
Abstract
Edgar Pask worked before, during and after World War II with the anaesthetist Robert Macintosh. Both were ranking officers and engaged in work with the Royal Air Force Physiological Laboratories at Farnborough, then in the charge of Dr Bryan Matthews. Pask submitted as a Doctorate Thesis a compilation of much of the experimental work in which he was the main subject, most of the data being acquired while he was unconscious. Experiments in which the Farnborough Team were engaged form a central core to the Thesis and relate to the development of life jackets. The information is well known and has been widely publicized, along with most of the biography of Pask. However, some extreme physiological experiments, again with Pask as the test subject and which probably were not conducted at Farnborough, are less well known but in their own way even more extraordinary. The theme in common is Pask's ideas to use the anaesthetized state and the properties of anaesthetic agents as surrogates to the extreme situations Royal Air Force pilots were subject to in modern warfare. There is no purpose to detract from Pask's ideas and selfless heroism by digressions into parallel processes conducted by the opposing Oberkommando der Luftwaffe (OKL) research establishments, but it is evident these were known and had shocked the Farnborough Team (including Pask) before revelation at the Nuremberg War Crimes Trials.
… you cannot be a good human physiologist unless you regard your own body, and that of your colleagues, with the same sort of respect with which you regard the starry sky, and as yet as something to be used and, if need be, used up.
1
J Burdon S Haldane (1892–1964)
Dr Edgar (‘Gar’) Alexander Pask trained at Downing College, Cambridge and the London Hospital, qualifying in 1937. He joined Professor Robert R Macintosh (1897–1989) in 1939. 2 ‘Mac’, as he was universally known, had a formidable reputation. Service in the Royal Flying Corps in World War I and experience as a troublesome German prisoner of war seem enough even without his reputation in practical and war anaesthesia and his nurturing of a fledgling discipline of academic anaesthesia as a Nuffield Professor in the University of Oxford. 3–5 He was promoted quickly to the rank of Group Captain in the Royal Air Force (RAF) as Britain entered World War II.
Pask, Macintosh's First Assistant, would also have been influenced greatly by the life, teachings and example of John Scott Haldane (1860–1936). Pask seems to have been keen to emulate the exploits of such greats, no doubt despite knowing the hazards such a course into experimental physiology might take. 6,7 The work as a clinical anaesthetist at the outbreak of war and joining the RAF were to prove opportune to put some of his ideas to use. In essence, these were to exploit the anaesthetized state and explore the endurance physiology of man at the extremes of the aerial wartime environment. In due course he defined these problems in order to submit his thesis for the degree of Doctor of Medicine 8 (Figure 1).

Professor Edgar Alexander ‘Gar’ Pask OBE MB BCh MD DA FFARCS. The copyright is untraced: the source is the Dr Brian Welsh Anaesthesia Archive, Royal Victoria Infirmary, Newcastle upon Tyne (1998)
Parachute descent from aircraft flying at high altitude (the first problem)
An early proposal was to simulate conditions in which disabled pilots would have difficulty to deploy a parachute. The protocol assumed they would be unconscious or rendered so immediately on bailing out since they would be separated from static oxygen supplies.
The RAF Physiological Laboratories at Farnborough, then under the direction of the civilian physiologist Dr Bryan Matthews (1906–86), had decompression chambers that provided the usual setting for high altitude (20,000–30,000 ft) simulations for aircrew and researchers. 9 Flight Lieutenant Pask's idea of using a decompression pressure chamber while being suspended in a parachute harness and going beyond the usual limits were considered too dangerous and so the Nuffield Department of Anaesthesia in Oxford became the site for the ‘top secret activity’ experiments that were conducted at atmospheric pressure. 10–12
It was already known that the altitude limit for bailing out without oxygen or losing consciousness was in the region of 20,000 ft. 13 The starting point for the experiment was set to simulate 30,000 ft. Test subjects breathed a changing concentration of nitrogen or nitrous oxide. Oxygen was gradually introduced into the breathing circuit, 4% oxygen at sea level being equivalent to 35,000 ft, and increased with a theoretical descent rate assumed to be 2000 ft a minute. 14 A stenographer recorded Macintosh's observations on what was to become typical of 16 experiments recorded in the Thesis on five subjects, but the bulk, eight in number, were on Pask himself. Three experiments (one each on three subjects, of which Pask was one) were conducted with the test individual suspended in a parachute harness. In the fourth descent the experimental ceiling was raised to the equivalent of 40,000 ft while supine and breathing 2% oxygen at sea level. 15
Descent number 4 gives details of Pask, lying and breathing either nitrogen and oxygen or nitrous oxide and oxygen at a simulated altitude of 40,000 ft:
Minutes:
Subject already unconscious Respiration irregular and jerky Pupils 2/3ds dilated, eyes pulled to the right and downwards. Forced, prolonged, irregular respirations Forced expirations. Gasping inspirations Marked jactitations Expirations less forceful rhythm becoming regular Jactitations have ceased: eyeballs still displaced: pupils 2/3rd dilated Causing no anxiety Very brief irregularity of pulse noticed Still not answering questions Speaking and asking questions
On completion of the series, it was concluded that for the majority of subjects (on the basis of supine tests and their tolerance of altitude) a 40,000 ft descent was ‘on the borderline of safety’; however, in those suspended in a parachute the risks were significantly higher and therefore deemed ‘unsafe’. The final recommendations were that parachute opening should be delayed until below 30,000 ft and that all aircrew flying above 30,000 ft ‘should be provided with emergency portable oxygen equipment for use during descent’. 16
The efficiency of methods of artificial respiration (the second problem)
To test the different methods of resuscitation, the research protocol for the Pask idea took into consideration that the drowned or near-drowned pilot would have to be resuscitated by personnel undergoing a rough passage in the cramped conditions of an Air/Sea Rescue Launch. It is not hard to see that his supervisors would probably have had to tone down such an idea, given Pask's subsequent record and actions where he quite happily undertook projects for real at sea. Instead, in 1943 he was the subject of at least one experiment in which he was fully anaesthetized with ether and this agent, in the jargon, ‘pushed him’ to the deep Guedel stages of anaesthesia to cause respiratory muscle paralysis. Then several of the more promising possible methods of artificial respiration were tested and examined in succession. This set of experiments was set aside although the idea seems not to have gone away. It was revisited in 1946 by which time the anaesthetic technique and lessons learnt were the template applied to render unconscious an individual (Pask) on which to test survival equipment for exposure and immersion protection. 17
The testing of life jackets (the third problem)
These sections of Pask's research and Thesis are very well documented: parts were even filmed contemporaneously and in re-enactment for a feature film. 18–20 Most famous are the experiments in which Pask was anaesthetized by Macintosh for many hours, intubated with a non-cuffed tracheal tube and kept asleep by means of ether through a long anaesthetic pathway that was in most elements a prototype of what was later to be called the Bain system. 21–24 In typical and underwhelming manner, the full scientific description of these endeavours did not appear until 1957, published with Macintosh as the lead and under the rather modest title of The Testing of Life Jackets. 25
There was more work in the lab and in the field on flying clothing and immersion testing carried out in this period of Pask's war: and even some amusing project's like the designing of an oxygen mask so that the wartime Prime Minister, Winston Churchill (1874–1965), could smoke his cigars when being flown above 10,000 ft! 26, 27
Problem 2 revisited
The finale to Pask's big ideas was to be the combination of all his subjective experience and more. The experiment was undertaken in March 1946. 28 The research proposal was to repeat the experiments on artificial respiration in the light of some new physiological ideas into standardizing ways of comparing techniques and of removing the experimental confounder of respiratory muscle movement that had been regarded as being a drawback to earlier work. In his Thesis, Pask refers to the suggestion ‘tests should be made on curarised large monkeys’. Pask's thoughts clearly had gone beyond even such a radical concept. The advent of clinical preparations made Pask think that Man would be an appropriate subject and the reports of ‘reversible complete paralysis of all respiratory muscles with it [curare]’ meant that he was certain to be tempted to be the first.
Air Commodore Macintosh administered ether to Squadron Leader Pask through an endotracheal tube. But on this test, instead of ‘pushing’ the general anaesthetic to the point of respiratory arrest, a different mechanism was used. Pask's Thesis record is eloquent beyond further description. 29
Subject EAP. Age 34. Wt 10 stone
The subject had already been anaesthetised for 1 hour 58 minutes, with diethyl-ether and air for an experiment on the basic floatation position of certain life jackets to be described in the last section of this thesis. Anaesthesia had been uneventful except for some tremor during immersion.
Timetable
Time
Administration of ether ceased and no further ether was administered. Respiration vigorous – both diaphragmatic and intercostal 20 mgs Tubo-curarine chloride administered intravenously 10 mgs Tubo-curarine chloride intravenously. Spontaneous respiration ceased. No evidence of any diaphragmatic or intercostal action. Artificial respiration by Silvester's method commenced Measurement of ventilation and oxygen consumption under Silvester's method Change made to Schafer's method Measurement of ventilation and oxygen consumption under Schafer's method Change made to Eve's method Some evidence of diaphragmatic activity 10 mgs Tubo-curarine chloride intravenously. Diaphragmatic activity ceased Measurement of ventilation and oxygen consumption under Eve's Rocking method (45 deg-0–45 deg) made About 17.35 spontaneous respiration became adequate again
Pask's earlier conclusion to Problem 2 was that the Eve's method was the most suited to the needs of the service – to be practical at sea under operational conditions. This last experiment confirmed that view, scientifically. Using the same tidal volume mark as standard, Eve's method was the better in terms of oxygen consumption implying a greater effect on blood circulation brought about by the rocking motion integral to the technique.
By the time Pask wrote up his Thesis, reports of the clinical use of curare, since classic in the development of muscle relaxant use in modern anaesthetic practice, were available for referencing. He and Macintosh had been aware of ether potentiation of the actions of muscle relaxant drugs when used in what at that time were uncontrolled clinical experiments with various curare-based concoctions in the USA, Canada and the UK. 30,31 Nevertheless, acquisition of any paralysing drug was difficult and its use controversial, experimental and already known to be very dangerous. The reversibility of muscle paralysis was still uncertain, the mechanisms theoretical and barely understood, and the antidotes unknown and untested. Military associations may have been crucial. Macintosh is recorded as having acquired some ‘Intocostrin’, the most pure curare extract at the time, from the ER Squibb Company through the good offices of Harold Griffith (1894–1985), then Wing Commander and Consultant to the Royal Canadian Air Force. 32 Dr John Halton (1903–68), also attached to the RAF and closeby on Merseyside, was another anaesthetist interested in the potential of curare in anaesthesia. 33,34
Now, in the 21st century it is difficult to see how any scientific equilibrium on which to base a comparison of techniques was going to be achieved with the then methodology. By the end of two hours of deep ether anaesthesia and the additional effect of total respiratory muscle paralysis, Pask's body temperature, carbon dioxide levels and acid base status would have rendered him perilously close to cardiac arrest: he would have been in the physiological equivalent of the mountaineers ‘death’ zone and a lot closer to the reality of a near-drowned pilot than would have been intended or recognized. Was it necessary? The War was over!
The use of curare by the Oxford Group is not mentioned in a 1945 publication, but in his obituary of Pask Macintosh states that ‘Later in the War’ Pask ‘asked’ to repeat the earlier work on artificial respiration using the newly introduced curare. 35,36 This phrasing, though possibly strictly true in relation to the idea, is, like several things in the Pask saga, at variance with the Doctorate Thesis record and just a part of why ‘he remains something of an enigma’. 27,37 The experiment does, however, give a structured completeness to the production of a Thesis, to be entitled the ‘Applications of Anaesthetic Techniques in Physiological Research’ and that was to be compiled out of scientifically disparate and extraordinarily hazardous experiments, but no longer justified for the war effort. Ironically, this experiment was probably out of the control of Bryan, later Professor Sir Bryan, Matthews FRS (1906–86) who was to become Professor of Physiology at Cambridge where, on 27 November 1946, the Thesis was submitted.
The influence of the OKL
Writing in the context of the rejection of plans to use a decompression chamber to simulate parachute descent from altitude, Pask states:
There is reason to believe, however, that in later years German investigators used this method and carried out a number of fatal experiments upon ‘condemned experimental persons
38
(Figures 2 and 3). A test subject is seen in a swimming pool or tank of water with two or more attendants. Professor Robert Macintosh, Nuffield Professor of Anaesthesia, is the bald-headed man. Pask is anaesthetized and in the water (reproduced from a copy of IAM Report No. 614
19
) This scene appears almost the same as that in Figure 2. However, Professor Holzlöhner, Professor of Physiology at Kiel, is the observer to the left of Rascher and he committed suicide before the Nuremberg Trials. Sigmund Rascher was executed by the Nazis in 1945. A condemned concentration camp inmate is in the water and not anaesthetized (copyright and acknowledgement is the Dachau Memorial, see www.archiv@kz-gedenkstaette-dachau.de [2006])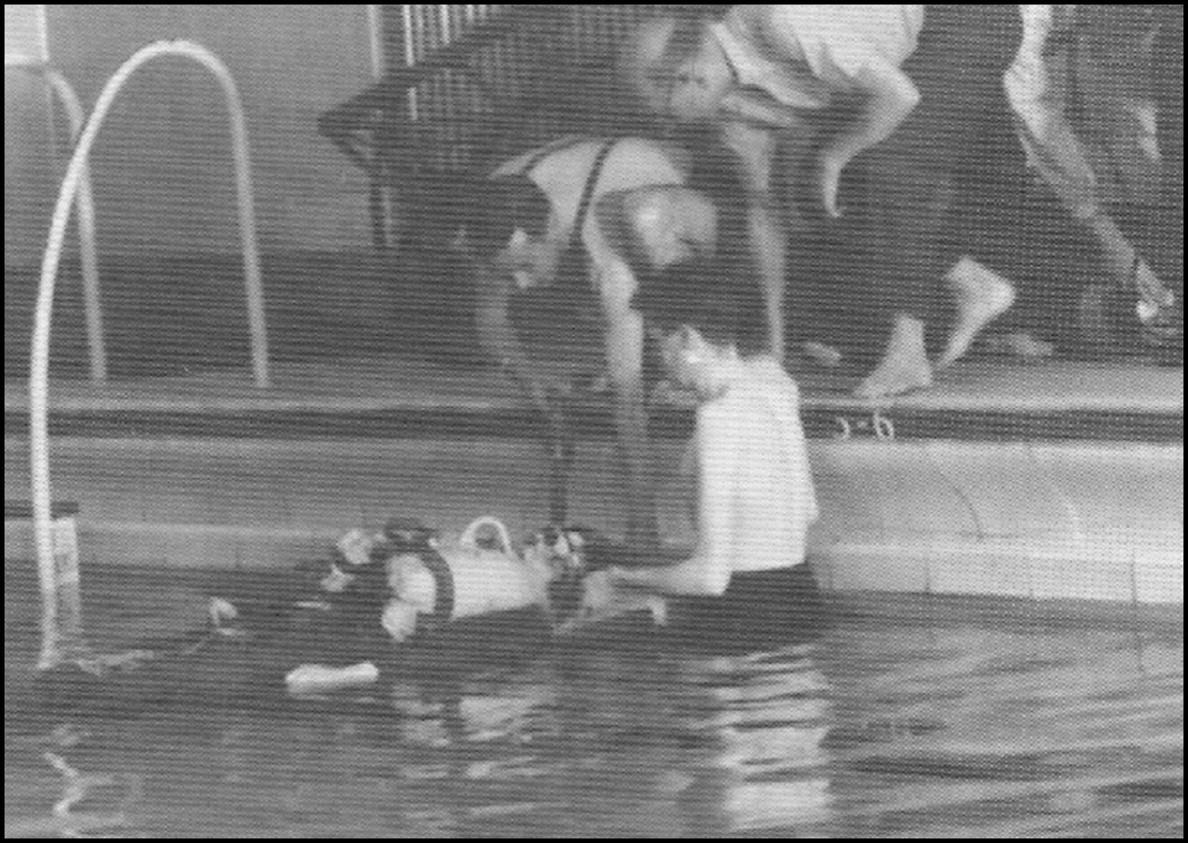

Pask had first-hand evidence, having been sent to Hamburg at the cessation of hostilities to salvage anything that could be of use in Farnborough. 39 The order came from Roland H Winfield (1910–70) who, charged with debriefing captured scientists, had begun to find that the OKL, faced with the identical challenging scenarios as the RAF, had gone beyond what was regarded as inconceivable in order to obtain answers. Though the OKL methods, means and, in particular, the activities of Sigmund Rascher will haunt aviation medical science, Winfield and Pask probably stumbled on others that did not get exposed or aired at the Nuremberg Trials. The anger Pask and his companion felt at what they found resulted, almost punitively, in enough salvage or ‘requisitioning’ for four Lancaster bomber flights and left senior officers with the dilemma of what to do with two serving military officers who had so wilfully committed an act of looting. 40 Reprimands were delivered for form's sake and carried little conviction, given the horror and revulsion clearly being felt at the revelations later to be euphemistically described as ‘one of the darkest chapters in the history of high-altitude physiology and medicine’. 41 The ‘loot’ was being used many years later in Farnborough and some possibly for Pask's research. 42 A camera nicknamed ‘the Robot’ and with clockwork drive is a possible candidate for souvenir from a Hamburg visit. 43
After Oxford
As the super-powers moved quickly into the jet, stratosphere and space ages, technological advances supplanted the Pask concept of anaesthetically induced unconsciousness at sea level atmospheric conditions as a surrogate for extreme physiology and a model or tool for aviation research on volunteer human subjects. That the concepts and model were only of value and relevance during the short period of World War II and resulted in significant savings in the lives of those in the sea would go some way to explain why the other experiments in the Oxford/Farnborough work have not been seen as landmarks in aviation and high altitude physiology. 9 It would also go some way to explain why Pask, in Macintosh's opinion and with a record that would have secured a prestigious chair of physiology anywhere in the world, and now so thoroughly moulded to the ways of the Haldanes (father and son), chose to move to the North East of England, a place as it turned out much more suited to his developing post war and more fruitful research interests.
Pask earned an OBE for his war work. Macintosh ensured any weaknesses as a clinical anaesthetic practitioner were dealt with by sending Pask to the USA. He returned to anaesthesia. Though he was never to be a match practitioner for Dr MH Armstrong Davison (1911–70), a polymath with a significant war record and something of an academic competitor, the indefatigable Pask quickly established an academic department as Reader in Anaesthetics at Durham University. 27,44 His role model would seem to have shifted from Haldane to Macintosh and his department generated a succession of practical and simple devices ranging from monitoring methods to a series of ventilators. In 1949 he was awarded a personal chair, becoming the second Professor of Anaesthesia in the UK. As such, he formed one of the most successful post war schools for academic anaesthesia. 27 Fifty years later, the University of Newcastle upon Tyne abolished the post of Chair of Anaesthesia, of which he had been the founder holder.
Professor Pask continued to be driven, despite his proneness to seasickness, to saving life at sea. 45 The immersions in all weathers continued, this time off the coast of Northumberland and in colliery swimming pools to add to those in Shetland, Iceland and other hostile seas. Some of the burden was shared with Seaworthy ‘Sierra Sam’ – a life-sized, weighted and articulated dummy with some electronics that was to become his sea-going alter ego. 46,47
Pask was seen as never quite the same after the experiments on resuscitation, the last certainly taken too far and overinflating his lungs to the point of permanent damage. 48 His cigarette smoking addiction did not help and he died of a myocardial infarct in 1966 at the age of 53.
The Doctorate Thesis is remarkable and extraordinary not just because the bulk is based on data acquired while he was rendered unconscious, with gruelling and experimental anaesthetic techniques requiring endotracheal intubation over many hours, but as testament to his unique courage: courage that was to earn the label ‘the bravest man in the RAF who never flew an aircraft’. There is little doubt that Edgar Alexander Pask was ‘used up’ as stated in the IAM Report No. 614 and, borrowing the famous JBS Haldane quote, this was by his colleagues administering arrow poison extract and other potentially fatal agents and techniques. 49,50
Footnotes
Acknowledgements
I am grateful to Mr Norman Burn, a holder of the Association of Anaesthetists of Great Britain and Ireland Pask Certificate of Honour, for the conversations and information about working with Professor Pask after World War II and for a copy of IAM Report No. 614. 19