
Abstract
Two centuries ago, electricity was being used for the treatment of paraplegia and trials were taking place in France. This study aims to identify cases of traumatic paraplegia treated with electricity in the 19th century in order to assess the therapeutic benefit. Only four such cases were identified, none with a complete transection of the spinal cord since these patients would have died from pressure sores and urinary tract infections. The personalities involved, William Gull, William Erb, Guillaume Duchenne and Cyril Henry Golding Bird are portrayed and contemporaneous views on electrotherapy analysed. While the four patients apparently benefited from the treatment, the lack of follow-up and the incomplete data prevented a definitive conclusion on the therapeutic value of electrical treatment in traumatic paraplegia.
Electricity has been used to treat patients for 2000 years. It has been applied indiscriminately to a wide variety of conditions of an indeterminate nature that defy scientific analysis and are largely unrecognizable today. The patients were probably suffering from functional disorders and showed a variety of manifestations of hysteria. It is hardly surprising that the orthodox medical establishment viewed it with suspicion and considerable reservation. It became the monopoly of quacks and charlatans since any results could be attributed to suggestion, placebo effect, spontaneous recovery or to a mixture of these.
Surprisingly, electricity was applied for the treatment of spinal paralysis more than 200 years ago. The patients thought most likely to benefit were suffering from paralysis or involuntary movement (chorea). In order to assess the benefits, it is necessary to study a group of cases with a well-defined prognosis. Such cases are very difficult to identify in the literature of 200 years ago. However, patients suffering from traumatic paraplegia fulfilled this criterion since the outcome was fully recognized then. Brockliss described how in 1782 the Académie Royale de Médecine sent Chambon de Montaut to the Military Hospital at Bourbonne-les-Bains to assess the usefulness of electrotherapy and water therapy on paralysed soldiers. 1 In 1784 Mauduyt in his mémoire described the use of electricity on patients paralysed from the waist down and recommended early treatment for better results. 2
Methodology
Licht 3 identified 100 publications from the 18th century and a total of 900 from the 19th century describing the use of electricity treatment but the emphasis was on the dramatic personalities of the practitioners involved and the novelty of the equipment rather than on individual case descriptions. The present study involved a literature review of 42 publications describing paraplegia and/or electrotherapy and 15 primary sources were analysed in detail. The review yielded 13 cases of paraplegia (see Appendix) but only four patients with traumatic paraplegia treated with electricity were identified and these were in the writings of Gull 4 and Erb. 5
Sir William Withey Gull FRCP (1816-90)
Gull (Figure 1) was born in Colchester. His father kept a wharf but died young and Gull was brought up by his mother on an estate owned by Guy's Hospital. He came to the attention of Benjamin Harrison, Treasurer of Guy's Hospital, when he was visiting the estate and under his patronage he studied medicine at Guy's. He graduated in 1841 and obtained his MD from the University of London, gaining the Gold Medal in 1846. He held honorary degrees from Oxford and Cambridge Universities and was a Fellow of the Royal Society.
Sir William Withey Gull. Lithograph. Reproduced by kind permission of the Wellcome Library, London
Gull published several authoritative papers on myxoedema and anorexia nervosa and was a pioneer in diseases of the spinal cord. 6 After successfully treating the Prince of Wales for typhoid in 1871 and being appointed physician-in-Ordinary, a largely honorary appointment, in 1788, Gull became a fashionable doctor with a brilliant career both at Guy's Hospital, where he worked for 18 years following his appointment in 1851, and in private practice, amassing a large fortune. Despite being a prominent figure in medical and scientific circles, he was described as very authoritarian. He resented nurses having too much influence on the wards and believed that all authority should rest with the doctors. He was very disdainful of his colleagues but he was a general physician and it is of great interest that, despite his antagonism to specialization, he realized the value of electricity and used it on his paralysed patients. 4
William Heinrich Erb (1840-1921)
Erb (Figure 2) was born in Bavaria, Germany and trained as a doctor in Heidelberg. In contrast to Gull, Erb was a full-time neurologist. In 1868 he introduced the method of electrodiagnosis by galvanic and faradic currents, developing an electrophysiological method for detecting denervation in muscle and this indeed popularized the use of electrodiagnostics in neurology. In 1880 he became Director of the Medical Clinic at Leipzig where he set up a neurological outpatient clinic and later he was appointed Professor of Neurology at Heidelberg. He followed Duchenne in the extensive development of electrotherapy and his textbook Handbuch der Elektrotherapie became the standard reference work for neurologists at that time.
5
Wilhelm Erb, Neurologist. Reproduced by kind permission of the Wellcome Library, London
The pre-eminence of German scientific medicine had already led to the emergence of neurology as a specialty. Doctors wishing to follow a scientific career, including Harvey Cushing (1869-1939), Henry Head (1861-1940) and Gordon Holmes (1876-1965), all went to Germany to pursue their studies.7,8
Case histories
William Gull (1896): case 15
A 23-year-old stoker was struck by a fist on the side of his neck at the junction of the skull and the cervical spine some five years before presentation 4 . Recently he had a choking sensation and occasional difficulty in passing urine. He received a second blow to the back of his hand from a falling piece of iron. He experienced immediate loss of power in his right upper limb which persisted for six weeks followed by an incomplete recovery with difficulty in swallowing and weakness in his lower limbs. The bladder was paralysed and he required catheterization for several weeks. He recovered some power in his lower limbs to such a degree that he could walk about.
Examination showed total loss of power in his right upper limb and partial loss of power in his left upper limb and both lower limbs. Bladder and bowel control was lost. He received ‘electricity’ but details of the treatment are lacking. He had fluctuating symptoms and was discharged with a walking stick. He was readmitted four months later with severe lower limb paralysis and paralysis of his intercostal muscles. This progressed and in a few weeks he became totally paralysed and died six months later. Postmortem showed swelling of the cervical cord but doctors had difficulty in forming an opinion on his condition although they thought he suffered from a lesion of the spinal cord related to trauma.
This patient clearly suffered an incomplete spinal lesion but its relationship to trauma is debatable.
William Erb (1883): case 18
A 23-year-old soldier fell from his horse and suffered immediate back pain. He developed pleurisy and a gastric disorder. Four months later the pain became severe and spread to the limbs with hyperaesthesia and irritation and numbness in his legs accompanied by twitching, diminished motor power and incontinence of urine (ref. 5 p.161).
Examination showed normal pupils, diminished sensation, and tenderness of the spine. He was treated by galvanism with electricity applied through the skin over the spine. After eight sessions the pain in the legs was relieved. He returned to duty but suffered a relapse and again was treated by electricity.
Dr Hitzig treated this patient for four months. Although the case description is brief this is clearly a case of delayed paralysis four months after the initial injury but probably not a traumatic lesion of the spinal cord. There was no postmortem. The diagnosis at the time was meningitis spinalis subacuta and the improvement after electric treatment may have been spontaneous.
William Erb (1883): case 20 (p.162)
A 55-year-old labourer fell from a tree upon his feet and buttocks, sustaining an immediate paralysis of his lower limbs with pains in his back. At first his legs were paralysed for about a week; there was no muscular atrophy and then a gradual return of power. There was no loss of sensation. Micturition was normal. On examination he could stand upon tiptoe with difficulty. Tendon reflexes and cutaneous reflexes were retained. Electrical excitability was diminished and he received galvanic treatment through the skin to the spine and the legs with striking results. After 22 sittings, the patient could walk and was discharged.
This patient sustained an incomplete lesion of the spinal cord and his recovery might have occurred spontaneously irrespective of the treatment.
William Erb (1883): case 22 (pp.162-163)
In 1870 this 22-year-old soldier received a bullet wound in the cervical vertebrae. He developed complete paralysis with anaesthesia of his lower limbs extending as high as the thorax with retention of urine which remitted after four weeks. There was a gradual return of power and sensation particularly in the left lower limb. He was seen two months after his gunshot wound. There was tenderness over his cervical vertebrae and sensation was restored completely and he had a little power in his right lower limb. He had involuntary spasms. Electrical excitability was well preserved in his lower limbs. Galvanic treatment was applied through the skin to the spine, particularly to the cervical vertebrae. There was a rapid improvement in his condition and he was able to stand, put weight upon his left lower limb and move his right leg more freely. After 10 electrotherapy sessions he could walk around his bed and after 12 he could stand securely and walk a few paces.
This was an incomplete cervical lesion of the spinal cord and this patients’ recovery might have been spontaneous irrespective of electrotherapy.
Results
The Appendix summarizes the 13 cases of paraplegia identified in the literature and the results of the four patients who received electrical treatment.
All the patients were paralysed as a result of traumatic injuries to the spinal cord; none had suffered a complete transection of the spinal cord - all were incomplete lesions, two with cervical lesions and two with lower lesions of the spinal cord. Two of the patients developed immediate paralysis and two showed delayed onset paralysis. Bladder function was impaired in three patients indicating severe involvement of the spinal cord.
Three patients received between eight and 22 sessions of galvanism applied to the skin and over the spine. One received ‘electricity’ but there are no other details.
All the patients improved after receiving electrotherapy; all recovered the ability to walk and one experienced pain relief. One patient died six months after injury but three survived and were discharged later.
Discussion
Paralysis in the 18th and 19th century was a medical term used widely to describe various conditions including apoplexia, hysteria, epilepsy and even transient paralysis due to colds, rheumatism, gout and stroke. 9 The spinal cord was the ‘Cinderella of neurology’. 10 Before the publications of Charles Bell (1774-1842) the cord was not thought to have independent function but merely to be a conductor of impulses from the brain. 11 It was not until Duchenne, Erb and Charcot's seminal studies that the new discipline of neurology emerged. 12 The case descriptions were so ill-defined that it was difficult to establish whether paralysis was spinal or cerebral in origin.
The development of paraplegia as a direct result of traumatic injury has to be demonstrated clearly but the term ‘paraplegia’ was not used until the end of the 19th century. 5 The more remote from the time of trauma, the greater the doubt about this relationship and so this survey had to rely on the immediate onset of paralysis or postmortem findings to diagnose traumatic spinal cord injuries. The difficulties arose when the paralysis developed more than 48 hours after the accident as in the case of a spinal abscess (Gull case 22) and the two cases of odontoid dislocations (Gull: William B and MH). 4 Even today, with CT scans, X-rays and imaging, the diagnosis of fractures of the foramen magnum can be difficult as there is more room for the spinal cord at this level. Odontoid dislocations can produce either incomplete lesions of the spinal cord or immediate death as in judicial hanging. Sometimes paralysis appears many years later in which case the relationship to trauma becomes increasingly tenuous.
Not a single patient with a complete traumatic lesion of the spinal cord was treated with electricity since the five acute patients identified died of pressure sores and urinary tract infections without receiving electrical treatment (see Appendix). There were many case descriptions by Paré, Astley Cooper, Bell and Brodie but both Astley Cooper and Bell described how patients with paraplegia due to complete lesions of the spinal cord inevitably died soon after injury and before any form of treatment could be applied. 7 Today a review would only include patients with complete lesions of the spinal cord since these have a known prognosis. When the patient does not regain power and sensation after 48 hours and the lesion remains complete, there will be no recovery. Studying patients with incomplete lesions is beset with difficulty since the condition may remain stationary or may improve spontaneously or deteriorate due to neglect, immobility or the development of cystic changes in the spinal cord. Consequently, it is difficult to apportion any improvement to the electricity treatment. Medical disorders including multiple sclerosis, transverse myelitis and cases of Pott's paraplegia can also have an unpredictable prognosis and would be excluded.
The methodology used for the electricity treatment is vague and cannot be evaluated properly. At the time there were seven different forms of direct stimulation: galvanization, faradization, electro-puncture, direct stimulation of the muscles and stimulation of the spine, reflex stimulation and skin stimulation. There are no details of the duration of the treatment, the method of application, the frequency or the intensity. This is inevitable in any retrospective study since vital information is omitted or considered not important enough to be recorded, a view expressed by Head. 13
How did the medical profession perceive electro-therapy in the 19th century and what can we learn from the treatment of spinal disorders in particular?
Before the 19th century electrical treatment was the monopoly of charlatans and quacks including Dr James Graham (1745–94), Dr Franz Anton Mesmer (1734–1815), Dr Harry Lobb and Gustavus Katerfelto (c1743–1799) (Figure 3). By selecting suggestible willing victims with indefinite illness, these powerful personalities achieved popularity, prestige and enormous financial success, which ignited the jealousy, hatred and suspicion of the orthodox establishment.
14
Electrical treatment was administered with great showmanship, in unsavoury places including the Adelaide Gallery or in the homes of unorthodox practitioners including William Hooper Halse, the well-known ‘medical galvanist’.15,16
Two unorthodox medical practitioners, J Graham and G Katerfelto battling against each other, each surrounded by objects symbolizing his practice (Etching, 1783). This shows how interested the general public was in the use of electricity. Reproduced by kind permission of the Wellcome Library, London
At the turn of the century, attitudes changed and electricity treatment gained respectability when electrical rooms were established in the major London teaching hospitals – the Middlesex (1767), St Bartholomew's Hospital (1777), St Thomas's Hospital (1799), Guy's Hospital (1836) and The National Hospital for the Paralysed and Epileptic in Queen Square (1867).17,18
Electricity treatment gave medical men an opportunity to build a reputation and affluence but, before this could be achieved, the discipline had to gain respectability among orthodox practitioners and be used as a recognized form of treatment. John Birch had used electricity treatment at St Thomas's as early as 1815 but its acceptance in mainstream medicine was achieved largely through the work of CH Golding Bird at Guy's Hospital after the establishment of an ‘electrifying room’ in October 1836 at the request of Benjamin Harrison, the powerful Treasurer of Guy's.
Golding Bird was a respected general physician with a scientific background in chemistry and with an established reputation (Figure 4). He applied his expertise in chemistry to write a chapter on the composition of breast milk in Astley Cooper's book on the breast. His position was enhanced through the patronage of Thomas Addison (1793–1860) and Astley Cooper both of whom were on the Staff at Guy's Hospital. In 1837 Golding Bird joined the London Electrical Society to improve his technical understanding of electricity. He understood the need to transform electrical treatment from a popular and empirical practice to a rational and orthodox discipline administered under controlled conditions in the hospital. He established a school of ‘electricians’ at Guy's Hospital with prominent figures Benjamin Guy Babington (1794-1866), Henry Marshall Hughes (1805-58) and William Gull. Although Gull complained of irregular attendance on the part of the patients, the large numbers of working class patients being subjected to electricity at Guy's provided Golding Bird with a unique opportunity for correlating and standardizing the results of treatment in the electrifying room. Patients were regarded as experimental subjects and every case was recorded by a student or the doctor. By the middle of the 19th century, electricity was no longer used indiscriminately or as a last resort but was targeted to chorea and hysterical paralysis.
15
Portrait of Golding Bird by Alexander Craig. Reproduced by kind permission of the Wellcome Library, London
The protagonists
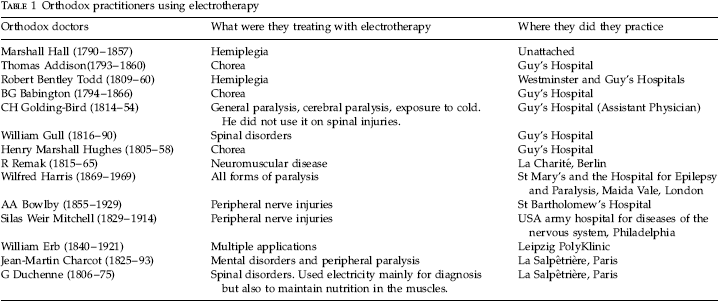
Orthodox practitioners using electrotherapy
… it was whilst brooding over the humiliating failure of a whole host of remedies employed in one of such cases and which will be described in the sequel that as a last resort, I determined upon giving electricity a fair trial. 20
On the continent specialization was already well advanced. Erb, Duchenne and Charcot were all specialists in neurology, publishing papers detailing the patho-physiology of neurological conditions. Erb's book on electricity was regarded as the ‘Bible’ and he was a fervent electrotherapist:
… I am not guilty of exaggeration when I say that the most curative effects not infrequently astonish even the most experienced physician by their magical rapidity and completeness. 5
The opponents and neutral observers
Not everyone was enthusiastic. Critics were cautious and discriminate. In 1888 WR Gowers, doyen of clinical neurology stated emphatically that electricity treatment was ineffective in treating softening of the brain, ocular paralysis, migraine headaches, paralysis agitans, tabes dorsalis and muscular atrophy. 21 Nevertheless, he did recommend its use in cases of hysterical paralysis and for the early examination of muscles in acute spinal paralysis. 22 Duchenne, 23 the great advocate of electricity for diagnosis, was equally sceptical of its effectiveness as a means of treatment and he always correlated treatment to pathology. In his standard text of medical practice, Jonathan Pereira (1804-53) listed electricity treatment as a treatment of doubtful or unproven efficacy and yet he quoted favourably the work of Addison and Golding Bird on the electrical treatment of chorea. 24 By contrast, Paul Julius Möbius (1853-1907) maintained that electricity treatment was for the most part just psychotherapy and suggestion. 21
Contemporaneous textbooks of medicine and textbooks of neurology hardly mention the use of electricity treatment although the latter were devoted mainly to diagnosis and pathology. The exceptions include Henry Charlton Bastian's (1837-1915) work that mentioned electricity treatment for hysterical paralysis and also reported some occasional benefit in cases of spinal paralysis and Byron Bramwell's (1847-1931) work that also endorsed electricity treatment.25,26
The overall picture is of a remedy that was regarded with some scepticism and reserve throughout the medical profession and only deemed appropriate for specific conditions - chorea, paralysis and hysteria once orthodox treatment by a course of drugs had been tried.
Indications and contraindications to electricity treatment in traumatic spinal cord injuries
The paucity of descriptions of traumatic spinal cord injuries treated by electricity is not because there was a lack of interest but, on the contrary, paralysis was considered to be a condition ‘par excellence’ for electricity treatment yet such patients did not survive. Doctors were interested in treating spinal cord conditions but were careful to link the pathology of the spinal cord injury with the indications and outcome of treatment. Not all patients were suitable and in 1804 Wilkinson discredited electricity treatment in cases of paralysis:
When paralytic affections arise from organic defect, as in cases of palsy of the lower extremities, from diseased spine, no good effects can be expected to result from the application of galvanism. 27
Golding Bird concurred and suggested that the situation could be made worse by the application of electricity treatment:
In true spinal paralysis depending upon organic lesion, the electro-magnetic current often does mischief, especially where there is subacute inflammation, or a highly irritable state of the spinal marrow. 19
Duchenne also endorsed Wilkinson's findings and demonstrated through meticulous physiological research in acute cases that when the muscles failed to respond to electrical stimulation they were not in continuity with the spinal cord and as a result the prognosis was poor (the reflex arc had been destroyed). When, on the other hand, the muscles were excitable and continuity with the spinal cord had been preserved immediately after injury (the reflex arc was preserved) then it was desirable to commence electricity treatment early so that when recovery did occur it would not be masked by the secondary effects of atrophy and contractures. 28 Erb 5 disagreed with Duchenne and would only apply electricity after a traumatic lesion of the spinal cord had entered its chronic phase, with the aim of restoring function in individual muscles.
Erb recognized the limitations of electricity treatment especially in cases of paralysis from cancer, chronic inflammation, severe degenerative change, haemorrhage and neoplasm. He understood the dangers of using electricity on the spinal cord where results are much scantier than the brain. 5
Trials on the benefits of electrotherapy
Scepticism about the value of electric therapy did not emanate just from individual doctors. The controversies about the application of electricity led to confusion and there was a demand for an objective authoritative enquiry as to the benefits of treatment. Committees were set up to investigate electrotherapy formally.
In 18th century France, where medicine was administered centrally from Paris, the French Academy instigated trials to evaluate the therapeutic use of electricity all over the country. Jean Antoine Nollet (1700-70) was given access to 12 paralysed soldiers from the Hotel Royal des Invalides to perform his experimental research. Antoine Louis (1723-92), Surgeon at the Salpêtrière Hospital in Paris, together with Pierre Mauduyt (1732-92) and Nicolas Chambon de Montaut (1748-1826) produced first-hand accounts of the use of electricity in cases of paralysis but these case descriptions are non-specific.29,30,2,31 Chambon's manuscript dwells heavily on the hospital facilities, the baths, the atmospheric conditions, the need for ventilation in summer and heating in winter, and on the difficulties of studying both water and electric therapy concomitantly. His report reads like a research proposal, listing areas of study for which he asks the commission for additional funding. There is little information on the electricity treatment and the outcome for individual patients and, furthermore, most patients suffered with hemiplegia.
By contrast, in England medicine was fragmented and regulation of the profession chaotic. The Colleges were concerned mainly with disciplinary matters and the regulation of medical practice, not with therapeutic indications. The Medicochirurgical Society was influential and sought to offer guidance to its members. In 1873 members of the Medicochirurgical Society set up a committee, under the chairmanship of Charles Bland Radcliffe (1822–89) to investigate the benefits of electrotherapy. The committee met 16 times and was very influential. Sir J Russell Reynolds (1828– 96) was a member. They visited The National Hospital for the Paralysed and Epileptics at Queen Square and tested patients and committee members on an insulated couch. Dr Radcliffe suffered from a headache, a boy from aphonia, another patient suffered from paralysis agitans, another from suspected food poisoning and one of the doctors on the committee had rheumatic pain in his hip which was cured. They thought that treatment should be carried out in a hospital and they recommended regular inspections. They issued a form to try and standardize the treatment but still they could not come to any meaningful conclusion since the committee was beset with the same problems as encountered today – lack of standardization of methods and patients, internal quarrels, poor attendance and complaints. Eventually they produced a provisional report and dissolved the committee. 32
Conclusions
In 19th century England the protagonists of electricity treatment were highly regarded doctors and the treatment was accepted albeit with some reservations. While most acknowledged the benefit of electricity treatment in cases of paralysis, there were very few patients with spinal injuries treated with electricity in the 18th and 19th centuries and no patient with a complete transection of the spinal cord received galvanic or static electricity treatment since they all died as a result of pressure sores and urinary tract infections before treatment could be started. The treatment did have a beneficial effect on patients with incomplete lesions but in view of the natural history of incomplete lesions it is not possible to attribute all the improvement to the electricity treatment.
The approach in England was different. Specialization, in particular neurology, was well advanced on the continent and practitioners carried out the treatment themselves and looked to improve matters by linking pathology with the treatment outcome whereas in England treatment was on an ad hoc basis. Nevertheless, both on the continent and in England practitioners made efforts to formally assess electricity treatment in order to give it respectability. Among the chronic cases with spinal cord injuries, poor patient attendance at follow-up made it difficult to accumulate meaningful information about the long-term benefits of electrical treatment as Erb indicated:
The fact should not be concealed that the electro-therapeutics of diseases of the spinal cord presents an extraordinary large number of failures, indeed much larger than the successes. This is to be expected however from the nature of the disease in question. 5
Footnotes
Acknowledgements:
We are grateful to the Wellcome Library for giving us permission to reproduce the illustrations and to Dr Hugh Baron and Dr Eric Nieman for their constructive suggestions.
Appendix
Summary of cases of paraplegia identified in the literature including the results of the four patients who received electrical treatment. Paralysis cases summary