
Abstract
Sir Geoffrey Marshall was a remarkable, hard-working man who helped in the development of anaesthesia and respiratory medicine. Both were in someway helped by his military experiences in World War I, first when working on an ambulance barge and then in the Casualty Clearing Stations researching the increasing problem of surgical shock. Among a multitude of high-ranking medical posts he also acted as Physician to King George VI and Sir Winston Churchill when they developed respiratory conditions.
Early life
Geoffrey Marshall (Figure 1) 1 was born on 23 April 1887, the son of Henry Marshall from Bognor in Sussex. 2 His early education was at St Paul's School before enrolling for medicine at Guy's Hospital whence he graduated MBBS in 1911. After qualifying he worked as a general practitioner and then in the Physiology Department at Guy's Hospital in and then London.

Sir Geoffrey Marshall (1887–1982) (reproduced courtesy of Thomas KB. The Development of Anaesthetic Apparatus. London: Blackwell, 1980:143, with the kind permission of the Association of Anaesthetists of Great Britain and Ireland)
World War I
On an ambulance barge
At the outbreak of the war, Marshall left his physiology post to work with the Royal Army Medical Corps (RAMC). His first post was in charge of a 20-bed ambulance barge that had been fitted up as a mobile evacuation hospital
3
and was staffed with two nurses. Due to the muddy waters often being used for bathing by the troops, he gained a lot of experience in reviving the apparently drowned.
3
Away from the water he recalled that his work would include attending barns. On one occasion he was asked:
Look here, Doc, do you mind mending these chaps? We can't report them because they weren't supposed to be fighting but there was a lot of noise the other night and we knew there was a battle on and we thought we ought to join in. It's very awkward having some wounded because we can't possibly let them go through the ordinary channels or we shall get dismissed.
3
This was enjoyable work for Marshall who remembered fondly that ‘one became a very popular character. They would say “come for a drink anytime the barge fetches up”’. 3
Research on shock and the development of an anaesthesia machine
However, it was mainly in the specialty of anaesthesia that Marshall's work in World War I was to become better known. World War I has been credited with helping develop anaesthesia through the actual need and creation of a specialist anaesthetist at the casualty clearing stations (CCSs) as well as the monitoring of the depth of anaesthesia and disseminating how to do this.
4
Before the war, comparative work had not been undertaken on the effects of different anaesthetic agents on the severely injured.
4
Previous studies had focused upon morbidity and mortality rates but not in distinct groups. The outbreak of war created subgroups of patients that could reliably be compared, the most important comparison of which was to be in the different severities of shock.
4
This had been the subject of debate in the Crimean War but never quantified sufficiently.
5
Consequently, Marshall's ideal barge posting ended in 1915 when:
A dreadful old man, who was the senior consultant, Sir Anthony Bowlby (1855–1929), drove up to my barge one day – lovely day – and said, ‘Marshall, we are having an awful lot of deaths in the forward hospitals from shock, and you did a lot of work on the physiology of anaesthesia before the war so I want you to come along and see if you can do anything about these chaps.
6
The result was a transfer to CCS number 17 and the start of multiple observations and reports aimed to accomplish Bowlby's brief. This involved measuring the blood pressure, pulse and haemoglobin concentration in patients arriving at CCSs in different degrees of shock. The averages of these measurements were calculated at intervals before, during and after operations with different anaesthetics and then compared. 7
Marshall presented his findings on 2 February 1917 at a meeting of the Section of Anaesthesia of the Royal Society of Medicine. 7,8 This was a landmark for anaesthesia. The main subject of his attention was spinal anaesthesia which he revealed could cause extreme hypotension up to 40 hours after the anaesthetic, a time that would have been further extended but for replenishment of intravascular volume with fluids. 7 Similar dangers were witnessed with the intravenous administration of alcohol and 6% ether, as well as the inhalation of chloroform and ether. 1 However, ether was seen to protect the patient during the operation, currently thought to be due to the sympathometic effect of ether on cardiac output. Therefore, after a chance meeting with the American anaesthetist James Gwathmey (1863–1944) who in 1912 had introduced a nitrous oxide and oxygen machine, Marshall focused his energies on the combined nitrous oxide, oxygen and ether technique. This he administered with an improvised machine that he commissioned from a tinsmith in France. 1 With this, he found that shocked patients survived better than with any other agent or combination of agents and, when reminiscing on the experiment, he believed ‘We cut down the mortality from about ninety percent [in thigh amputations] to something like twenty-five percent’. 9 Furthermore, he observed that these patients made quicker recoveries probably due to lighter anaesthesia and quicker return of consciousness.
The increasing use of the nitrous oxide, oxygen and ether sequence was to stimulate elaboration of the anaesthetic machine. As has been described already, Marshall had designed a machine for his own use. However, when he returned to London to present his paper, he took his design to Coxeters, the instrument manufacturers. They approved of the blueprint and agreed to manufacture the machine. This machine became the standard RAMC machine in the latter parts of the war (Figure 2). 1 Consequently Coxeters warned him: ‘For goodness sake, publish this because some chap has borrowed our blocks’. 6 The advice was not taken since Marshall was needed back at the Western Front. This allowed the gentleman in question, Captain Henry Boyle (1875–1941) who had attended Marshall's aforementioned presentation, 8 to attach his name to a slightly altered version of Marshall's machine. 10 For Boyle this success led to a career in anaesthesia and the development by 1933 eventually of eight anaesthesia machines. 4 Boyle's name, largely due to Marshall, is still associated by some with the vastly different apparatus of today. 4
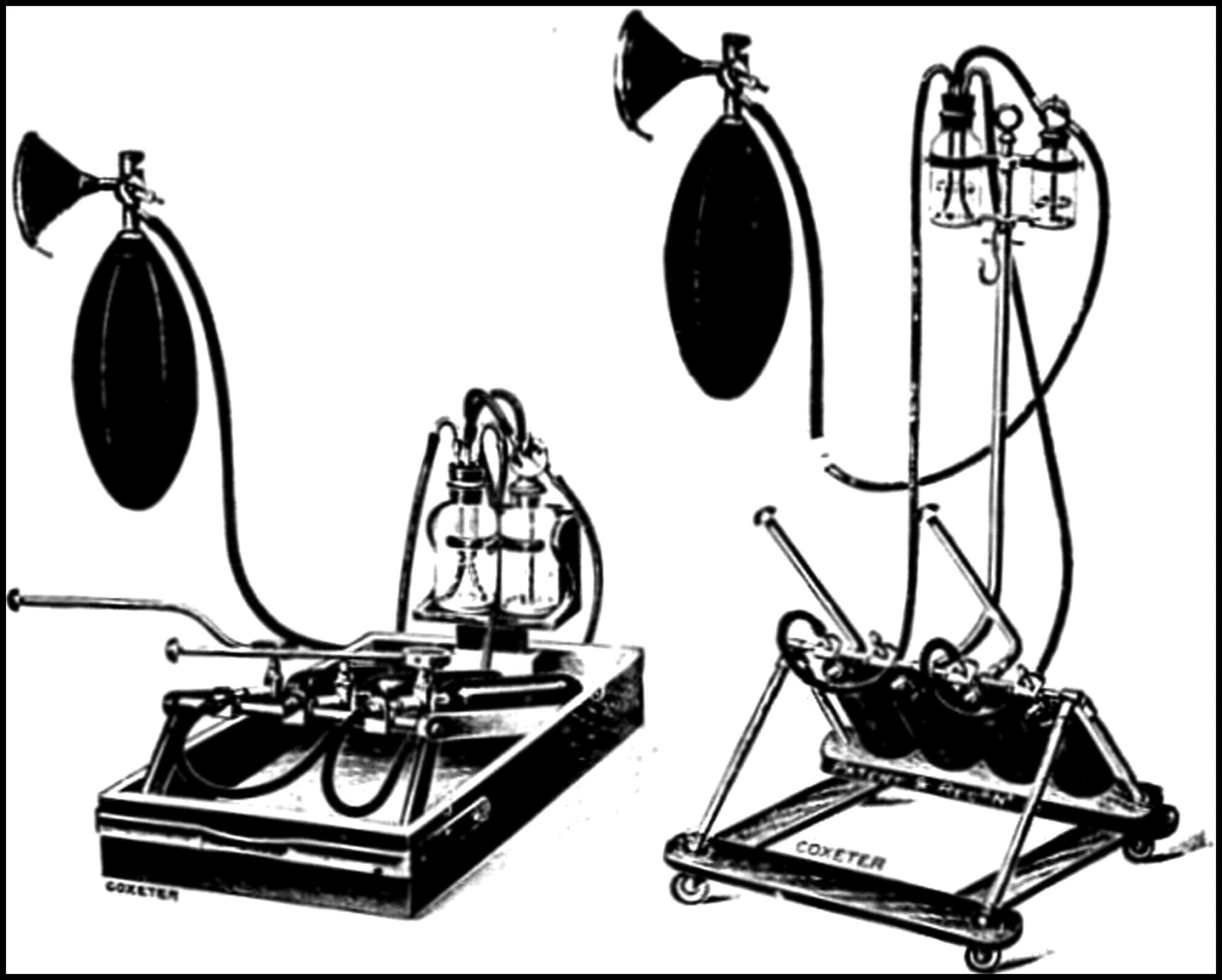
Marshall apparatus in complete form (reproduced courtesy of Thomas KB. The Development of Anaesthetic Apparatus. London: Blackwell, 1980:145, with the kind permission of the Association of Anaesthetists of Great Britain and Ireland)
Resuscitation techniques and the extension of the role of the anaesthetist
As well as improving knowledge of the role of anaesthesia in shock, World War I aided the strategies for its general prevention and treatment. One of these included the improvement in the infusion of fluid as part of the resuscitation procedure. Again, a lot of credit for this must be given to Marshall for it was he who noticed in autopsies that the giving of three pints of fluid subcutaneously to shocked patients was useless as the fluid remained in the axillary folds. 7 Accordingly, the custom of giving fluids intravenously received momentum during the war and by the end of the war intravenous infusion had become an integral part of medical management at all the evacuation stations. Consequently Marshall is seen as one of the catalysts of anaesthesia development before the 1920s. 4
Gas casualties
Marshall was mentioned twice in despatches during World War I and was awarded the OBE in 1917 for his work on treating poison gas victims. In 1916 he was working at a Clearing Station near Poperinghe in the Ypres Salient when chlorine gas was used for the first time in warfare. Marshall was known to have worked in physiology and so he was asked for a solution when hundreds of men appeared in a winding trail each with his hand on the fore-runners' shoulder. Under Marshall's direction they were laid out in rows on the ground and then:
like an irrigation system, we had tubes running between the files of men, their heads towards the main tubes, head to head in two lines. We had any number of glass connections and finer tubing and we stuffed a fine tube up the nose of every man and kept the oxygen running with cylinders every so many feet apart so as to keep up a good pressure.
9
The oxygen worked but ‘their eyelids were terribly swollen, but if you pulled them apart men could see, and so I sent other men up and down the lines shouting out to them that they had not been blinded’. 9 This psychological boost was said to have been nearly as valuable to the men as the oxygen. 9
Immediately after World War I
The Armistice in 1918 occurred during Marshall's honeymoon with his first wife Belle Philip (d. 1974) whom he had met when she worked as a theatre sister behind the battle lines in France. 9,11 His next six months were spent at Tourcoing in France, close to the Belgian border where ‘a lot of our chaps were coming out of prison camps in Germany and finding their way back through our lines. They were emaciated and badly clad, and trampling through the snow, and of course the flu bowled them over … an awful lot of them died’. 3 Marshall tried managing these patients in beds out in the snow and found that his 60% recovery rates compared favourably with the 20% recovery rates of others. 3
Becoming a Consultant Respiratory Physician
After demobilisation with the rank of Major he did not become an anaesthetist as he wanted to go into medicine. After a short period working in the Physiology Department at Guy's with Professor Marcus Pembrey (1868–1934) he proceeded to his MD with a Gold Medal in 1920 and took the MRCP. Later Marshall recalled that he was ‘quite rightly’ 9 beaten to the appointment of Physician to Guy's Hospital by John Ryle (1899–1950, later to become the first British Professor of Social Medicine). This situation caused Hector Cameron (1878–1958, later to become the first paediatrician at Guy's) to give up his position on the consultant staff as he thought a further position would not come Marshall's way.
However, a position as Physician at Guy's did become available and Marshall was appointed in 1920. He moved into chest medicine ‘because I was good in the job of managing the tuberculosis department. There were a lot of awfully nice fellows doing chests then’. 3 He cited an example of such generosity when ‘some swarthy man came into my out patients … and said “You don't know me at all. My name's Chandler, and I've got a parallel job with this at Bart's, I've been doing it for six months – you haven't been doing it for six weeks. So I've learned something about it and I'm going to work as your clinical assistant”’. 3 He was soon to be given the job of founding the combined Chest and Tuberculosis Department and later he developed his own pneumothorax apparatus. In 1928 he was appointed FRCP and in 1934 Consulting Physician to King Edward VII Sanatorium at Midhurst and the Brompton Hospital for Diseases of the Chest. 12
World War II and Sir Winston Churchill (1874–1965)
Unfortunately for Marshall and his wife, personal tragedy befell them early in the war when their only son, George Philip, died on Christmas Day 1941 from wound diphtheria while on active service in the Rifle Brigade in Africa. Marshall never let this loss affect his work. Consequently, due to his experiences with poison gases in World War I he continued as adviser in defence against chemical warfare for the southern region in England. He sat on numerous War Office committees in London and at Porton Down. In 1943 he was called to the scene in Chichester when an accidental poison gas explosion occurred at a demonstration. The timing of this was not ideal for Marshall as it meant he was called away by the War Office on arriving at his Silver Wedding Anniversary Dinner hosted by friends when, rather unusually while rationing was at its height, the dinner was to be a roast goose and all the trimmings. 9
At the same time he was Physician in Charge at the Brompton Hospital and would sleep either at the hospital or in the cellar in his garden at Hampstead during the air raids. 11 In 1944 Marshall was working in outpatients when Lord Moran called him to 10 Downing Street to see Mr Churchill who was chesty and feverish. Geoffrey diagnosed pneumonia and informed the Prime Minister: ‘You will have to relinquish the conduct of affairs for a fortnight’. 13 Churchill is said to have replied: ‘How dare you! The war is at a critical stage’. 13 Marshall's well-known communication skills succeeded when he asserted: ‘but you know what we call this illness? We call it old man's friend because you fade away so gradually that you arrive in the next world before you know you've left this one!’ 13 to which Churchill answered: ‘Am I as ill as that? Very well, then I'll do as you say’. 13 Churchill was as good as his word and he got better on his much beloved ‘M & B’, known correctly as the sulphonamide antibiotic sulphadiazine, as well as the novel Moll Flanders that Marshall gave to distract him, the story of a female schemer. 13
Streptomycin and the first randomized control trial
Following the immense success and publicity of penicillin, a lot of research for potential antibiotics was undertaken using other fungi. 14 In 1943 streptomycin was isolated and this proved very effective against tubercle bacilli, first in the test tube and then in tuberculosis in guinea pigs. 14 However, the drug was very expensive and consequently, in July 1946, the Ministry of Supply asked the Medical Research Council (MRC) to organize clinical trials to test the small volume of streptomycin supply. 15 It was to Marshall, through his overall burgeoning reputation and specific work at the Brompton Hospital, that the MRC turned.
The streptomycin MRC trial ran from 1946 to 1948. 14–17 Marshall chaired a hastily arranged conference of clinicians in November 1946. This 15-strong group included Austin (later Sir Austin) Bradford Hill (1897–1991), Professor of Medical Statistics at the London School of Hygiene and Tropical Medicine. Several years earlier Bradford Hill had set out the principles of clinical trial design and the requirement of allocation and randomization 16 but had been worried that doctors would be unwilling to relinquish the doctrine of anecdotal evidence. 14 Despite this, the trial group decided to focus on pulmonary tuberculosis and to use untreated controls. The decision as to whether a patient received streptomycin or a control was decided by using Bradford Hill's process of randomization. 16,17 Patients were blinded to the treatment they received as were the clinicians assessing the results using monthly chest radiographs, and direct smear and culture of sputum.
Published in 1948, 17 the trial was extremely useful. With regard to streptomycin, it showed that it did have clinical benefit in treating pulmonary tuberculosis. In addition it also revealed the problem of resistance that had not yet been seen with penicillin, as well as the side-effects of streptomycin. However, it is widely accepted to have been the first randomized curative trial. This heralded the general conversion of scientists to randomization and so the subsequent trials and eventual evidence and developments have all been possible following this. Dr (later Sir) John Crofton (1912–2009), who was the Streptomycin Registrar for the trial at the Brompton Hospital, reported that some of the success of the trial was due to the reassurance given to clinicians entering their patients to the trials with regard to any ethical dilemma. 14 The reassurance was credited to two factors – first, there being no effective alternate treatment and second, the prestige of Marshall as the Chairman of the Oversight Committee. 14
King George VI (1895–1952) and the KCVO
In 1951 Marshall was to have further heavy responsibility in looking after King George VI when Clement Price Thomas (later Sir Clement [1893–1973] operated on him for bronchial carcinoma. While staying in Buckingham Palace to supervise the King's recovery after the operation performed by Price Thomas, Marshall was Knighted by the King. One of Marshall's treasured possessions was a letter from the King, written in his own hand, expressing his gratitude for all that he had done for him. 11
Further medical work
Marshall undertook a range of medical duties throughout his life. This included being a Medical Referee to the Civil Service Commission, for which in 1951 he was appointed CBE, and Consulting Physician to the Ministry of Pensions. He took a leading role in forming the Association for the Study of Diseases of the Chest (later the Thoracic Society), becoming its President. This role he also undertook for the Section of Diseases of the Chest at the Annual Meeting of the British Medical Association in 1956, the Section of Medicine of the Royal Society of Medicine 1941–2 18 and later of the Society itself (1958–60) who elected him an Honorary Fellow in 1962. In 1955 he delivered the Tudor Edwards Lecture at the Royal College of Surgeons. In the Royal College of Physicians he served as Examiner, Councillor and Harveian Orator, and was recipient of the Weber Parkes Prize in 1960 for his example over many years in the clinical care of his patients. He wrote many papers in his specialty and was the author of Diseases of the Respiratory Tract in Conybeare's Textbook of Medicine and Editor of Diseases of the Chest (1952). In addition he served as Sub Dean of the Medical School at Guy's.
Marshall's own respiratory health
When he was 74 years old, Marshall developed a cough and went to have a chest radiograph that proved unremarkable. He insisted he had a hissing suction with every inspiration and must be broncoscoped but nothing was found. 9 He then persuaded his friend and colleague Clement Price Thomas to explore his chest with the words: ‘Take anything out you don't like the look of’. 9 As a result his left lower lobe was removed in March 1964. He said afterwards that he had never felt better. This confidence in chest surgeons had been seen throughout his career at a time when physicians were reported to be mistrustful, indeed resentful, of chest surgeons. 13
Away from medicine
He enjoyed many aspects of life outside of medicine. He loved the ballet and watching sport. In earlier days he watched cricket and such was his longevity that he was able to describe with clarity and enthusiasm, only a month before his death, the sight of William Gilbert Grace (1848–1915) at the wicket at Lord's. 13 He was at Goodwood races only a fortnight before he died. 13 He was a less keen player of sport yet struck a bargain with Lady Marshall that if she would go the ballet with him he would play golf, which she much enjoyed. 13 Lady Marshall died in 1974 and Marshall remarried in 1979 to Joan Felicity Wilson-Brown who died just two months later in 1980. It was remarked that ‘Geoffrey never inflicted his own considerable personal tragedies upon even his intimate friends and he retained his splendid qualities to the very end of his life’. 13 He died, disabled by arthritis and increasing deafness, on 9 August 1982, aged 95.
Footnotes
Acknowledegments
The author would like to thank Mrs Harriet Metcalfe for reviewing this manuscript and Hull York Medical School (Medical Education Department) for allowing me the study time required for researching and writing it.