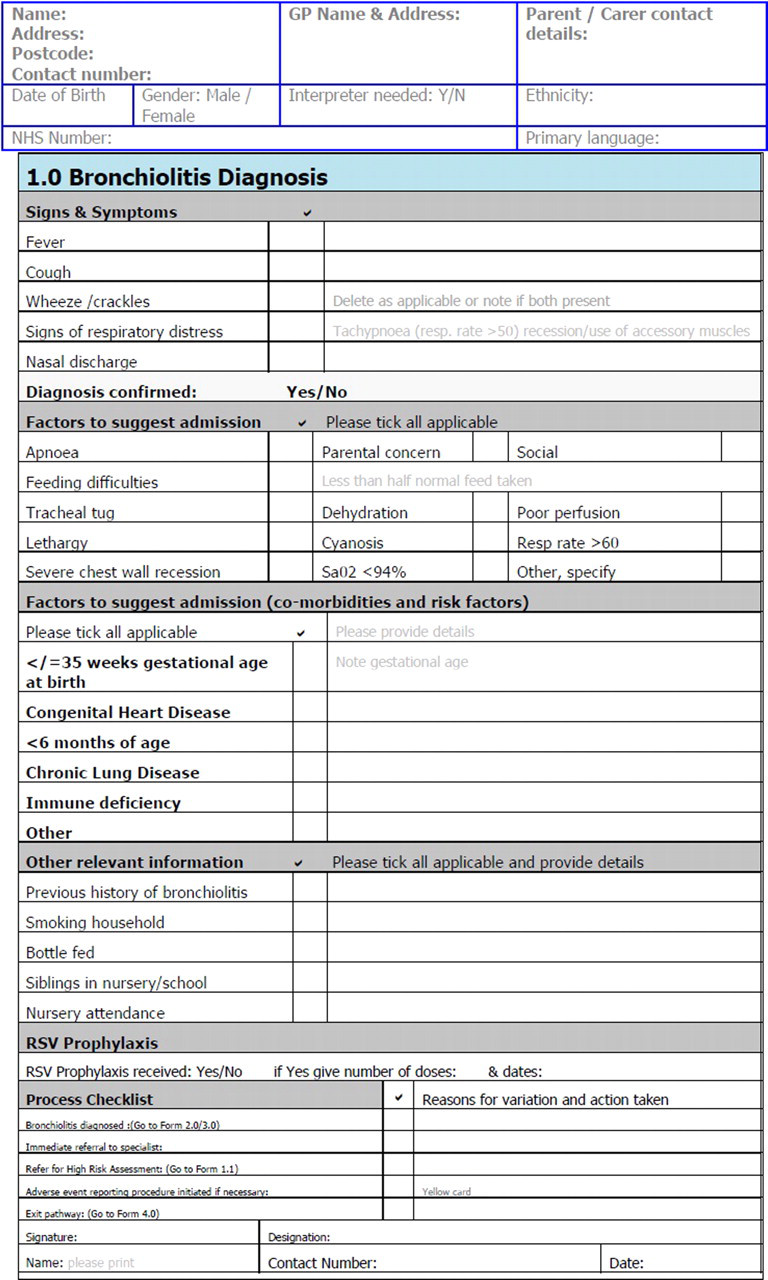
This ICP for bronchiolitis comprises a flow chart illustrating the patient journey (Figure 1), a series of forms (Figure 2) that provide clear guidance on patient management and a document summarizing and clarifying the relevant evidence base (Box 1). Each form includes a process checklist for the care of each patient intended to ensure that the relevant next steps are planned and taken and that variation from the recommended action is documented. Each section in the care pathway is supported by a summary of the current evidence to support decision-making at the relevant point of care and outlines the clinical outcomes that should be used to define and commission service provision.
The diagnosis of bronchiolitis is an important clinical decision and one that should be made based on history and examination findings.
Bronchiolitis is a lower respiratory tract disorder most commonly caused by viral infection characterized by acute inflammation, oedema and necrosis of epithelial cells lining bronchioles, increased mucus production and bronchospasm. A UK consensus guideline reported a definition of bronchiolitis as ‘a seasonal viral illness characterized by fever, nasal discharge and dry, wheezy cough. On examination there are fine inspiratory crackles and/or high pitched expiratory wheeze. During initial assessment, clinicians should consider risk factors indicative of severe disease: age less than 12 weeks, prematurity, underlying co-morbidity or immunodeficiency.
The course of bronchiolitis is variable and dynamic, ranging from transient events such as apnoea to progressive respiratory distress from lower airway obstruction. It is important to assess the impact of respiratory symptoms on feeding and hydration and the response, if any, to therapy. The ability of the family to care for the child at home, and to attend for review, should also be assessed. Any history of underlying conditions such as prematurity, cardiac or pulmonary disease, immunodeficiency or previous episodes of wheezing should be identified.
Bronchiolitis most commonly affects children under two years of age. By the age of one year, 70% of children will have been infected with respiratory syncytian virus. Indeed, 90% of cases requiring hospitalisation occur in infants under 12 months of age. Incidence peaks at 3–6 months.
Bronchiolitis more commonly presents between the months of November and March in the UK. Process map Example ICP formExample evidence base section
Service outcome measures
In addition to the ICP process map, forms and evidence base, the members of the steering group with commissioning and public health roles identified the data that must be captured in order to review the effectiveness of the service being delivered. For each step in the patient journey, a number of service outcome measures have been identified (Figure 3). In order to demonstrate the effectiveness and efficiency of bronchiolitis management based on this care pathway template, the steering group recommends that these measures are undertaken.
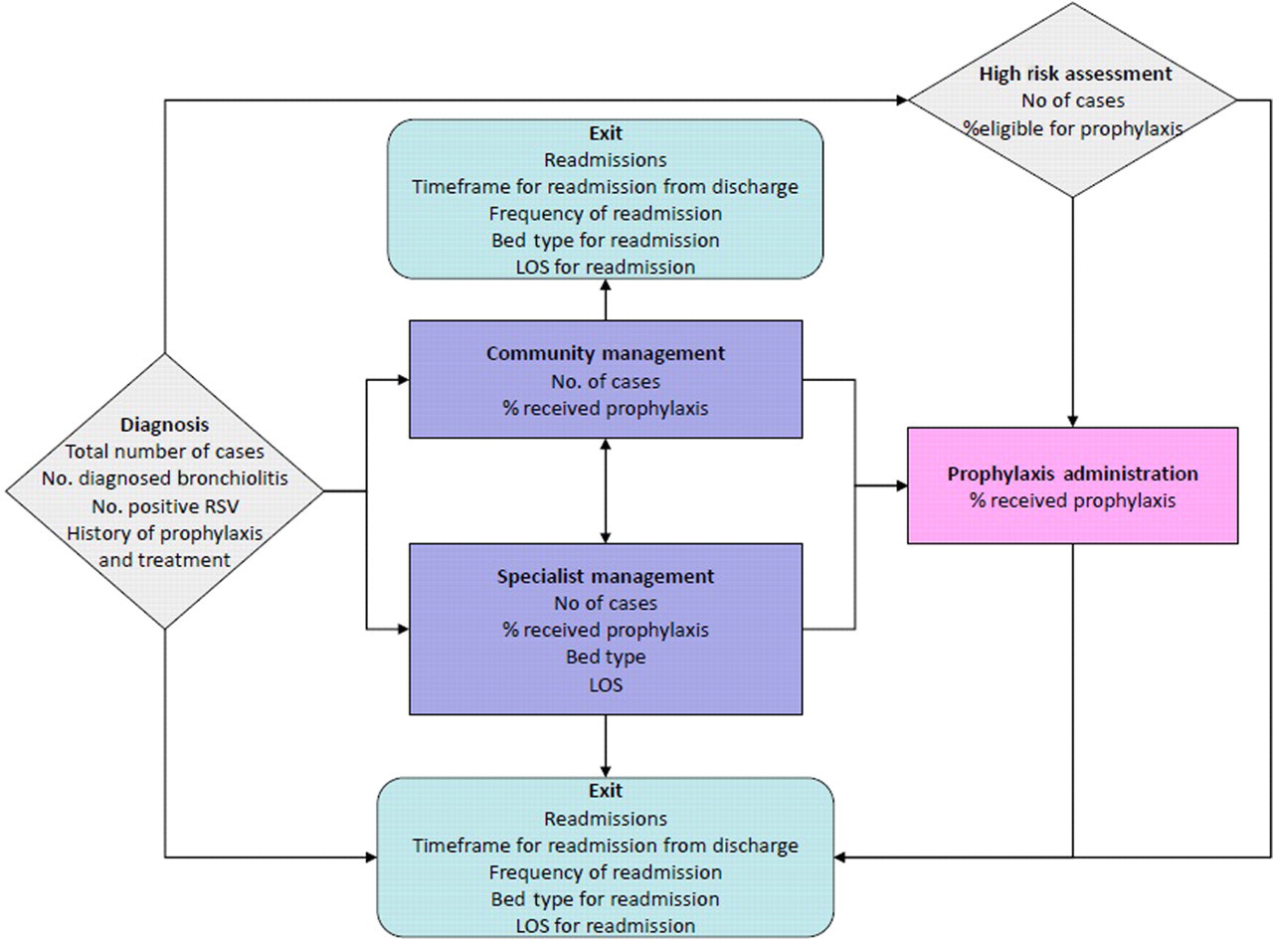
Measures to demonstrate the effectiveness and efficiency of bronchiolitis management
Conclusions
We present the development process for an ICP for bronchiolitis, which is based on expert consensus, multi-stakeholder input and a critique of published evidence. The steering group urges health professionals to work together across networks to improve the care for children at risk for and with bronchiolitis using the ICP and to audit the outcomes to measure improvement as a result of its use.
The authors believe that the process for developing this ICP may be replicated in many other therapy areas and their desire is to share both this process to support and inform the development of other ICPs, and the outputs of the project in the form of the care pathway itself.
It remains clear that the quality of care for children at risk of bronchiolitis in the UK is currently variable. Children who have had bronchiolitis deserve better care, which in turn will be cost-effective by preventing or controlling further episodes, as well as improving quality of life.
Discussion
This study has been written to share the development process of the ICP and the key learnings gained, which may be applied in other therapy areas. The authors’ desire to share the development methodology and the outputs of the project are driven by their aim to see change in practice across the UK and improved outcomes for the health service and end users.
By disseminating the methodology and key findings, the authors hope to increase the credibility, usability and ability to replicate the outputs and encourage greater uptake of the ICP.
It is anticipated that this pathway for bronchiolitis will be implemented locally by multidisciplinary teams working across local health economies, leading to more streamlined care of patients at risk for and diagnosed with bronchiolitis and appropriate acute and longer-term management of the disease.
It is hoped that the involvement of such a wide multidisciplinary team in the development of this ICP will encourage a wider audience to take interest in its content and support those wishing to engage commissioners in funding services for bronchiolitis management and prevention.
Conclusion
There is currently no standardization in the UK for the management and prevention of bronchiolitis, leading to widespread variation in management. The authors feel that existing guidelines such as SIGN are not followed due to a lack of understanding of what it is necessary to ‘do’ to change clinical routine and lack of motivation for commissioners to ensure that the necessary funding is in place. There is a need for a single approach for bronchiolitis, endorsed by all clinicians involved in the care of children and outlining a management strategy.
We believe that this ICP and the development process, which is based on expert consensus, multi-stakeholder input and a critique of published evidence adds to the existing guidance. The steering group believes that if health professionals work together across networks using this approach it will improve the care for children at risk for and with bronchiolitis. The authors believe that the process for developing this ICP may be replicated in many other therapy areas.
DECLARATIONS