
Abstract
In an era when few women achieved consultant surgical status, Miss Forrester-Brown proved not only a pioneer orthopaedic surgeon but also demonstrated that her sex was no bar to this physically demanding specialty. Virtually on her own she consolidated a series of clinics throughout three counties, elevating the Bath and Wessex Orthopaedic Hospital to national prominence. In addition to her books and journal communications, she maintained strong links with distinguished orthopaedic surgeons in Europe and America to keep abreast of innovations beneficial to her patients. Yet her shoulder was not always at the wheel, for she enjoyed horse-riding, ski-ing and swimming, and she was deeply interested in literature and art.
Early years
Since Miss Forrester-Brown MD MS (Figure 1) did not marry and appears to have had no near relatives or descendants, little is known about her family and early life. She was born to James Samuel Brown, Civil Engineer and Emma Laetitia Brown (née Tomkins) on 15 November 1885 at Wyverndern, The Ridgeway, Enfield, North London
1
and named Maud Frances. Subsequently she spent some of her childhood in India.
2
Maud Forrester-Brown at about 50 years (reproduced courtesy of the British Orthopaedic Associaton)
In March 1898 she became a pupil at Bedford High School with the name Maud Forrester Brown; the origin of Forrester has not been determined. She matriculated in preliminary sciences of London University in June 1904 and left school in September 1906. A later reference letter by her headmistress, Miss SM Collie, stated that she was one of her most brilliant and well-balanced scholars. 3
In September 1906 she applied for entrance to the London (Royal Free Hospital) School of Medicine for Women with a short testimonial from Miss Collie reporting she had spent eight years at Bedford High School and recommending her admission. Her hand written application form gave her name as M Forrester Brown of 17 Leinster Square, Bayswater, her age as 20 years 10 months and the address of her parent, guardian or nearest relative as ‘JS Brown Esq, Consulting Engineer to Government Bombay’. 4 Clearly her father had not added Forrester to his name and it was not until the summer of 1907 that she hyphenated her name in the Medical School records as Forrester-Brown, the surname she assumed permanently thereafter. In September 1906 she took an entrance scholarship examination at the School of Medicine, finishing top of four candidates, the subjects being Latin, English, Euclid, Arithmetic and Algebra; evidently biological and scientific subjects were not taken. 5 She was awarded a School Scholarship.
Surviving records of the examinations taken by Miss Forrester-Brown at the School of Medicine for Women indicate that, of some eight to 10 students, she performed well and was placed first in Physics, second in Practical Inorganic Chemistry, shared first in Biology, first in Histology, second in Practical Anatomy, first in Practical Physiology, second in Pharmacology and first in Midwifery yet only fourth in Surgery. Generally she excelled at practical subjects and won several prizes. 5 At the London University MB BS examination in 1912 she passed with Honours in Pathology and Forensic Medicine, and then pursued postgraduate courses at the Brompton Hospital, the National Hospital and Queen Charlotte's Hospital, all in London, and also at the Victoria Infirmary, Newcastle–upon-Tyne (her application omitted the word ‘Royal’). 3 On the award of a Gilchrist Studentship of London University, she went to Berlin to attend special courses in surgical anatomy, radiology, paediatrics, cystoscopy and operative gynaecology. 3 Finally, she attended an obstetric course in Glasgow. 2 In 1914 she gained an MD London with gynaecology as her subject. 3
Junior clinical experience
She continued to be adventurous when selecting junior hospital posts from as far apart as London and Dundee, successively being house surgeon at the Samaritan Hospital, Glasgow, house surgeon at Dundee Royal Infirmary, house physician at the Royal Free Hospital, London, house surgeon at Liverpool Royal Infirmary, house surgeon to Sir Harold Stiles (1863–1946) at the Royal Hospital for Sick Children, Edinburgh and senior resident at the Royal Infirmary Sheffield.
3
Her stay in Sheffield was cut short in October 1916 and her subsequent career shaped by an invitation from Sir Harold Stiles to join him as orthopaedic resident at the Edinburgh War Hospital, Bangour, where he established a unit treating injuries sustained by soldiers wounded in World War I. Sir Harold was a general surgeon and pioneer paediatric surgeon familiar with bone and joint tuberculosis and the traumatic problems of civil life including fractures and dislocations. However, at the War Hospital he was challenged by complex gunshot wounds, including nerve injuries of which a special study was undertaken with the able assistance of Miss Forrester-Brown. When Stiles resigned from the War Hospital in 1919, Miss Forrester-Brown was described as Surgeon to the Edinburgh War Hospital, being responsible for 300 beds with the assistance of Royal Army Medical Corps officers whom she supervised. When this hospital closed in 1921, Stiles and Forrester-Brown produced a book entitled Treatment of Injuries of the Peripheral Spinal Nerves of which he wrote part two and she wrote parts one and three.
6
She also performed two of the six nerve repairs detailed in the illustrative case observations and was responsible for the preliminary drawings of the many operative techniques figured. A footnote at the end of the book reads: The illustrations have been made by the artist from drawings done at the time of the operations by one of the authors (M.F.B.)
During the 1914–18 War, Bangour was visited by Sir Robert Jones (1858–1933), Director of Army Orthopaedic Services and a personal friend of Sir Harold. There seems little doubt the charisma and specialty of Sir Robert had persuasive influence with Miss Forrester-Brown and, indeed, after the war she attended his orthopaedic clinics in Liverpool and Oswestry. She also visited Oxford to observe the work of GR Girdlestone (1881–1950) who was to become the first Professor of Orthopaedic Surgery in the UK in 1937 (the Girdlestone operation consists of excision arthropalsty of the hip for tuberculosis).
Meanwhile in 1920 she published, ‘Difficulties in the diagnosis of nerve function’ 7 and ‘The possibilities of end-to-end suture after extensive nerve injuries’. 8 Also in 1920 she passed the Primary Fellowship Examination of the Royal College of Surgeons of England 3 and yet, for unexplained reasons, never proceeded to the Final Fellowship. Meanwhile in 1920 she became MS (London) with a thesis entitled The results of operations for peripheral nerve injury. 3
In 1921 she wrote a chapter on the result of operations for nerve injury in Orthopaedic Surgery of Injuries edited by Sir Robert Jones 9 and in the same year ‘Study of some methods of bone grafting’ 10 based on the extensive experience at Bangour of open fractures complicated by sepsis, demonstrating that nerve trauma was but part of her responsibilities; she favoured a two stage operation, excising scars and controlling infection before bone grafting, illustrating this with 26 case histories.
After the war Miss Forrester-Brown worked in Dundee, one of her appointments being Visiting Orthopaedic Surgeon to Fairmuir Specialist School. She was now often invited to lecture, stimulating further publications including, ‘Sacro-iliac strains’ and ‘Some modern methods in the treatment of bone and joint tuberculosis’. 11
In June 1923 she was awarded the William Gibson Research Scholarship (donated by his widow Maud Gibson of Melbourne and exclusive to women doctors) of the Royal Society of Medicine, London, holding this for three years and enabling her to visit orthopaedic clinics in the USA, Italy, France, Norway, Sweden, Denmark and many centres in Britain. She compiled detailed reports of these visits,
12
describing many methods and equipment introduced subsequently into her practice in Bath. She was interested particularly in appliances and splints used by Vittorio Putti (1880–1940) of Bologna (the Putti-Platt reconstruction for recurrent shoulder dislocation is named after him) and JE Goldthwait (1866–1961) of Boston, USA, in sunlight methods for bovine tuberculosis used in Switzerland and in gymnastic exercises employed in Swedish and Danish hospitals, translating their brochures into English for her physiotherapy staff.
12
After the Scholarship lapsed she continued regular visits abroad; Stirling commented:
2
Miss Forrester-Brown spent one vacation every year visiting orthopaedic clinics. There must be few in Europe who did not at one time or another entertain this avid enquirer, and few who did not gain from her visit.
The Bath and Wessex Children's Orthopaedic Hospital
Until 1924 orthopaedic patients in the West Country were under the care of general practitioners and, for in-patient treatment, general surgeons with an interest in what was still an emerging specialty. At Bath an orthopaedic clinic was established in the city in 1922 under the care of two general surgeons, WG Mumford (1870–1955) OBE FRCS, and JS Levis (1888–1943) MC MB of the Royal United Hospital, who became the first surgeons to the Children's Orthopaedic Hospital when it was opened officially by the Duke of Connaught in May 1924, with 20 beds. Specialist orthopaedic expertise was provided for complicated cases by Sir Robert Jones and GR Girdlestone who were appointed Honorary Consultant Surgeons; since 1919 they had been instrumental in promoting a national scheme of orthopaedic hospitals via the Central Council for Crippled Children and it is assumed they supported Miss Forrester-Brown strongly for appointment as Resident Surgeon, noted in the first Annual Hospital Report dated 1924. 13 Her own statements confirm she started work in Bath in May 1925 and in the second Annual Report was named the Resident Medical Officer and Visiting Surgeon to Clinics. 14 Her residence was at 22 Combe Park, across the road from the Hospital and later she rented rooms in the Circus for private consultations. Beds were shared equally with Mr Mumford and Mr Levis although, as she had responsibility for a growing number of children's clinics throughout Somerset and Wiltshire, she acquired a major proportion of the beds. By 1926 the original 20 beds had increased to 72 and Miss Forrester-Brown was attending clinics in Somerset at Taunton, Weston-Super-Mare, Bridgwater, Yeovil, Radstock, Frome and Glastonbury, and in Wiltshire at Corsham, Salisbury, Swindon and Trowbridge; 14 a clinic at Devizes, first established by GR Girdlestone, came under the care of Messrs Mumford and Levis, as did the clinics in Bath itself.
In 1924 only 51 operations were performed, increasing rapidly to 140 by 1926 and to 237 by 1927. Expansion continued especially with the addition of Dorset to the Hospital's responsibilities and by 1930 Miss Forrester-Brown was termed Visiting Surgeon to the Bath, Somerset and Dorset Central Children's Orthopaedic Hospital and Visiting Surgeon to the Clinics, predominantly in Somerset and Dorset. 15
Former staff told this author that she would disappear into Dorset for a week at a time, allegedly on horseback, visiting Dorchester, Weymouth, Bridport, Sherborne, Wimborne and the Red Cross Children's Hospital in Swanage; Robert Robins FRCS, orthopaedic house surgeon in 1947, notes this was known as her ‘out-week or away week’. 16 In 1931 the original long title of the hospital was shortened to The Bath and Wessex Children's Orthopaedic Hospital and a special unit of 20 beds for babies was opened. At this time, throughout three counties, 14 major clinics were visited monthly or quarterly by surgeons and 14 minor clinics were established for follow-up purposes and visited by after-care sisters and later by orthopaedic physiotherapists. 17
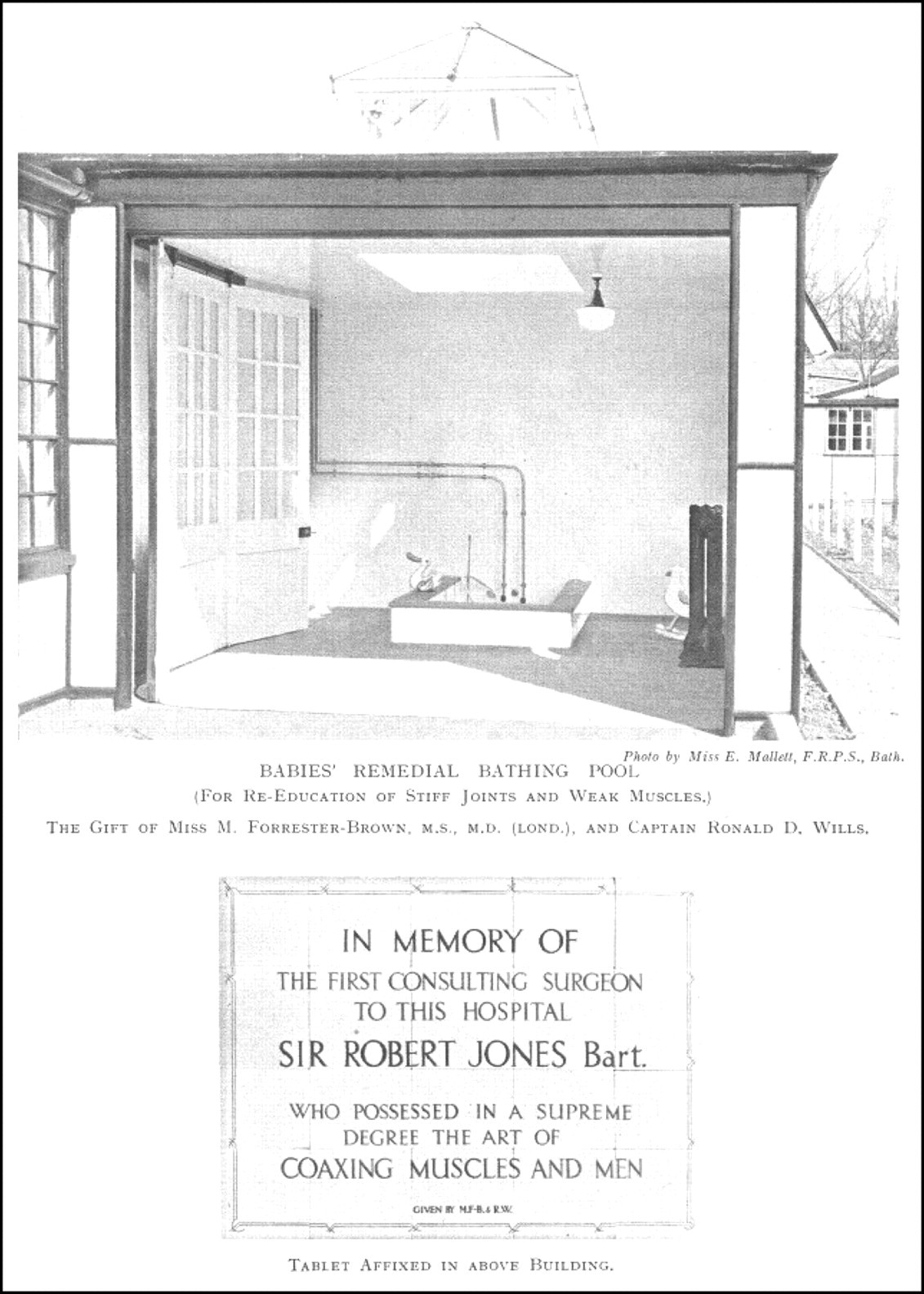
In 1934 WG Mumford retired, followed by JS Levis in 1935 when John Bastow MD FRCS (1906–64) was appointed Second Surgeon and Visiting Surgeon to the Clinics of Wiltshire, Miss Forrester-Brown becoming Senior Surgeon and Visiting Surgeon to the Bath, Somerset, Dorset and Swindon Clinics. John Bastow, an energetic Australian who trained at the Dame Agnes Hunt and Robert Jones Hospital in Oswestry, also had appointment to the Royal United Hospital, Bath with responsibilities for adult orthopaedic problems and trauma; indeed he and Charles Kindersley FRCS, a general surgeon, initiated the first fracture clinic service in the South West of England. Although Miss Forrester-Brown never dealt with acute traumatic cases, gradually she took increased responsibility for adult orthopaedic cases, especially former children under her care. During 1935 Captain Ronald Wills provided an annexe to the babies ward in which a remedial pool was housed, being donated by Miss Forrester-Brown and dedicated by her to Sir Robert Jones who had died in 1933 (Figure 2).
18
Pool and plaque for babies ward, Bath & Wessex Orthopaedic Hospital, 1934
18
With the outbreak of World War II, the Orthopaedic Hospital was designated suitable for acute surgical and medical cases under the Emergency Hospital Scheme and extra beds were arranged and used by military personnel in the gymnasium, board room and out-patients' room. Fortunately, these were no longer required after September 194218 for, in the meantime, the demand for children's beds had intensified and extra accommodation for recovering patients was arranged at Southstoke House near Bath. During the Baedeker air raids on Bath in 1942, patients were placed under their beds that were reported to be ‘nearly as robust as Morrison shelters’. Happily, the Hospital was only slightly scarred and no one injured.
19
In the 1930s a house surgeon was appointed and this post was usually given to graduates of the Royal Free Hospital, although under war-time conditions none was available. After the war, the number of Visiting Physicians increased to four and Visiting Anaesthetists to five. Meanwhile Miss Forrester-Brown and John Bastow were attending 21 children's clinics periodically (Figure 3) and performing more operative surgery as emerging antibiotic cover diminished risks and improved cure rates of bone and joint diseases; in addition, 10 clinics were undertaken by after-care sisters.
20
Robert Robins, appointed House Surgeon in August 1947, has vivid memories of Miss Forrester-Brown's operating sessions:
She was a dab hand with a Thomas' wrench for relapsed club feet: ‘mush it up’ was her advice. She never picked up a vessel unless it could be done with Ochsner's forceps and ligated with chromic catgut of her own manufacture. Before closing a hip operation she would empty a galley pot of neat iodine into the wound. She would not allow her patients to have a blood transfusion, even after a Hibbs' fusion for scoliosis (‘overlap the bones like “shlates” on a roof') or an arthrodesis of the hip but the surgeon of today may be unaware of the efficacy of a plaster spica in securing haemostasis and counteracting shock.
16
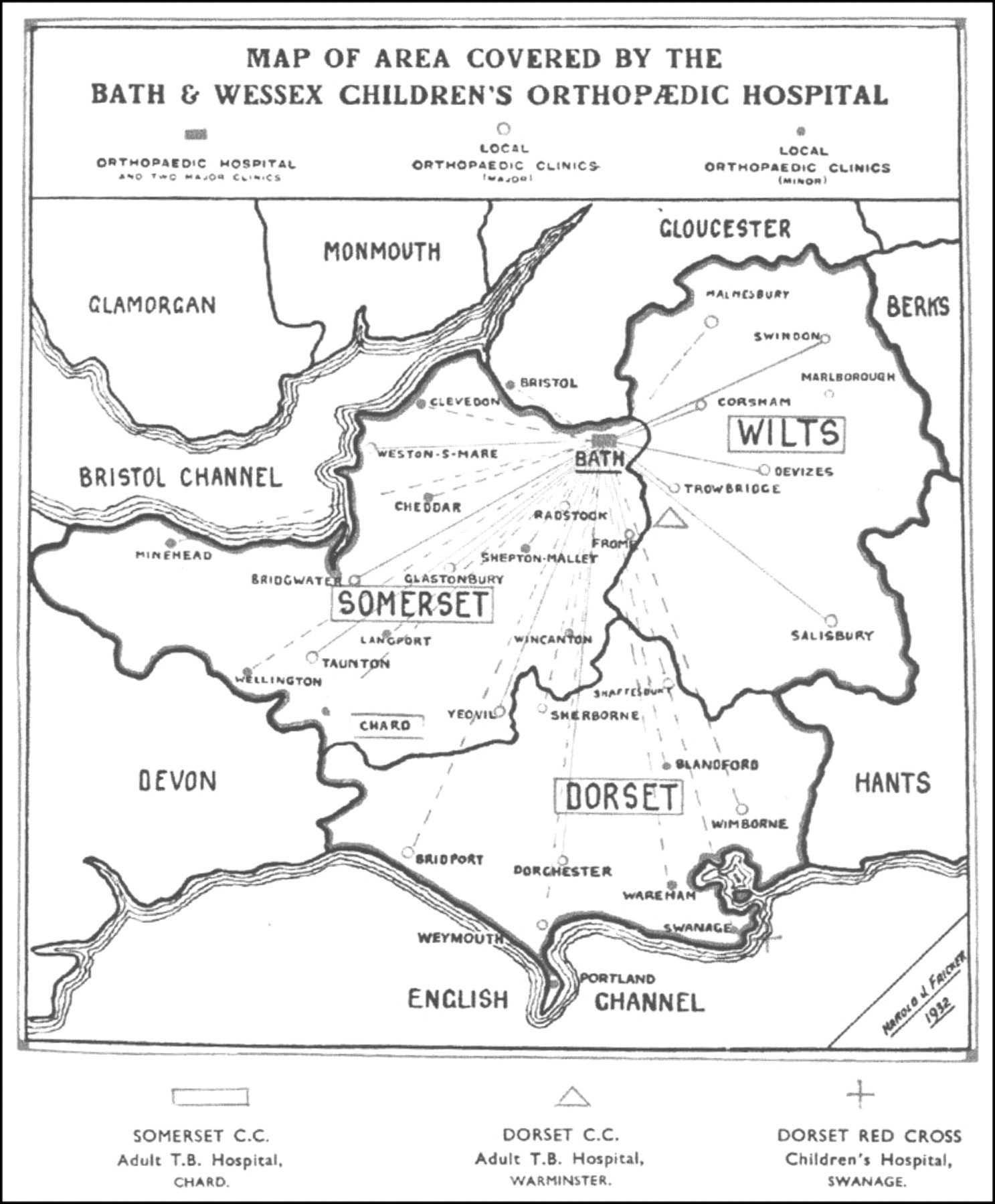
Map of clinics dependant on Bath & Wessex Children's Orthopaedic Hospital, 1939 (Annual Report ending 31 March 1940)
The 22nd and last Annual Report, 31 March 1947, noted the passing of the National Health Service Act and its implementation on July 1948, coupled with an appeal for supporters to continue subscriptions and donations until the new arrangements were in place. 20 Miss Forrester-Brown was then termed Consultant Orthopaedic Surgeon until her retirement in December 1950, aged 65, by which time two further orthopaedic surgeons had joined John Bastow. In retirement she returned to Edinburgh to assist Sir James Learmonth's investigations into the repair of peripheral nerves and she was a frequent visitor to the Princess Margaret Rose Orthopaedic Hospital, contributing to discussions and ward rounds. In 1954 she worked as a locum in Huddersfield, in Kirkcaldy and at other orthopaedic centres. Then she went to South Africa as temporary orthopaedic surgeon at the Holy Cross Hospital, East Pondoland in the Transkei where clinical problems resembled those she had experienced in her early career. 2 Retaining Edinburgh as her base, she continued to travel and to attend and participate in meetings and conferences; at a congress of the British Orthopaedic Association, in her late 70s, the writer recalls one session when she stood up to question or, more often to instruct, practically every speaker.
Clinical experience and further publications
The Annual Reports of the Hospital are largely concerned with financial matters, lists of subscribers, donors, collections, annual accounts, a school report, a workshop report, a needlework guild report (up to 30 voluntary centres throughout the three counties supplied clothing for children in hospital), and also brief statistics of clinic, physiotherapy and dental attendances. Until 1936 the medical reports were brief although they always provided hospital admission statistics under the same diagnostic headings, reflecting the hospital practice of Miss Forrester-Brown. These statistics do not separate new cases from readmissions, apart from occasional observations, for example in 1936 when of a total of 82 cases of poliomyelitis admitted, 25 were fresh each requiring an average stay of 174 days. 21 Most years, congenital deformities formed the largest diagnostic group followed closely by surgical tuberculosis and infantile paralysis (poliomyelitis). Rickets remained a lesser problem as late as 1947, surprisingly so for an essentially rural area where children were exposed to sunlight and the consumption of fresh milk enriched with vitamin D; unfortunately unpasteurized milk was also a source of bovine tubercle bacilli. Osteomyelitis was a significant cause of admissions, the numbers increasing even after the introduction of penicillin, perhaps, as one medical report suggested, because general practitioners realized early surgical care could prevent complications. Spastic paralysis, scoliosis, tumours, old bone and nerve injuries formed a significant remainder. Today, in complete contrast, tuberculosis, poliomyelitis, rickets and osteomyelitis produce very few admissions to orthopaedic units in Britain.
Miss Forrester-Brown's experience of congenital skeletal deformities was prodigious and in 1929 she published Diagnosis and Treatment of Deformities in Infancy and Early Childhood with a foreword by Sir Robert Jones (Figure 4).
22
This was aimed to assist early diagnosis by general practitioners and child welfare staff for, as she lamented, too many congenital defects were established and untreated before late referral, often when walking, being then considered by the family and practitioner ‘strong enough’ for treatment! She emphasized the importance of a thorough and careful examination with the patient naked except for a ‘fig-leaf’, illustrating her thesis with many clinical photographs, X-rays and apparatus. In the preface she recorded:
Title-page of Diagno sis and Treatment of Deformities
22
It would not be fitting to send forth this little book without a word of gratitude to the foundress of the ‘William Gibson Research Scholarship’ through whose generous benefaction the author was enabled to visit many of the famous orthopaedic centres on the Continent and in America, as well as noted ones in Britain; nor is it easy to express adequate appreciation of the kindness with which famous surgeons everywhere were willing to open their stores of wisdom and experience for the benefit of a colleague, however, junior.
In 1933 she co-authored Paralysis in Children with RG Gordon (1889–1950) MD DSc FRCP, Neurologist and Physician to the Orthopaedic Hospital. 23 The authors believed they had filled a gap in the literature by combining neurological and orthopaedic standpoints in order to obtain an accurate diagnosis and enhance surgical management. The first part is devoted to a detailed study of the physiology of movements, the second to descriptions of recognized neurological syndromes associated with paralysis and the third to treatment, including a final short section on surgery. It is well illustrated with diagrams, clinical photographs and equipment.
In 1935 she assessed 152 personal cases of congenital equinovarus (club-foot), 24 an experience accumulated over a mere 10 years that dwarfs that of today's surgeons, even many specializing in foot surgery. She emphasized the crucial importance of early and vigorous conservative care and the necessity to intervene surgically when progress was halted or relapsed; this included removal of hindfoot bone and rotational osteotomy of the tibia. Her paper listed additional appointments as Honorary Surgeon, Eastern Dispensary, Bath and Honorary Consulting Orthopaedic Surgeon, Swanage Red Cross Hospital and Walker-Dunbar Hospital, Bristol. In 1936 she published a short paper, ‘A clamp for stretching congenital club-feet’, 25 listing a further appointment as Consultant Surgeon to Wells and District Hospital.
In 1947 she lectured at the Royal College of Surgeons on ‘Operative procedures in poliomyelitis’, reported in their Annals of that year, 26 which discussed the possibilities and limitations of surgery, regretting that lack of time limited her lecture to a brief outline. It is evident her personal experience of poliomyelitis was formidable and her advice full of common sense. Recognition of this and of her many other contributions would have been appropriate by the award of an Honorary Fellowship of the College but the opportunity was overlooked.
Professional responsibilities, attainments and leisure pursuits
Maud Forrester-Brown was an assiduous supporter of professional associations and societies, in many of which she served as an officer. A member of the British Medical Association for over 50 years, she was honorary secretary of the Section of Orthopaedic Surgery at the Annual Meeting in 1931 and a member of the Association's Physical Education Committee formed in 1935 to report on the cultivation of physical development by the civil population.
2
In 1921 she was elected an active member of the British Orthopaedic Association, joining their Committee of Physical Education in 1936, becoming Honorary Secretary to the Association in 1937, an Executive Committee member in 1948–49 and an Emeritus Fellow in 1961. When the British Orthopaedic Association held their first visit abroad, in 1924 at Bologna, Miss Forrester-Brown was in the party (Figure 5). She was with the Association again in Italy in 1956 when meetings were held in Rome, Florence and Bologna (Figure 6) and at further meetings in France and Scandinavia.
27
In addition, she joined SICOT, the International Society for Orthopaedic and Trauma Surgery, later being elected an Emeritus Member, and also the Medical Women's International Association, attending their Ninth Congress in the Philippines in 1963 where she insisted on a personal bed-to-bed tour of patients in the National Orthopaedic Hospital.
2
From 1926 she was also a member of the Orthopaedic Section of the Royal Society of Medicine.
Maud Forrester-Brown, aged 39, visiting Bologna in 1924 with the British Orthopaedic Association, seated first on left; the other ladies are wives of delegates. Sir Robert Jones, seated in centre with a long white moustache; Vittorio Putti, cross-legged at the front in a white coat (reproduced courtesy of the British Orthopaedic Association) Maud Forrester-Brown, aged 70, visiting Pisa with Cyril Slack FRCS in 1956 (reproduced courtesy Cyril Slack)
As a result of her friendship with Vittorio Putti, the leading orthopaedic surgeon in Bologna, and her knowledge of Italian, she produced many English summaries for the journal Chirurgia degli Organi di Movimento and translated his book Historic Artificial Limbs in 1930 that described medieval iron prostheses in the Stibbert Museum, Florence, which Putti determined were designed for battle-field aristocrats on horseback;
28
fortuitously she was a very keen horse-woman. Stirling maintained she was fluent in five languages including Spanish, first studied in her sixties and added: She had a keen interest in all classical forms of drama, sculpture and painting; a wide knowledge of old masters, especially those of the Italian schools; a catholic knowledge of literature. Indeed her retentive memory and critical abilities made discussion of literature with her a formidable task.
2
During her later years in Edinburgh when she attended orthopaedic ward rounds and meetings, she must have become well known to Stirling who commented: Bodily fitness was not only a sermon to be preached to others; it was a goal to which she strove all her life – by ski-ing, skating, riding, golf and swimming. She took a vacation each February for winter sports, usually in Norway. Many associates must remember the twinkle in her eyes when she slipped away from a congress session with murmur: ‘I have an appointment with a horse’.
2
As already noted, she was said to visit country clinics on horseback and, according to Robert Robins, she often arrived similarly at the hospital where a large granite boulder outside the theatre and plaster-room building, known to the writer, was said to be her mounting block. Mary Franklin, treated by Miss Forrester-Brown for severe poliomyelitis and who subsequently worked in the operating theatre from 1937 to 1961, confirms her arrival on horseback 29 as does Sister Corp who commenced training as an orthopaedic nurse in 1942 and who also remembers her exclaiming, ‘Oh you “shilly” nurse’. 30 Stirling stated that three years before her death she was still riding once a week and swimming twice a week in the local baths. Her swimming skills were significant, according to a Bath press report in 1930 that recorded her fine display of diving at a Gala of the Beau Street Swimming Bath. This enthusiasm for physical exercise and postural regimes for her patients stimulated her donation of a Posture Cup for the girls of Bedford High School in 1934. 31 When aged six, Bob White recalls referral for poor posture followed by the agony of an exercise regime that his mother soon terminated after harsh words with Miss Forrester-Brown. 32 Despite much physical activity, she may have suffered from osteoporosis for she sustained at least four fractures after the age of 60. Robert Robins noted a fracture-dislocation of an ankle in 1947 for which she refused an anaesthetic, insisting on a skin tight plaster which she cut down to a below knee plaster the following day and resumed horse-riding, with an excellent result; 16 however, in November 1948 a local newspaper reported her fall from a horse caused a fractured collar bone. In 1960 she fractured the neck of a femur that was nailed successfully in Edinburgh, followed by a convalescent voyage to Cape Town on a ship with a gymnasium and mechanical horse offering suitable exercise for riders, avidly utilized by Miss Forrester-Brown. 2 On return she informed surgeons at the Bath and Wessex Orthopaedic Hospital, with great enthusiasm, how the mechanical horse had speeded her recovery and why she considered this a breakthrough in rehabilitating elderly ladies with hip fractures. She offered to buy such a machine for the hospital but was politely persuaded this would be inappropriate, even dangerous, for fragile patients who with few exceptions were unfamiliar with horse-riding. In 1962 she sustained a comminuted fracture of an elbow joint which was reduced and plastered briefly; she insisted on her own rehabilitation and within two months was swimming and driving her car. 2
Miss Forrester-Brown was a resident of Edinburgh after she retired from Bath and she died in the Edinburgh Royal Infirmary on 12 January 1970 after a cerebrovascular accident, aged 84 years. It is not yet known where she is buried.
Conclusion
Not only one of the pioneers of British orthopaedic surgery in the early 20th century, Maud Forrester-Brown was undoubtedly the first female orthopaedic surgeon in the UK and probably worldwide. Shortly after she became a member of the British Orthopaedic Association in 1921, Florence Barrie Lambert CBE MB DPH was also elected, perhaps for her late service as an Inspector of Military Massage, for she was not a surgeon; the second female surgeon elected was Vera Veitch MB in 1929. 27 In 1983 the Ruth Jackson Orthopaedic Society was formed for women orthopaedic surgeons of North America – Ruth Jackson being the first to practise in the USA in 1932, achieving membership of the American Academy of Orthopaedic Surgeons in 1937.33 Possibly earlier female surgeons in Continental Europe remain undiscovered by the writer?
As is evident, Miss Forrester-Brown dedicated her life to an emerging specialty, making significant contributions to its science and literature, and sparing no effort to keep in touch with developments at home and abroad. Indeed her international connections were extraordinary, even before the development of air transport. Everyone who remembers her, including the writer when she was aged 78, recalls a formidable personality with firm opinions based on the prodigious experience yet also a compassionate lady with a clear enquiring mind.
It was principally due to her knowledge, energy and dedication that a vast network of clinics were established throughout three counties for the treatment of neglected crippled children. Thus was forged a favourable reputation for the Bath and Wessex Orthopaedic Hospital in treating surgical tuberculosis, congenital deformities, poliomyelitis, rickets, scoliosis and osteomyelitis at a time when most preventive and therapeutic remedies had yet to materialize. She was a devoted practitioner and exceptional woman who, sadly, never figured in an Honours List, nor yet in the Dictionary of National Biography.
Footnotes
Acknowledgement
I wish to thank Robert Robins, former Consultant Orthopaedic Surgeon, Truro, Cornwall and house-surgeon to Miss Forrester-Brown, 1947–48, for his special help and advice.
Addendum
Since completing this communication, the Oxford Dictionary of National Biography was approached to consider Miss Forrester-Brown's exceptional history as meriting an entry in a future volume and they have agreed. The author has been asked to formulate this in 800 words.