
Abstract
Walton Lillehei can be truly regarded as the ‘Father of Open-Heart Surgery’. His career demonstrates the virtues of tenacity and the ability to overcome adversity and opposition in the taking forward of significant innovation.
Introduction
Cardiac surgery, dating as it does from the 1940s, has been chronicled and discussed extensively. The developments in the field have been exponential and wide ranging, and reflect the contributions of many pioneers, who continued their endeavours in the face of cynicism and adversity, associated often with poor initial results. Indeed, one wonders whether present day research ethics committees would have allowed the unhindered progress of the specialty given its radical nature and the high mortality of many cardiac surgical procedures at the outset. Of these pioneers, one who must surely stand out among the others is Walton Lillehei, who made Minneapolis the Mecca for cardiac surgery in the 1950s and 1960s (Table 1). He was not only innovative but also responsible for training a large cohort of cardiac surgeons who went on to achieve prominence all over the world.
Original open-heart operations and techniques developed at the University of Minnesota, 1952–57
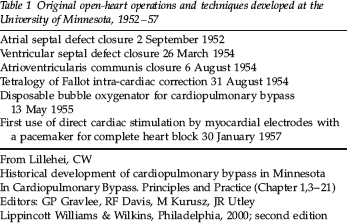
From Lillehei, CW
Historical development of cardiopulmonary bypass in Minnesota
In Cardiopulmonary Bypass. Principles and Practice (Chapter 1,3–21)
Editors: GP Gravlee, RF Davis, M Kurusz, JR Utley
Lippincott Williams & Wilkins, Philadelphia, 2000; second edition
I first came across Lillehei at Vellore, South India, in the late 1970s, where one of his trainees, Professor Stanley John, was the head of the cardiac surgery unit at the time. Here he delivered a highly inspirational talk covering his early contributions to cardiac surgery. Coming as it did with movie clips of operations performed employing controlled cross-circulation, and containing reference to trainees including Christiaan Barnard (1922–2001) and Norman Shumway (1923– 2006), it was exciting in the extreme to watch history in the making.
Unlike many of his peers who had reputations as prima donnas in the operating room, Lillehei was a man of calm composure and always kind and supportive to his assistants. His chief at the time, Owen Wangensteen, noted an instance when a visiting dignitary was viewing an open-heart operation from the gallery. Lillehei's assistant injured a coronary artery while opening the chest whereupon Lillehei calmly took over the conduct of the operation. The visitor remained blissfully unaware of the potential cause for catastrophe in the course of this operation.
Lillehei was single minded and took forward his innovation in the face of opposition and uncertainty. Questioning authority was his way to drive forward the frontiers of open-heart surgery. In later life he was able to describe cynically the four stages in the evaluation of a new treatment, as judged by responses from his peers, as: It will never work; It might work in selected cases; It is the treatment of choice; and, finally, I told you so!
Early days
Clarence Walton (Walt) Lillehei was born in Minneapolis on 23 October 1918, the eldest of the three sons of Dr Clarence Ingewald Lillehei (1892–1973), a dentist and Elizabeth Lillian Walton, a professional pianist, who lived in the southern suburb of Edina. In common with a significant proportion of the population of the state of Minnesota, the family was of Norwegian origin, the original name being Lille Heie. Jens Kristian Lillehei (1868–98), his grandfather, had emigrated to America from the island of Tysnes in Norway in 1885.
Walt's brothers, Dr James P Lillehei (b. 1923) and Dr Richard C Lillehei (1927–81) were also to become doctors, James an internist and cardiologist practising in St Paul, Minnesota, and Richard, a Professor of Surgery at the University of Minnesota, performing the first human pancreas transplant in 1966 and thereafter the first small bowel auto-transplant. Walt was educated at West High School, Minneapolis, from whence he graduated in 1935.
Early medical career
Lillehei attended the University of Minnesota from 1935 to 1939 and the University of Minnesota Medical School from 1939 to 1941. He went on to receive five degrees from the University of Minnesota: BS (with distinction) in 1939, MB in 1941, MD (Alpha Omega Alpha) in 1942, and MS in physiology and PhD in surgery, each in 1951. His doctoral thesis was on the role of cardiovascular stress in the pathogenesis of endocarditis and glomerulonephritis. 1
After serving as an intern in Minneapolis General Hospital from 1941 to 1942, he served in North Africa, Sicily and Italy from June 1942 to February 1946. He was commanding officer of the 33rd Field Mobile Army Surgical Hospital (MASH) Unit with the US Army Medical Corporations in North Africa and then directed a field hospital at Anzio in Italy. Initially holding the rank of First Lieutenant, he rose to become Lieutenant Colonel. He was awarded the Bronze Star Medal for meritorious service at Anzio, the European Theatre Ribbon with five battle stars, and the Bronze Arrowhead Award for amphibious operations (Table 2).
Awards and honours

Following his return to the USA, he was a Resident at the University of Minnesota Hospital in Minneapolis from 1946 to 1950, while simultaneously being a Research Assistant in Wangensteen's laboratory from October 1946 to December 1947. Owen Harding Wangensteen (1898–1981), Chairman of the Department of Surgery in Minneapolis from 1928 to 1967, and he set up one of the foremost surgical centres in the USA. He was an authority on perioperative fluid replacement and wrote a highly regarded book on intestinal obstruction. While his original contributions were more ephemeral and included gastric freezing for peptic ulcer, he served as a magnet in attracting a host of innovative and versatile talent under his wings, many of them returning to the USA after wartime military service.
As a Surgical Resident, Lillehei worked as an Assistant in the Physiology Research Laboratory of Maurice Visscher (1901–83) from October 1948 to September 1949. He found that the creation of large arterio-venous fistulae in dogs led to the invariable development of bacterial endocarditis and glomerulo-nephritis. He extrapolated these findings to the increased incidence of bacterial endocarditis in patients with congenital heart defects, including atrial and ventricular septal defects and patent ductus arteriosus. This provided a rationale for the surgical correction of these defects. By his own account, it was his period of research with Visscher that laid the foundations for his interest in cardiac surgery.
In 1941 he met a nurse, Katherine Ruth (Kaye) Lindberg, while working at Minneapolis General Hospital and they married in 1943. She graduated at the University of Minnesota on 31 December 1946. She was the only daughter of Swedish immigrants and grew up in Minneapolis. They had three sons and one daughter, Kimberle. Craig Walton Lillehei went on to practise as a paediatric transplant surgeon in Boston and Kevin Owen Lillehei as a neurosurgeon in Denver. A third son, Clark (1955–96), died of a brain tumour.
Lillehei's career was interrupted temporarily when he developed lymphosarcoma of the parotid gland. He underwent left parotidectomy, radical neck dissection and mediastinal exploration on 1 June 1950, one day after he completed his residency. The operation was performed by Wangensteen, assisted by Richard Varco (1912–2004) and John Lewis (1961–93), and was followed by radiation therapy. The operation involved a sternal split and lasted 10 hours and 35 minutes, with the transfusion of nine units of blood! He had originally detected a lump in front of his left ear while shaving late in 1949, and this was removed by the head and neck surgeon David State on 9 February 1950 and subsequently confirmed as lymphosarcoma (a form of non-Hodgkin's lymphoma).
Cardiac surgery at Minneapolis
Walt Lillehei served as Clinical Instructor from 1949 to 1951, Associate Professor of Surgery from 1951 to 1956 and Professor of Surgery from June 1956 to October 1967 at the University of Minnesota Medical School in Minneapolis.
The Variety Club of the Northwest donated to the University of Minnesota an 80-bed facility for paediatric and adult patients, and it opened its doors to patients on 1 July 1951. This was the world's first heart hospital devoted entirely to the medical and surgical treatment of heart diseases, providing the venue for major developments in open-heart surgery including Lillehei's own pioneering work (Table 1).
At the time, two major figures in cardiac surgery were working in Minneapolis and these were influential in developing Lillehei's own career. Clarence Dennis (1909–2005) had been working with dogs, in the process of developing a heart-lung machine, since 1945. The machine was first used in April 1951 on a six-year-old girl with a presumed diagnosis of secundum atrial septal defect. The results were unfortunate as it turned out subsequently that she in fact had an unsuspected atrioventricular canal defect. On 2 September 1952 F John Lewis (1916–93), after a period of laboratory research on dogs, successfully closed a secundum atrial septal defect in a five-year-old girl under direct vision using the caval inflow occlusion and moderate total body hypothermia. This was the first successful operation in the world to be performed within the open human heart under direct vision. 2
In 1952 Anthony Andreasen (d. 1986) and Frank Watson, working at the laboratories of the Royal College of Surgeons of England at the Buckston Browne Farm in Downe, Kent, found that isolation of the heart by occlusion of the superior and inferior venae cavae in dogs, while maintaining the patency of the azygos vein, prevented brain damage for up to 40 minutes of caval occlusion – the low flow azygos flow principle. Lillehei recognized the significance of this work for cardiac surgery. He repeated the experiments, introducing a single motor for the pumps of the pulmonary and systemic circuits to achieve a better balance. Along with Morley Cohen (b. 1914), he confirmed that the amount of blood flowing through the azygos vein was sufficient to maintain the vital organs undamaged for extended periods of time. 3
Lillehei believed that the risks of mechanical blood oxygenation could be avoided by the use of normal lung tissue, whether inpatient or donor, for blood oxy-genation. Cohen and Lillehei operated on dogs utilizing cardiac bypass, with one lobe of the lung, the cardiac lobe, as blood oxygenator. Warden and Cohen continued this work with experimentation with controlled cross-circulation in dogs. 4
Lillehei had to undertake controlled cross-circulation in humans in the face of strong opposition, especially from Professor Cecil Watson (1901–83), then Chairman of the Department of Medicine at the University of Minnesota. The general concern was that two individuals, one of them being otherwise healthy, were sharing an unquantifiable risk. The procedure was first used on 26 March 1954 when Gregory Glidden, 13 months old and a victim of repeated bouts of pneumonia and heart failure, underwent ventricular septal defect repair after being connected up to his father, Lyman Glidden. Perfusion was carried on for 13 minutes and the operation went smoothly, the defect being closed by direct suture. After initial good progress, the boy unfortunately developed pneumonia, dying 11 days later. The surgical team consisted of Lillehei, Morley Cohen, Herbert Warden (1920–2002) and Richard Varco. Between 1954 and 1955 Lillehei et al. used this procedure 45 times at the University of Minnesota, with infants or children as patients. A parent or a close relative with the same blood type was connected to the child's circulation. There were no donor fatalities and no long-lasting donor sequelae. Controlled cross-circulation was associated with the first total corrections of ventricular septal defect, Tetralogy of Fallot and atrioventricular canal defects. 5
Lillehei attended the autopsy of every patient dying at the hospital from a known or suspected heart defect, and he operated on the cadavers with a view to correct the defects found. He performed mock operations at autopsies on patients who had died with Tetralogy of Fallot, a constellation of congenital defects of the heart that led to the cyanotic congenital heart disease, presenting as a ‘blue baby’. On 31 August 1954 he went on to operate on a 11-year-old boy suffering from Tetralogy of Fallot. The child recovered uneventfully, went home two weeks later and went on to marry and have four children. In April 1955 Lillehei presented his experience with surgical correction of Tetralogy of Fallot to a meeting of the American Surgical Association at Philadelphia, with excellent results in the five survivors.
Vincent Gott, Richard DeWall, Morley Cohen and Herbert Warden collaborated with Lillehei in developing a pump oxygenator for cardiopulmonary bypass. Starting on 3 March 1955, the first of a series of five patients was operated on at the University of Minnesota for intra-cardiac repair of ventricular septal defects or transposition of the great vessels, by continuous perfusion from a reservoir of oxygenated blood.6, 7
On 13 May 1955 DeWall and Lillehei, based on their dog laboratory research, began routine clinical use of a simple disposable helix reservoir bubble oxygenator. De Wall, working as a laboratory animal attendant after being turned down for a residency in surgery, had developed a bubble oxygenator using the poly-vinyl plastic tubing procured from Mayon Plastics of Hopkins, Minnesota, which he formed into a spiral helical coil. All seven initial patients who underwent ventricular septal defect closure by August 1955, awoke postoperatively without evidence of neurological, hepatic or renal impairment. The DeWall-Lillehei bubble oxygenator was an instant success. 8
Lillehei first used retrograde coronary system perfusion for myocardial protection by coronary sinus can-nulation during an aortic valve operation on 31 January 1956. The perfusion lasted 11 minutes and the technique eliminated the risk of coronary air embolism.
Lillehei was a pioneer in cardiac valve surgery. On 29 August 1956 he performed mitral valve repair (annuloplasty) on a 15-year-old boy with mitral incompetence. 9 He undertook the first intra-cardiac aortic valve replacement in a 57-year-old woman in 1957 with a plastic prosthesis. He went on to be involved in the design of four cardiac valve prostheses: the Lillehei-Nakib toroidal disk (1966), the Lillehei-Kaster pivoting disk valve (1967), the Kalke-Lillehei rigid bi-leaflet valve (1968) and the St Jude valve.
Complete heart block was identified as a major cause of death in the first patients after ventricular septal defect closure. Lillehei and his group induced heart block in dogs by placing a suture in the atrial wall near the atrioventricular bundle, and he inserted a wire attached to an electric pacemaker directly into the right ventricle wall. By stimulation of the heart with low voltages at the desired rate, the heartbeat was restored and blood pressure rose to normal levels.

Lillehei and the heart
Lillehei implanted the first internal cardiac pacemaker. On 30 January 1957 William Weirich, working with Lillehei, first implanted an electrode in the ventricular myocardium of a three-year-old girl following ventricular septal defect repair. The electrode was attached to an external stimulator and the indifferent electrode buried under the skin. By early 1958 they had used this method 18 times with one death, caused by the indifferent electrode becoming unstuck from the skin; thereafter they inserted it under the skin. 10

Lillehei in characteristic pose
Early in 1956 Lillehei described to Earl Bakken (b. 1924) the problems associated with the large and cumbersome vacuum tube pulse generators that had to be kept plugged into an electrical outlet; Bakken was the electrical engineer whom the surgery department called in when electrical equipment in the operating room failed to work. At the time Bakken, in partnership with his brother-in-law Palmer Hermundslie, operated an electrical equipment business in a garage in northeast Minneapolis. They sold medical equipment to physicians and repaired television sets. Bakken went on to create a small, portable mercury battery-powered transistorized external pacemaker. In 1958 Bakken and Hermundslie incorporated their business under the name Medtronic, Inc, to manufacture the new pacemakers. The Medtronic 5800 pacemaker was launched for clinical use. By 1960 Lillehei et al. had used the Medtronic pacemaker to overcome complete heart block in 66 patients. After two to three weeks of continued electrical stimulation, the majority of patients regained a normal heartbeat. 11 By 1984 Medtronic Inc reported annual sales of $422.7 million and employed 5500 people.
Between 1951 and 1967 Lillehei trained 51 residents from the USA and 76 residents from 38 other countries in cardiac surgery. Most notable were Norman Shumway and Christiaan Barnard. He trained another twenty at Cornell from 1967 to 1979. Twenty-three of his trainees went on to become programme directors in cardiothoracic surgery. His departure from Minneapolis came about when he was bypassed for Chairmanship of the Department of Surgery by John Najarian (b. 1927), felt to be a more stabilizing influence, who went on to have a distinguished career as a transplant surgeon.
Cardiac surgery in New York
Lillehei was Chairman of the Department of Surgery, and Lewis Atterbury Stimson (1844–1917) Professor of Surgery, at Cornell University Medical Center from 1967 to 1970, and Surgeon-in-Chief from 1967 to 1970 and Attending Surgeon from 1970 to 1975 at New York Hospital.
He performed the first heart transplant on 2 June 1968 at New York Hospital Cornell Medical Center, followed by two more in January 1969. Deteriorating vision related to cataracts caused by radiation therapy for cancer led to the premature end of his surgical career at the age of 55.
Final days
Lillehei received many awards (Table 2). However, he was latterly under a cloud largely of his own making, being convicted of income tax evasion in February 1973. He was found guilty by a federal grand jury in St Paul, Minnesota, of omitting more than $250,000 from his tax returns for 1964 through 1968, and of owing more than$125,000 in taxes. This was presumably brought about by lax book-keeping procedures. He was placed on probation for five years by the USA Judge Philip Neville, and performed six months of ‘charitable medical services’ at Brooklyn Veterans Administration Hospital in New York City. It is believed that this misdemeanour may have prevented him from being awarded the Nobel Prize in Medicine for which he was nominated on several occasions. This was a difficult period, when he was ostracized by most of his professional colleagues throughout the USA and cold-shouldered at national meetings. A particularly noticeable snub was his failure to be invited to the Second International Symposium on Cardiac Surgery at the Henry Ford Hospital in Detroit, held on 6 October 1975 and which was attended by all the notable figures of American cardiac surgery of the period. The support and advocacy of John Kirklin (b. 1917), who had led to the other major contemporary cardiac surgical team in Minnesota at the Mayo Clinic, was crucial to the process of his rehabilitation.
Lillehei in later days
His Licence to Practise in Minnesota was restored in 1975 and he returned to practice in St Paul. He was Director of Medical Affairs at St Jude Medical, Inc, in St Paul, Minnesota, from 1970 until his death. The firm had been founded in 1976 as a medical equipment maker. In 1989 the C Walton Lillehei and Richard C Lillehei Professorship of Cardiovascular Surgery was established at the University of Minnesota.
Lillehei died of prostate cancer at his home in St Paul, Minnesota, on 5 July 1999. The Lillehei family established the Lillehei Heart Institute at the University of Minnesota in 2000 with a $13 million bequest. The Lillehei Heart Institute houses the C Walton Lillehei Museum, open to the general public. Another $3 million was used to establish the Katherine R and C Walton Lillehei Chair in Nursing Leadership at the university at the same time.
Footnotes
Acknowledgement
I am grateful to Dr Selwyn Vickers, Professor and Chairman of the Department of Surgery at the University of Minnesota, and to Cynthia De Kay of the Lillehei Heart Institute at the University of Minnesota for providing me with the photographs of Dr Lillehei. I am grateful to Professor Stanley John for his observations.