
Abstract
The forensic care pathway that is the focus of this UK regional review has itself seen a considerable amount of change over the last decade, focusing on implementing wide reaching reform within both prison and health care. Reforms have seen a reduction in the number of people in some parts of the care pathway and new interventions and growth in other areas. At the end of 2009, the region that was subject to this review there had seen over 450 people cared for in high, medium or low secure services in that year and had a prison population approaching 10,000. The aim of the review was to understand the impact of these changes with a view to sustaining effective pathways and systems, and to increase impact and ensure value for money in order to improve the efficiency and quality of services. A primary objective was to consider the influence of statutory mental health provision upon the use of high, medium and low secure psychiatric services. It was proposed that from a regional perspective more needed to be understood about the influence of wider services upon the care pathways for people using secure services. This paper considers what is available from primary care locality and its features, alongside the rates of secure service use. It also acknowledges the wider influences upon the use of those services.
Introduction
The purpose of this review was to consider the influence of statutory mental health provision upon the use of high, medium and low secure psychiatric services. Under the auspices of health service delivery and organizational research it was argued that increased understanding of the use of secure services could further knowledge and service development in an informed way. In this case there is a need to assess the merits of different service models and determine their possible impact on high-cost, low-volume secure services.
The brief for this review posed the ultimate question: ‘which, if any available statutory mental health services correlate with a lower use of secure services in region?’ It was agreed that wider factors that may influence the use of secure services would also be considered at a population level. The review process commenced with a literature review undertaken to establish what is already known about the influence of the use of secure mental health services. This did not set out to focus on the clinical features, but concentrated on the routes and access to services. This was to specifically consider whether there are particular models of services that have been designed and developed that have influenced this pathway and population in past studies.
Literature review
The main focus of this review is the topic of forensic care pathways, although wider literature about access to forensic services, trends in their use, outcomes and evaluation are also drawn upon. The purpose of the literature review is to ascertain the most suitable method for this review, the specific questions to be answered, what is already known and what extraneous variables should be considered. Sources which focused upon purely clinical aspects were generally not included.
The literature is summarized in two main parts; a description of the elements of the forensic care pathway, and features of the system that influence the operation of the care pathway.
Rutherford and Duggan 1 described forensic services as those that provide care for mentally disordered offenders – people who have been in contact with the criminal justice system and who have been transferred to secure hospitals. They outlined two levels of security in forensic services hospitals to which offenders charged with an offence and prisoners can be transferred; these are high secure and medium secure. In addition to these are low secure services, where it is less likely that offenders are transferred directly from prisons or the courts. The majority of people transferred from prison or the courts initially enter high or medium secure facilities. It was reported that in 2006–2007 there were at that time 4500 secure places in high and medium secure forensic services for England and Wales. 1
Secure services are a significant part of the care pathway for mentally disordered offenders and others, who require treatment and care under conditions of security. They encompass subspecialties including mental health, learning disabilities, personality disorder, women and dangerous and severe personality disorder. The wider care pathway for individuals includes a comprehensive range of inpatient, prison and community-based services. The Bradley Report 2 outlines how there must be better management of the care pathway for prisoners who experience mental health problems starting with assessment prior to and on reception, improved primary mental health-care services in prison, evaluation of prison in reach services, reduced waiting for transfer to hospital from prison, provision for prisoners with a dual diagnosis, use of the care programme approach, that prisoners are supported and have access to mentoring during resettlement and that there is mental health training for prison staff.
There are a considerable number of influences in the flow of patients through forensic services that originate from features of the system. Cree and Hodgins 3 reported that since regional secure units were developed in the 1970s they have not been able to cope with the demand placed on them by the criminal justice system, the high secure hospitals and other routes of referral. It is suggested that this unmet need has blocked the rehabilitation of people from high secure beds. While it is acknowledged that provision has increased there has been variation in treatment programmes and their applications. Rutherford and Duggan 1 report the number of admissions via restricted hospital orders remaining static while transfers from prison have continually increased. While for a period between 2004 and 2005 the numbers received directly into high secure care fell, waiting times for transfer from prison often exceeded three months due to lack of available beds. Cree and Hodgins 3 offer the commentary that dedicated prison in reach saw an increase in the numbers transferred from prison under the mental health act, but there was often a delay in the times for transfer due to lack of beds at the receiving unit. Early in the delivery of this service interventions were focused upon identification and crisis. Laing and Buisson 4 assert that there is a financial incentive to contain transfers from prison to health services, since average prison costs are much lower than mental health hospital costs.
The qualitative factors that influence variations in pathways should not be overlooked, for example, Long et al. 5 report that the quality of living accommodation and access to a variety of psychological interventions can have an impact upon patient satisfaction. Patients showed a preference for the increased access to psychological therapies at high secure hospitals above what was available in medium secure services. Environmental factors in some units and the milieu contribute towards an increased sense of recovery and reduction in distressing symptoms and disturbed behaviour.
Heyman et al. 6 describe how medium and low secure units occupy a central role in forensic mental health care, bridging high secure and community services. They carried out a case study in a medium/low secure forensic mental health-care unit located in London. Impediments to the ideal progression of treatment and rehabilitation were explored through consideration of patient and staff perceptions of three issues: organizational processes; patients’ attempts to actively manage their own risk status and multidisciplinary collaboration.
The blocks to the two-year pathway and operation of the downward risk escalator included difficulties in risk assessment and management arising from patients’ strategic attempts to control their risk status, and reliance on mostly unfulfilled multiprofessional and interorganizational collaboration. The most noticeable outcome of these problems was a difference between perceived risk status; however, assessed, and the patient's location on the risk escalator, a conflict which undermined its therapeutic legitimacy.
Similarly, Tetley et al. 7 describe that personality disordered patients detained in high secure psychiatric hospitals appear to experience difficulties progressing to medium secure services. Examining the referrals to medium secure services for 80 previous and current patients from a personality disorder service and a dangerous and severe personality disorder service in one English high secure hospital suggested a poor success rate of referrals to medium secure units and extensive delays encountered in the transfer process. Brooker et al. 8 in their review of service delivery for prisoners with mental health problems recounted the limitations of pathways of care in the prison setting. Arising from the lack of skills, resources and cultural effects that lead to the failure to detect mental health problems within the prison population, there was a consequent lack of intervention for these individuals. Little is understood yet about the impact of training prison staff or the implementation of standards upon the interventions delivered or their outcomes.
In terms of the fuller pathway Brooker et al. 8 reported that offenders in the community experience difficulty accessing mental health services and over-use other crisis services. No data are available about the possible impact of variation on the wider pathway i.e. does the availability of community forensic psychiatry or access to locked rehabilitation provision impact the flow at lower levels of security.
Methods
The methods used to complete the review were largely descriptive and inferential statistics. To review any differences in the pathways between the nine primary care trusts (PCTs) descriptive statistics were used for the purpose of benchmarking. When considering whether a particular feature of a PCT is an ‘outlier’ the z-score function within SPSS (Statistical Package for Social Sciences; SPSS Inc., Chicago, IL, USA) is used. To review the relationships between the use of and spend on secure services and other factors tests of correlation were used. This was to consider three possibilities: (1) that there could be a positive relationship (i.e. the more that is spent on crisis resolution and home treatment services, the more is spent on medium secure services); (2) they could not be related at all, which would mean that the spend on medium secure services stayed the same regardless of how much is spent on crisis resolution and home treatment; or (3) they could be negatively related, which would mean that the more is spent on crisis resolution and home treatment services the less is spent on medium secure services.
In correlation research you cannot absolutely say one variable causes something to happen. This can only be done through experimental research. In correlation studies samples of over 20 cases are desirable and given the small sample size in this review all correlations were also examined by using scatter plots. It is acknowledged that this review considers nine PCTs and therefore as a sample this is too small for absolute conclusions to be drawn. Throughout the findings, any limitations are acknowledged, along with contrasts from the literature and possible explanations.
Sample
The data used for this review focused upon nine PCTs and three specific sources of data were used. These were the National Survey of Investment provided by Mental Health Strategies and published by the Department of Health which represents details of the investment in mental health services for working age adults (aged 18–64) in England for 2009–2010 and compares it with the reported results in previous years. Each year, commissioners report on mental health and older adult mental health expenditure through this national financial benchmarking exercise. The regional activity data for secure service use was extracted from the data-set held by the Specialised Commissioning Group. This provided an anonymous summary data for the years 2005–2010.
The population data source was the 2009–2010 and 2010–2011 PCT recurrent revenue allocations exposition book supplement: revised weighted populations accessible from the Department of Health. For the purpose of the analysis the mental health and mental health weighted and the unified weighted populations are used. Where there are notable differences these are highlighted.
Findings
Care pathway activity
Between 2006–2007 and 2009–2010 expenditure on secure and high dependency services across the region more than doubled, and within the period growth varied between the nine PCTs. Overall there is a growth in low secure and a decline in high secure occupied beds days (see Figure 1).
Service use over time (2005–2009)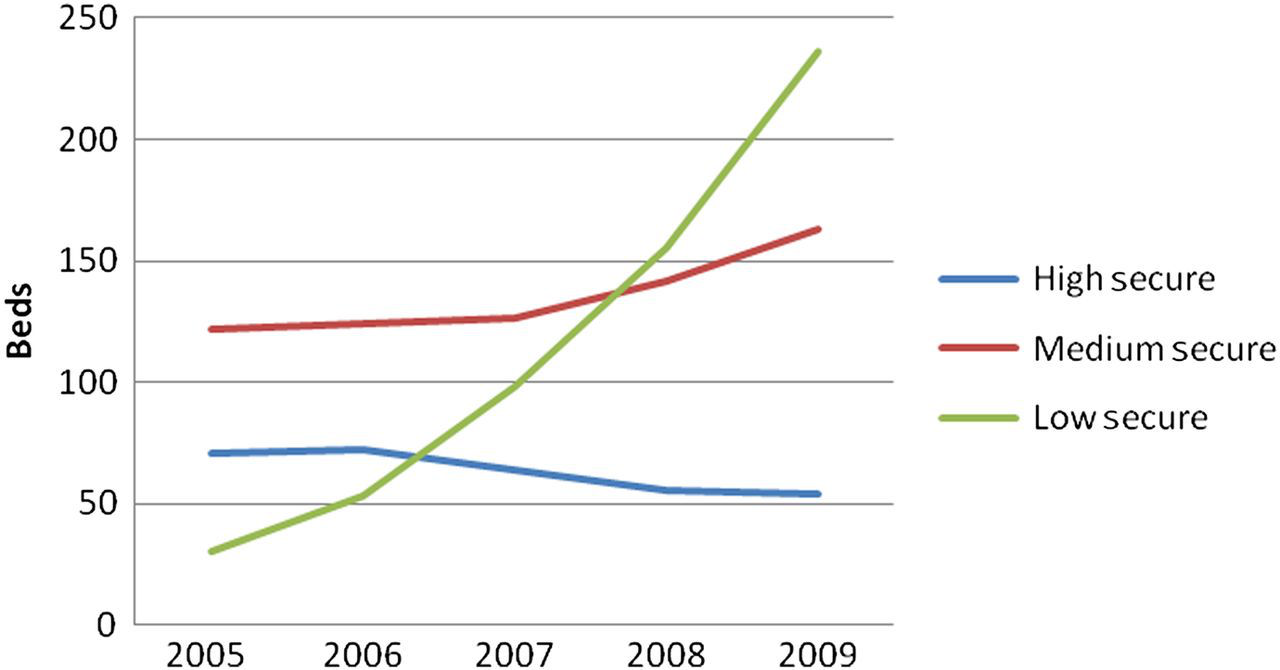
Between 2005 and 2010 the average length of stay for completed episodes in high security has fallen from 1728 to 1221 days. Medium secure average length of stays over the period, peak at 862 days in 2007 and show a minimum of 474 days in 2009. Although there are varying accounts about the anticipated length of stay in medium secure units, the regional usage is largely in line with the theoretical length of stay proposed by Heyman et al. 6 While the data are for completed episodes they do not correspond with 21% of patients staying beyond five years reported by Jacques et al. 9 Although the data are for completed episodes it is possible that some outliers exist in uncompleted episodes.
The most significant changes in the population have been
The fall between 2005 and 2009 in male learning disability and mental illness in high secure; The increase in medium secure male learning disability rising from 10 to 32 between 2005 and 2009, and male medium secure personality disorder rising from 16 to 30; The increase between 2007 and 2009 in low secure mental illness beds from 48 to 117.
Routes of admission and discharge
Figure 2 shows the overview of admissions to and discharges from secure services, and assumes either bottlenecks in the lower levels of security or increased capacity. Further analysis showed the sources of admission to each level of security. The notable factors in these breakdowns were that the rates of admission from local services to low secure services significantly outweigh those from medium secure services. This is contrary to the pathway described in the literature, where it was envisaged that the most common route of admission was to be for those moving down from a place of medium security.
Secure services admission and discharges summary (2005–2009)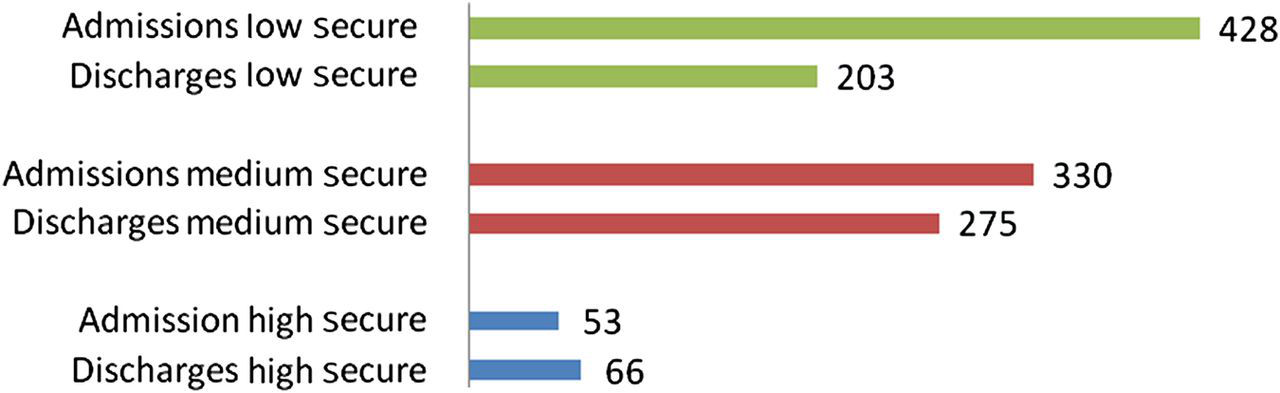
In the region prison as a source of admission to high secure services grew by 58% in 2009, and this is assumed to be directly linked to the increase in specialist mental health staff working in prisons, and implementation of the standards described in the offender mental health pathway tool. This is also consistent with Rutherford and Duggan's report 1 that transfers from prison into forensic services have continually increased. Increases in transfers from prison to low secure are also noted while referrals from prison to medium security have continually been the source of between 38 and 42 referrals a year with little variation since 2005.
The numbers discharged from high secure are a relatively small population and more significant patterns can be detected in the routes from low and medium secure. Routes from medium secure have been consistent over time with the largest percentage of patients being transferred to low secure services. While the most likely destination on discharge from low secure is to local services. Beer described the important role both psychiatric intensive care units and low secure units play in providing a bridge between forensic and general mental health services. Length of stay in intensive care and residential units has a probable impact upon the pathway out of low secure services. 10
Variation and relationships with other mental health spend
Figure 3 shows the sum of secure service occupied bed days (OBDs) (i.e. the total of low, medium and high secure beds days) averaged for 2008 and 2009, by PCT. The figure shows regardless of the population weight applied that PCT 2 has the highest OBD per weighted head.
Sum of the average secure services OBDs (2008–2009) by PCT population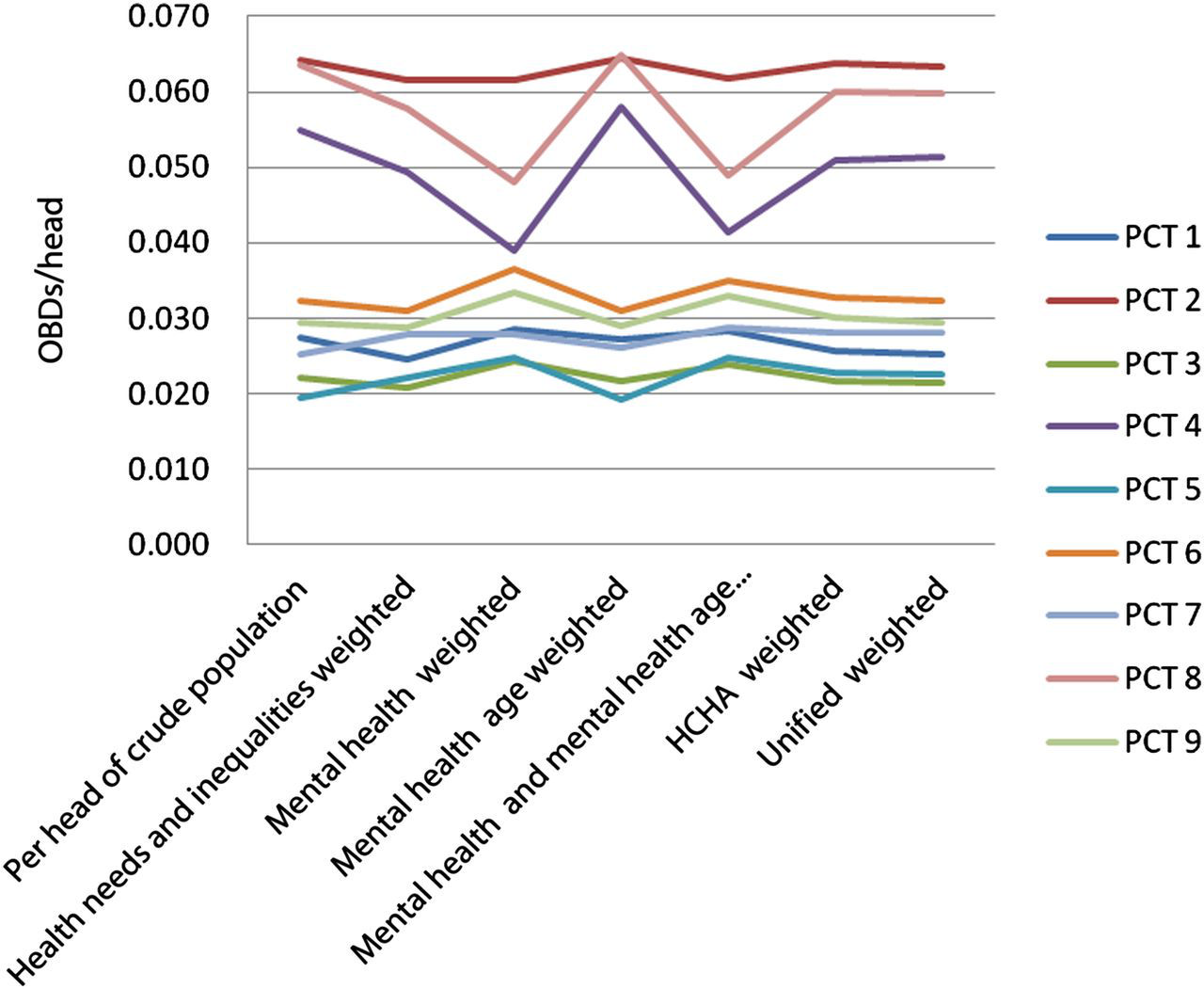
Z scores identifying outliers by OBD/weighted population
*Outliers
It was found that low secure occupied bed days is negatively related to spend on Assertive Outreach (r = −0.479, P < 0.05). To observe this relationship see Figure 4 Of the nine PCTs those which spent more per head on assertive outreach used less low secure occupied bed days. The scatter plot is given due to the small sample available, and while this relationship is suggested it cannot be said this factor is the direct cause of the reduction in low secure OBDs.
Low secure OBDs/assertive outreach investment per PCT
Noting the caveat about low numbers of completed episodes per PCT, Kendall's Tau was used to understand whether there is a relationship between length of stay and these categories of expenditure. No significant relationships were found between high, medium and low secure length of stay and any other forms of local mental health service investment. Similar to Figure 4 it has been found that there is a relationship between assertive outreach spend and spend on secure and high dependency services (r = −0.444, P < 0.01). That relationship can be observed in the scatter plot in Figure 5 The PCTs who spent less on assertive outreach spent more on secure and high dependency services. This is a possibility that warrants investigation using a larger sample than the nine PCTs.
Assertive outreach spend/secure and high dependency spend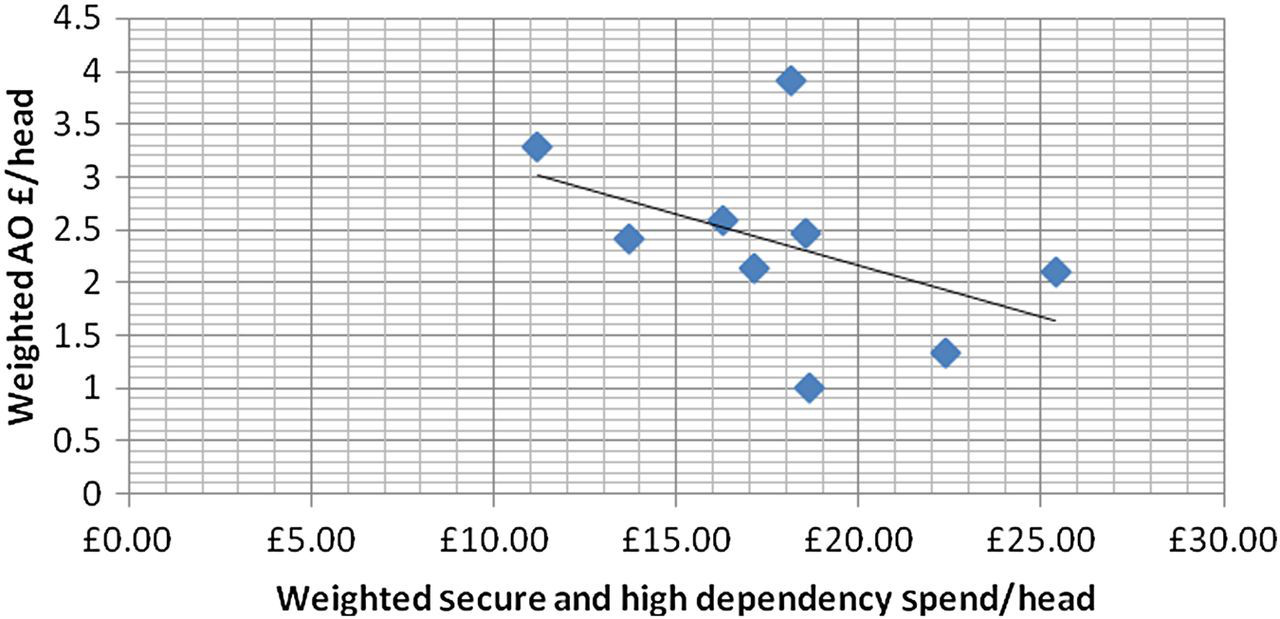
Other factors which may influence secure service (i.e. market forces, income, deprivation and education)
These factors were examined using the mental health- and mental age-weighted occupied bed days for each level of security and the income deprivation factor ID2004, market forces factor (MFF) and the standardized proportion aged 16–74 with no qualifications based on the 2001 census. Income deprivation domain (ID2004) includes a number of indicators, chosen to cover a range of economic, social and housing issues, into a single deprivation score for each small area in England. The focus of the overall MFF used is on the costs experienced by the providers. Education is considered using the standardized proportion aged 16–74 with no qualifications based on the 2001 Census.
Using Kendall's Tau (1-tailed) it was found there was a relationship between high secure bed use, and education (r = 0.487, P < 0.05) and income deprivation (r = 0.730, P < 0.01). The higher these factors per PCT the greater the high secure OBDs. It is though not possible from this to suggest that either factor directly causes the increase in high secure OBDs – although there is the possible relationship described. No significant relationships were found between these factors and low and medium secure OBDs (P < 0.05).
Limitations
The main limitation is acknowledged as the small sample of nine PCTs although that has been implicit in this form of local appraisal. It has been noted that statistical methods are more reliably used in larger samples and associated with this limitation the data have been provided transparently throughout the report. Care has been taken to use these methods for indication rather than asserting causation.
At the outset it was recognized that this review would not be able to use individual cases which in themselves would illuminate some of the qualitative experiences of both professionals and service users.
Conclusions
This review set out to understand the influence of wider services upon the care pathways for people using secure services. The purpose was to conduct an appraisal across one region, and reviewing the literature highlighted that this kind of examination had not been undertaken at a population level before. The literature highlighted that policy and services have been the focus of a great deal of modernization in the last decade and that this is still continuing. Also the literature highlighted variation in provision, reservations about the evidence base available to support procurement of the most effective interventions in some services, and variation in length of stay and expenditure underpinning this pathway. Within the context of growing demand, many features are suggested to influence the patient flows across the pathway that spans health and judicial systems.
A retrospective review of the pathway expenditure in the region highlights how growth and retractions have not been uniform across the nine PCTs and one can argue that this should be the case. The overall profile of the secure services used in the region shows a decline in high secure services and a growth in low secure. Associated with this there is no consistent profile of secure service use across the nine PCTs even when they are attributed to peer groups. In terms of pathway flows; medium and low secure length of stay in the region contrast favourably with other published data. However, it has only been in high secure services where the rate of discharge exceeds the rate of admission. Therefore, assuming that there is little or no intention to increase capacity in low and medium secure services an increased rate of discharge would be required. A particular area to consider is the numbers accessing low secure services from local services and the functioning of intensive care and step down services enabling discharge from low secure services.
City PCTs in the region consume more secure occupied bed days even when their use is weighted according to features and size of their population. Using population-weighted samples no one PCT features as a particularly low user (measured by occupied bed days) of any form of secure services, while two PCTs are high outliers for specific groups. In financial terms one PCT is a low outlier for its spend on secure and high dependency services and this same PCT is a high outlier in its spend on PD services. On considering relationships between wider mental health provision and secure service use it was found that PCTs in the region that spend more on Assertive Outreach used less low secure occupied bed days and spent less overall on secure and high dependency services.
The level of variation and complexity in patient and prisoner pathways has been acknowledged both in the literature and within these findings. Factors beyond the mental health services provided are acknowledged to have a possible impact upon secure services including education and income deprivation. These and other factors warrant consideration in wider public health policy.
DECLARATIONS