
Abstract
The Halsted radical mastectomy that prevailed in the first half of the 20th century derived its scientific basis from the ‘lymphatic permeation theory’ of William Sampson Handley an Honorary Senior Consulting Surgeon and former Vice President of the Royal College of Surgeons. Through his pioneering work in the cancer research laboratories at the Middlesex Hospital in London, Handley propounded the theory of centrifugal lymphatic permeation as the leading mechanism for the spread of cancer. This work won him worldwide renown and celebrated recognition in 1911 from the Royal College of Surgeons of England for the best work in the pathology and therapeutics in cancer. During his active life he was one of the great names and influences in the world of surgery. He held many roles at the Royal College of Surgeons and was involved with the international surgical fraternity. His philosophy of the uniqueness of the individual and his kind and courteous disposition won him praise from juniors, colleagues and patients alike. Although much of his work was rejected later, much still remains noteworthy in the history of surgery and cancer research.
Introduction
Surgery is the oldest method of treating breast cancer. The Halsted radical mastectomy, developed and first performed by William Stewart Halsted (1852-1922) in 1882, became the standard breast cancer surgery worldwide during most of the 20th century.1,2 This method was supported conceptually by the centrifugal permeation theory proposed by William Sampson Handley. It won national and international acceptance at the close of the 19th century. Handley was reported to have once said that he wished to be remembered only for his work on the dissemination of cancer by lymphatic permeation and the role of lymphatic stasis in its aetiology. This account aims to concentrate attention upon the life of Handley and the important theories that won him worldwide recognition as a distinguished surgeon and experimenter in the 20th century (Figure 2).
An illustration showing the advance of permeation along a small lymphatic, seen in the upper figure in longitudinal section, and in the lower figures as a series of transverse sections. 1 - normal lymphatic, 2 - lymphatic permeated by cancer cells, but not yet distended, 3 - the lymphatic distended by cancer cells, 4 - the lymphatic ruptured by the growing cancer cells and followed by an inflammatory reaction, 5 - the mass of degenerate cancer cells enclosed in a false capsule of newly formed fibrous tissue, 6 - the cancer cells are destroyed by contraction of their fibrous capsule. From Cancer of the Breast and its Operative Treatment
7

Early life and career
William Sampson Handley was an English surgeon who profoundly influenced the development of cancer research and surgery. Born in Loughborough, Leicestershire on 12 April 1872, he was the son of a chemist, Thomas Handley (1842-). Sampson Handley went on to study medicine at Guy's Hospital, London which he entered with a scholarship in Arts in 1889.
He qualified in 1895 with the Gold Medal in the MBBS and obtained the MD a year later and the FRCS in 1897 when aged only 25.4,5 Handley's junior appointment as House Surgeon was to Sir William Arbuthnot Lane (1856-1943), a respected surgeon, who was said to have influenced him greatly.
During his subsequent training he held a post as Demonstrator of Anatomy at Guy's Hospital, a role held exclusively by aspiring surgeons at the beginning of the century. With a substantially lower salary of a £100 during the post, Handley's funds were limited. He lived on campus above a poorly ventilated kitchen and subsequently developed carbon monoxide poisoning and lost his job after two years. 4 Then he took a post in general practice in Woolwich during which time he worked for and attained his MS (Master of Surgery).
In 1901 after a year in Woolwich he was appointed Surgeon to Outpatients at the Samaritan Hospital for Women and Children in London. Handley had a keen interest in cancer research, in particular the pathology of cancer, and in 1904, having already received the Astley Cooper Prize at Guy's Hospital, he was awarded the Richard Hollins Cancer Research Scholarship at the Middlesex Hospital.3,4
His application for the Middlesex Hospital Research Scholarship was supported in part by a testimonial from his former chief, Arbuthnot Lane, who wrote of him: ‘If afforded such an opportunity as this appointment offers, his scientific capacity must carry him rapidly into the front rank of his profession.’
4
His work in the cancer research laboratories at the Middlesex Hospital was organized by Senior Surgeon, Sir Alfred Pearce Gould (1852-1922), and was to be a pivotal step in his career.
William Sampson Handley. An illustration from the portrait by Herbert Olivier that hung in the Boardroom of the Middlesex Hospital.
3

Noteworthy recognition came in 1911 when he was awarded the prestigious Walker Prize by the Royal College of Surgeons for the best work in the field of pathology and therapeutics of cancer. 4
Upon expiry of his research scholarship, Handley was appointed to the surgical staff at the Middlesex Hospital. In 1955 he was awarded the Comfort-Crookshank Prize by the Middlesex Hospital for pioneering work on breast cancer. Although he worked mostly at the Middlesex Hospital, Handley worked in a Harley Street clinic as well as at the Bolingbroke and Putney Hospitals, now part of the St George's NHS Trust.
Leadership roles
In 1907 while at the Middlesex Hospital Handley served as Secretary of the Section of Surgery at the Annual Meeting of the British Medical Association in Exeter. Many years later, between 1934 and 1936, he was elected to serve on the Consultants and Specialists Group Committee of the Association and between 1935 and 1936 he served as President of the Section of Surgery of the Royal Society of Medicine.4,5
Handley was particularly enthusiastic about his roles at the Royal College of Surgeons (RCS). He was elected Hunterian Professor on six occasions (in 1905, 1910, 1915, 1917, 1921 and 1924). He became a member of the Council of the RCS in 1923, a role in which he served until 1943, and he was Vice-President in 1931-1933. 6 He gave notable lectures on ‘Chronic mastitis’ in 1931, the Bradshaw Lecture in 1934 and the ‘Makers of John Hunter’ in 1939.
Other prominent achievements included Honorary Fellowship of the American College of Surgeons in 1926, of the Medical Society of London in 1944 and of the Royal Society of Medicine in 1961. He was also a member of the Executive Committee of the British Empire Cancer Campaign and of the Committee of the Imperial Cancer Research Fund.3,4 During World War I in 1914-18 Handley served as captain in the Royal Army Medical Corps.
As a surgeon Handley was described as slow yet meticulous and who paid scrupulous attention to haemostasis. As a teacher he was popular with juniors, often described as quietly inspiring with tremendous enthusiasm for research and academia. He was said always to be looking for ‘something new, something which would add to knowledge, something which would engender progress’. 4
On carcinoma of the breast and the lymphatic permeation theory
In his post as Research Assistant at the Middlesex Hospital, Handley chose to investigate the genesis of cancer and its dissemination. He believed that, in order for carcinoma of the breast to be excised completely, its paths and methods of dissemination needed to be understood. His work in the investigation of the routes of dissemination of breast cancer began by his challenging of the embolic theory, an idea that was widely accepted at the time to explain the presence of remote metastases. 7 Handley exposed inconsistencies in this theory by referring to examples of breast cancer metastases to bones of the axial skeleton. He also revisited the work of Schmidt (1903) who had described the destruction of cancer cells in the small arteries of the lungs that prevented them from spreading haemato-genously. 8 Handley then demonstrated that cancer cells in the lymphatic vessels were not destroyed. He described the process of cancerous growth along the fine lymphatic vessels as ‘lymphatic permeation’ or simply ‘permeation’. 7
In his permeation theory, Handley outlined how cancer cells, by centrifugal growth along the small lymphatic vessels adjoining the primary neoplasm, ultimately succeed in penetrating the fine anastomotic plexuses at the periphery of the lymphatic area concerned as well as other surrounding lymphatic areas. The process was independent of the current of lymph and proceeded either in the direction of, or against, the lymph stream. He explained that regional lymph nodes initially filtered the tumour cells but only once the tumour had grown through them was it capable of reaching the blood stream and disseminating by the bloodstream. He concluded ‘it is no doubt that, although carcinoma often obtains access to the blood almost as early as to the lymph, its dissemination takes place almost entirely by the lymphatics and not by the blood vessels’. 7
Handley's theory of lymphatic permeation of cancer was outlined in ‘Cancer of the breast and its operative treatment’, published in 1906, for which in 1911 he received the Walker Prize for distinguished progress in the knowledge of pathology and therapeutics of cancer (Figure 3)4-6
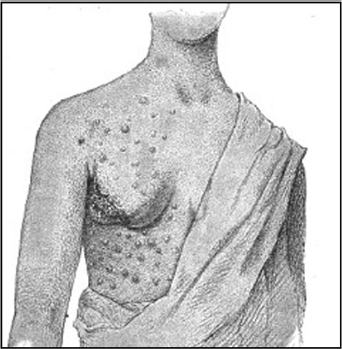
The drawing, reproduced from Mr Arthur Marmaduke Sheild's (1858-1922) work on Diseases of the Breast, shows how skin nodules have spread from the primary growth in all directions, involving an area around it which is roughly circular. From Cancer of the Breast and its Operative Treatment 7
Given the principles of lymphatic permeation, Handley stated that the object of the operation for breast cancer should be the removal of the lymph-vascular system that surrounds the primary growth along with the lymph nodes that may have been invaded. Handley's theory and its operative principles was welcomed by William Halsted, Professor of Surgery at John Hopkins Hospital in Baltimore in the United States, since it supported his radical mastectomy approach where the entire breast with its overlying skin, the pectoralis major muscle and the contents of the axilla were removed in almost every case of operable breast cancer. 2
Handley applied his ideas on the spread of cancer of the breast to other types of cancer, in particular to malignant melanoma of the skin and also to lupus carcinoma which he investigated extensively.
His immense interest in the treatment of breast cancer extended to his exploration of the impact of radiotherapy. However, the limited powers of X-ray therapy in his days meant that Handley resorted to using radium needles which he inserted into the chest wall of some of his patients after tumour resection in order to prevent recurrence from invaded mediastinal lymph nodes; in one patient long-term survival was achieved. 4
The theory of lymph stasis in the genesis of cancer
Some years later, in his The Genesis of Cancer, Handley proposed another theory namely that lymph stasis and its physiological consequences were an immediate cause of cancer. Previously he thought that identified irritants including arsenic, aniline and tar had in common the ability to produce lymphangitis and lymphatic obstruction that could result in malignancy. 9
In the case of breast cancer Handley observed that when lymphatic return from breast tissue was abnormal, for instance in cases of localized lymphatic obstruction, it gave rise to lymph congestion which acted as a stimulus to proliferation. Consequently papillomata appeared within the periductal lymphatics from which carcinoma then developed. The fact that chronic mastitis was able to affect single lobes of the breast and not exclusively the entire mass of breast tissue supported Handley's proposal that a local factor, rather than hormonal influence, must have accounted for the changes observed. That local factor, he proposed, was permanent lymph stasis and he demonstrated the sequence leading from chronic mastitis to cancer development using histological specimens taken from tissue within and surrounding carcinomatous growths. 9 Handley's idea that a local precancerous state must be recognized before cancer supervenes was a major contribution to medical knowledge.
Personal and family life
Handley married Muriel Rigby daughter of the Reverend Clayton Rigby of Great Yarmouth, in 1908. They had four sons and one daughter. He and his wife were described as gracious hosts by all who visited their London and country homes. Their Harley Street house was later destroyed by enemy fire during the World War I. One of his sons, Richard S Handley (1909-84), was also a surgeon at the Middlesex Hospital and a Member of the Council and the Court of Examiners of the RCS. He continued his father's line of study on the routes of dissemination of breast cancer, later publishing Invasion of internal mammary lymph nodes in carcinoma of the breast.5,6,10
Handley is often described as a man of small physique, gentle and earnest in manner. Though he was not naturally gregarious, he had a host of friends and good contacts among international lead surgeons. He was renowned for having a dry sense of humour that he exercised with great subtlety. Handley retired shortly before World War II. After retirement he was little occupied with surgical affairs although he still attended dinners given to members of the staff at the Middlesex Hospital as well as a dinner to celebrate his 80th birthday. Handley died on 18 March 1962 in his 90th year. A memorial service was held for him in the Chapel of the Middlesex hospital on 3 April 1962. His portrait by Olivier hung in the Boardroom of the Middlesex Hospital.3-5
Handley was once described as one of the most love-able personalities of the surgical profession. He left his mark by more than just his personality for he developed theories that won widespread acceptance at the time and secured his name as a leader in cancer surgery. In the light of modern advances indeed he had underestimated the importance of spread of cancer through the vascular system. However, it should also be remembered that most of Handley's work remains and deserves credit, in the history of breast cancer surgery in the 20th century.
Footnotes
Acknowledgements:
We would like to thank the librarians at the Royal College of Surgeons of England for their invaluable assistance.