
Abstract
The achievements of the Hogarth Pringles, father and son, represent a remarkable story of surgical innovation; remarkable not only for the range and significance of their contributions but also because neither of them has been given appropriate recognition for their pioneering work. George Hogarth Pringle introduced antiseptic surgery to Australia. His son James performed the first autologous vein graft in Britain and the first excision with en bloc nodal dissection for malignant melanoma, both of which procedures were successful. He was also one of the earliest exponents of hindquarter amputation, was a national authority on fracture management and an early supporter of women in medicine.
George Hogarth Pringle was born on 22 December 1830 at Kintail in Ross-shire. His father James Hall Pringle (1801–73) was a tenant farmer at Hyndlee in the Scottish Borders, a farm described in Walter Scott's novel ‘Guy Mannering’. Other authors1–3 have suggested that George's mother Mary Hogarth (1803– 50) was related to William Hogarth (1697–1764) the artist and to Charles Dickens (1812–70). Examination of the relevant birth and death certificates 4 does not reveal any obvious relationship to either. Charles Dickens was married to Catherine Hogarth (born 19 May 1815), 4 the daughter of George Hogarth (1783–1870), a legal adviser to Sir Walter Scott. George Hogarth's father was a farmer in Berwickshire but not obviously related either to Hogarth the artist or to the Hogarth Pringles discussed here. 5 There is no reference in the 12 volumes of published letters of Charles Dickens to suggest that his wife was related to either William Hogarth the artist or Mary Hogarth (1803–50). 5 The fact that Catherine had a sister, also Mary Hogarth (1819–37), may have misled other authors into making the connection between the Hogarth Pringles and Dickens.
George Hogarth Pringle
While little is known about his early years or schooling, George Hogarth Pringle qualified MD from Edinburgh in 1853 for a thesis entitled Organic Stricture of the zUrethra; Complications and Effects. 6 He was appointed House Surgeon in the Royal Infirmary of Edinburgh under Professor James Syme (1799–1870) and Professor James Spence (1812–82).
A photograph of George Hogarth Pringle with his fellow residents in the Edinburgh Royal Infirmary in 1854 is shown in Figure 1. It is not clear why Joseph Lister simply signs his surname because he has not been ennobled at this stage but it may have been part of his Quaker tradition. The other doctors depicted here are worthy of mention. John Beddoe (1826–1911) went on to become Physician to Bristol Royal Infirmary and was elected to Fellowship of the Royal Society for his research work in anthropology. John Kirk (1832–1922) was Medical Officer and Botanist on Livingstone's Zambezi expedition of 1858–63; thereafter he became Medical Officer to the British Consulate in Zanzibar and was later appointed Consul. He was a moving force in ending the local slave trade and was influential in the building of the Zanzibar Anglican Cathedral that symbolically stands on the site of the former slave market. Joseph Lister (1827–1912) went on to make, arguably, the greatest contributions ever made to surgical practice with the introduction of antisepsis and of catgut sutures. Patrick Heron Watson (1832–1907) became a surgeon in the Edinburgh Royal Infirmary. Later Knighted, he became President of the Royal College of Surgeons of Edinburgh on two occasions, on the second presiding over its 400th anniversary. Although the most successful surgeon of his day in Scotland, Watson is thought to have been, by reason of his size and military bearing, Conan Doyle's model for Doctor Watson in the Sherlock Holmes stories.
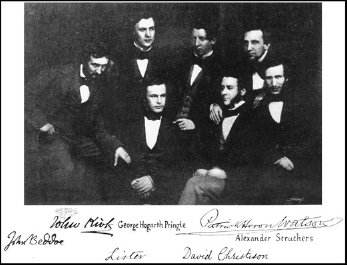
Joseph Lister and fellow residents, Royal Infirmary of Edinburgh, 1854
Alexander Struthers, (1829–55) brother of John Struthers, Professor of Anatomy in the University of Aberdeen, died at the age of 25 while serving as a Medical Officer in the Crimean War. David Christison, (1830–1912) son of Sir Robert Christison, went on to practise both as a physician and as an archaeologist.
George Hogarth Pringle left Edinburgh to serve as a Medical Officer in the Crimean War as a surgeon on a ship transporting the sick and wounded from the battlefields of the Crimean Peninsula to the base hospital at Scutari. Thereafter he worked as a ship's surgeon with the Cunard Company and then on the Peninsular and Oriental Company's ships between Suez and Sydney. In 1860 he settled in Parramatta in New South Wales. Parramatta, now part of greater Sydney and situated at the head of the Parramatta River, was proclaimed a city in 1788, the year of the arrival of the first fleet. It was here that the Governor's residence was established in 1799.
George Hogarth Pringle set up practice in George Street, Parramatta. His partner, a fellow Scot Dr (later Sir) Normand McLaurin (1835–1914), went on to become Chancellor of Sydney University. Pringle also worked with Dr Walter Brown (b. 1821), the first of three generations of Drs Brown to practise in Parramatta. The last of the three, Dr Keith McArthur Brown (d. 1962), wrote an account of medical practice in Parramatta that includes descriptions of Pringle's work. 7
Throughout his life George Hogarth Pringle continued to correspond with Joseph Lister and is credited with introducing antiseptic surgery into Australia. Pringle wrote a letter to the Sydney Morning Herald, published on 30 January 1868, which was essentially a case report describing the successful use of antiseptic principles for a compound fracture. This began: ‘Having at present under my care, what I may call a representative case of this form of treatment, the first, so far as I am aware in which it has been applied in the colony, I crave, in default of any local medical journal … ’ This assertion that there was no local medical journal was not entirely correct as the Australian Medical Journal had been founded in 1856 but he may not have regarded this as ‘local’ as it was published in Melbourne. His later case reports were published in the Australian Medical Journal.
He goes on to describe the treatment of a wound of the forearm sustained by the accidental discharge of a shotgun into an area some three inches above the left wrist joint: ‘I recommended immediate amputation,’ he wrote ‘more especially having the dread of secondary haemorrhage and lockjaw before my eyes; but neither the patient nor his relatives would consent to this, and begged for me to try to save the limb. I therefore, duly warning them of the manifold risks, resolved to try Professor Lister's plan’. After wound excision, he dressed the wound with a dressing soaked in carbolic, immobilizing the fracture with a fenestrated splint. He went on: ‘Suffice to say that in dressing the arm this morning, the 34th day from receipt of the injury, I find that the whole wound has completely healed up, thus converting a compound into a simple fracture. No pus whatever has appeared … firm union has taken place between the ends of the ulna and satisfactory progress made with the radius, perfect motion and sensibility retained in the hand’. He concluded: ‘Such are the astounding results of this method of treatment in the first case to which I have applied it. And be it remembered, this is no quack remedy, but the result of patient scientific enquiry and thought on the part of that “philosophical investigator” Joseph Lister’.
Pringle's decision to publicize this case in a newspaper was criticized in subsequent correspondence to the Sydney Morning Herald. Hugh 8 argues that Pringle's use of surgical and anatomical terminology suggests the article was directed at a medical readership and that Pringle's communication to the newspaper resulted in the rapid adoption of antiseptic principles by Australian doctors.
On a journey back to Britain he qualified to FRCSEd in 1870. George Hogarth Pringle died at the tragically young age of 41 years while on a further voyage to Britain in 1872 and was buried at sea 7 (Figure 2).

George Hogarth Pringle in Parramatta (reproduced from ‘Medical Practice in Old Parramatta’)
James Hogarth Pringle – early life
George's only son, James Hogarth Pringle, was born in Parramatta on 26 January 1863. Following the death of his father, he was sent to school at Sedbergh in Cumberland at the age of nine years, going on to study medicine at the University of Edinburgh from where he graduated in 1885. After graduation he was able to study surgical practice at three major European centres – Hamburg, Berlin and Vienna. This visit to European centres was later to prove important because he maintained links particularly with German, Austrian and Swiss surgeons, keeping up to date with their literature. 9 After serving as House Surgeon to Professor Thomas Annandale (1838–1907) in Edinburgh Royal Infirmary, he was appointed House Surgeon to Glasgow Royal Infirmary (GRI) under Sir William Macewen (1848–1924). In 1892 he was elected to the Fellowship of the Royal College of Surgeons of England and was appointed Surgeon to GRI in 1896. Although Macewen was to move his practice two miles from GRI to the Western Infirmary on his appointment as Professor of Clinical Surgery, Hogarth Pringle remained at GRI for the rest of his professional career.10, 11
James Hogarth Pringle was a true general surgeon and a surgical innovator across a wide range of surgical practice. He was first to make his mark in a way that was to prove unpopular with many of his contemporaries.
James Hogarth Pringle, champion for women in medicine
Medicine had remained an exclusively male preserve until the latter years of the 19th century. The Medical Act of 1876 allowed women to graduate with medical degrees from British Universities but opposition remained widespread. It was not until 1894 that Marion Gilchrist (1864–1952) became the first woman to graduate in medicine in Scotland from Glasgow University – shortly before women graduated in medicine from Edinburgh.
James Hogarth Pringle and Macewen were among the few senior figures at that time who were sympathetic to their cause, readily accepting women students into their clinics. 12 Some of these were to become well-known figures in later life including Louise McIlroy (1874– 1968), Elsie Inglis (1864–1917) and Helen Wingate (1895–1985). Pringle was appointed Lecturer in Surgery and Demonstrator in Anatomy to Queen Margaret College, which had been established for women students and opened in 1883, six years before the first women began medical studies. He had started to teach women's medical classes in 1890 before instruction in the medical school and the wards of the hospitals were opened freely to women. Queen Margaret College was incorporated into Glasgow University in 1895.
Some of the women whom Pringle taught and took on as House Surgeons went on to distinguished careers in medicine. Louise McIlroy graduated MB ChB in 1898 and MD with commendation in 1900. She was appointed Gynaecological Surgeon to the Victoria Infirmary in Glasgow and served with the Scottish Women's Hospitals in France, Serbia and Salonika in the First World War. After the war she was appointed Professor of Obstetrics and Gynaecology at the London School of Medicine for Women, the first woman appointed to a medical chair in the UK, and appointed Dame of the British Empire in 1929. Elsie Inglis studied medicine at the Edinburgh Medical College for women but, since clinical teaching for women was not then available in Edinburgh, she travelled for this to Glasgow where she was taught by Macewen and Pringle. She went on to found the Scottish Women's Hospitals of the First World War.
Fracture treatment
While James Hogarth Pringle had a very broad range of surgical interests, he made a particular study of the treatment of fractures. He was at an advantage in this regard as a result of the early and widespread use of X-rays in GRI that allowed him to gain wide personal experience of fractures and their management. His colleague John Macintyre (1857–1928) had established the world's first X-ray service for patients in GRI in March 1896. Shortly after his discovery of X-rays, Roentgen sent the original paper to three colleagues in various parts of the world, one of whom was Lord Kelvin in Glasgow. Kelvin shared the paper with three others, including Macintyre, an ENT surgeon but also the medical electrician at the GRI. Within weeks of receiving the paper, Macintyre and his colleagues had built an X-ray apparatus, taken their first X-ray and within months had established the first hospital X-ray department in the world. 13 This allowed James Hogarth Pringle an early, perhaps unique, experience in fracture diagnosis and management using X-rays, and his book on fractures and their treatment became a standard textbook for a generation in Britain.
He had the added advantage of working in the hospital where Lister had first introduced antisepsis and would surely have been aware of his own father's work on antisepsis. He was an early exponent of aseptic technique. Both of these factors undoubtedly contributed to his expertise and success with fracture management.
As surgical chief it was his practice to operate on virtually all of the patients admitted to the wards under his care and the results were impressive. In an analysis of 230 cases of open fracture of long bones treated by operative methods 14 his patients clearly benefited from his rigorous observance of aseptic technique. ‘There are few cases,’ he wrote ‘which afford a better test of aseptic methods’. But it was his policy of fixation of long fractures in an age when treatment by traction was the norm that marked him out as a pioneer: ’ … In every case,’ he wrote ‘I have employed some form of “fixation” of the bone fragments; the “fixation” being effected in some instances by wiring the main fragments, in others by the use of ‘plates’ and in others generally in the case of a small fragment (e.g. a portion of an articular surface) which has been fractured off and the use of a screw to fix the small to the large segment of the bone.’
His total reliance on external fixation was perhaps 50 years or more ahead of its time. ‘In my practice,’ he continues ‘plaster cases have rarely been employed during the early stages’. 14
In this series his amputation rate for sepsis was 2.6%, a dramatic reduction on the norm for the time. There were no cases of tetanus. In 1910 he published Fractures and their Treatment 15 where he wrote: ‘I fix most of the open fractures that I have to treat’. Several surgeons who reviewed the book were critical of this practice but Pringle was resolute, writing in his 1914 paper: 14 ‘I have not seen any reason for departing from [this practice] … I believe that these methods give better results’. In his treatment of other fractures he devised a series of splints and plasters, many of which were reproduced in his textbook. Among innovative splints that he devised was an adjustable inclined plane splint for lower limb fractures.
For the remainder of his life Pringle continued to work on methods of treatment for fractures and dislocations. His casebooks, preserved in the archive of the Royal College of Physicians and Surgeons of Glasgow, 16 show his methodical approach. Case reports are accompanied by detailed ink drawings that he coloured. These are supplemented by postmortem studies and drawings showing skull fractures, hip fractures and hip and shoulder dislocations. The history in each case is recorded according to his structured classification, and his thoughts on the mechanism of the injury and its treatment are appended. These show him to be a keen observer and gifted artist, an organized and methodical record keeper with an enquiring mind.
Hindquarter amputation
James Hogarth Pringle was also a pioneer of hindquarter amputation, a radical operation involving division of the pubic symphysis and the sacroiliac joint. This was first successfully performed by Girard of Berne in 1895 as a two stage procedure. 17 Pringle performed the first successful such amputation in Britain in 1900 for tuberculosis of the hip that had spread to the pelvis. 18 He was the first in the world to perform the one-stage procedure for sarcoma of the thigh. It is all the more impressive that he performed these procedures under spinal anaesthesia with the local anaesthetic stovaine and performed the operation in some 50 minutes. At the time this was a remarkable surgical tour de force, which surgical giants such as Billroth (1829–94), Jaboulay (1860–1913) and Kocher (1841–1917) had attempted without success. In 1916 Pringle was able to publish a review of 19 such operations with an early mortality of 68%. 19 This radical, technically challenging and risky procedure was described by Sir Gordon Gordon-Taylor (1878–1960) as ‘one of the most colossal mutilations practised on the human frame’. The size and relative success of Pringle's series may be judged by the subsequent experience of Gordon-Taylor, widely regarded as a pioneer of the technique. Gordon-Taylor first attempted the procedure in 1922 but did not perform a successful procedure until 1929. In 1934 he reported success in three out of five procedures attempted. Gordon-Taylor, whose name is more widely associated with the procedure, was generousin his praise of Pringle's technique and results. 20
Head injury
As a young doctor Pringle had training in ophthalmology at Moorfields Hospital in London and throughout his life continued to make use of the skills he had learned there including fundoscopy. It was inevitable he should develop expertise in head injury, having worked as assistant to Macewen, a pioneer of neurosurgery who, in 1893, had published results a series of 24 operations for cerebral abscess of whom 23 recovered. Pringle's casebooks 16 demonstrate the standard skull charts he devised for the recording of head injuries and the precise site and extent of skull fractures. Here too are recorded the levels of consciousness, meticulous neurological examinations and appearances on fundoscopy, which he had performed in such cases. These casebooks, neatly written and with meticulous coloured illustrations, offer an insight into the mind of a surgeon who was both painstaking and methodical.
Malignant melanoma
In 1908 James Hogarth Pringle published the first description of en bloc excision for malignant melanoma, reporting the procedure in two patients. 21 Some 30 years later he was able to publish a follow-up reporting two of these cases alive and well, 30 and 38 years on. 22 He included original photographs showing the en bloc excision in the axilla and inguinal regions (Figures 3 and 4).

Patient showing scar after excision of melanoma with inguinal block dissection

Patient showing scar after excision of melanoma with axillary block dissection
‘A radical extirpation of the disease,’ he wrote in the 1908 paper ‘will be most certainly ensured by excision of the tumour with a good zone of healthy skin around it … with a broad strip of the subcutaneous fascia up to and including the nearest anatomical group of glands at least; and all that is removed should be in one continuous strip … ’ This description of en bloc excision remains the basis for modern surgical practice. He continued: ‘I have not seen any description published of any patient operated upon in a manner similar to that here described but it seems to me to be a method indicated by the life history of these tumours’. His seems to have been truly the first description of what was to become an accepted surgical treatment.
Reconstructive arterial surgery
James Hogarth Pringle was also the first surgeon in Britain to carry out a free vein graft. Alexis Carrel (1873–1944) in 1905 had been the first to describe arterial anastomoses in animals 23 and in 1906 the Spanish surgeon José Goyannes Capdevila (1876–1964) used an in situ graft of popliteal vein to bypass a popliteal aneurysm, 24 the first recorded vein graft in man. The following year Lexer (1867–1937) in Germany performed the first free vein graft in man, using a segment of saphenous vein to restore arterial continuity following excision of a traumatic axillary aneurysm. 25 Pringle, who continued to read the German literature, was the first to perform free vein graft in Britain. He did this using a saphenous vein graft to restore continuity after excision of a syphilitic aneurysm of the popliteal artery and characteristically in this paper he duly acknowledged the ‘splendid work of Carrel’. 26 The technical quality of his surgery is demonstrated by this excerpt from his description of the first case: ‘The proximal clamp was removed and at once blood rushed through the graft. Not one drop of blood escaped at either of the lines of suture and distal pulses were instantly restored’.
The patient recovered and resumed work but died three years later of syphilitic aortic valve disease. The saphenous vein graft was recovered at autopsy and found still patent. These specimens (Figures 5 and 6) are on display in the Museum of the Royal College of Surgeons of Edinburgh.

Specimen of excised popliteal artery with aneurysm. The white rod indicates the position and relative size of the artery (reproduced courtesy of The Royal College of Surgeons of Edinburgh)

Patent saphenous vein graft removed at autopsy two years postoperatively
Pringle's manoeuvre
Yet it is for Pringle's manoeuvre that his name is known throughout the surgical world. The technique of occluding the portal triad to control haemorrhage in liver trauma, which he described in the Annals of Surgery in 1908, 27 is still widely used in modern hepatic surgery. That paper attests to the originality and logic of his thinking, often flying in the face of mainstream opinion. In describing his experience in dealing with liver injury he observed that portal triad occlusion controlled the bleeding from the liver sufficient to allow suturing or packing. Yet other authors, including the authoritative Carl Langenbuch (1846–1901), 28 had been wary of using the manoeuvre as apparently it had resulted in the death of experimental animals. Pringle repeated the experiments on rabbits, clearly showing not only that the technique could control bleeding but that the animals survived. Reassured, he used the technique clinically at a laparotomy for liver trauma. ‘An assistant,’ he wrote, ‘held the portal vein and the hepatic artery between a finger and thumb and completely arrested all bleeding’. 27 As a result of this experience, the animal studies and postmortem studies, he felt able to recommend it to other surgeons. It remains in standard use over a century later.
James Hogarth Pringle retired from GRI in 1923 at the age of 60 and was elected Visitor (Vice President) of the Faculty of Physicians and Surgeons of Glasgow in that year (Figure 7). He died at his home in Killearn in 1941 at the age of 78. 4
James Hogarth Pringle by William Dring
Pringle, father and son
Why did the pioneering work of these two surgeons not gain wider recognition? In the case of George Hogarth Pringle, had he published his work in a medical journal and had he lived for longer, it seems reasonable to speculate that his contribution might have been more widely known and received greater appreciation.
As for James Hogarth Pringle, other authors have suggested it may have been because he tended to work alone. 3 Of the 54 papers he wrote between 1887 and 1940, only two, one of these his last, had an additional author. One obituary 11 describes ‘a certain austerity of manner’ and a ‘lack of the gift of fluency in public speech and writing’ while another 10 talks of ‘a rather abrupt manner and a fierce expression’. Perhaps because of these characteristics he did not cultivate a school of young academic surgeons who could promote him and his ideas, although those who worked with him were intensely loyal.
Both father and son made important contributions to surgical practice that deserve greater recognition than they have enjoyed to date.
Footnotes
Acknowledgement
It is a pleasure to acknowledge the help in the preparation of this article from the following: The library staff at the Royal College of Surgeons of Edinburgh; Marianne Smith, Steven Kerr, Andrew Morgan; Andrew Connell in the College museum; Carol Parry, Archivist, Royal College of Physicians and Surgeons of Glasgow; Alistair Tough, Archivist, University of Glasgow Archive; and Tom Hugh whose paper on George Hogarth Pringle did so much to stimulate interest in the topic.