
Abstract
Objectives
Screening for colorectal cancer by biennial testing for faecal occult blood is being introduced in the UK from 2007. We examine the likely impact of the programme, in terms of reduced mortality, lives saved and changes in incidence, over the next 20 years.
Setting
Projections of incidence and mortality of colorectal cancer in England, and the policy that has been adopted for screening in England (biennial at ages 60–69 from 2007, then 60–74 in 2010).
Methods
The results are based on the output of a simulation model that has been used to examine cost-effectiveness of screening policy options, with two scenarios regarding compliance with screening; both assume that 20% of the population will never attend for screening, but attendance of those who do is modelled either as a random 60% or 80%, at each screening round.
Results
The decrease in mortality rates expected 20 years after introducing screening is 13–17% in men and 12–15% in women (depending on the attendance levels). The model predicts an initial rise in incidence, followed (after six to seven years) by a fall, so that there is little net change in the number of cases detected over a 20-year period.
Conclusion
Percentage changes in mortality seem modest, but the projected saving in terms of numbers of lives is not negligible – 1800–2400 per year by 2025 in England (equivalent numbers are 2200–2700 in all over the UK). Newer screening modalities may improve on these projected results.
INTRODUCTION
Cancer of the large bowel (colon and rectum) is a major problem in the UK. The most recent data 1 indicate that colorectal cancer ranks third in terms of numbers of new cases (36,109 in 2004) and second in terms of mortality from cancer (16,092 deaths in 2006). Male bowel cancer incidence rates rose slowly by an average of 1% each year between 1979 and 1999; since then there has been a slight decrease. Over the same period, the female rates have changed very little. On the other hand, in the 10 years between 1997 and 2006, the bowel cancer age-standardized mortality rates in the UK fell by 17%. This fall in mortality affected all age groups with the largest fall in the 40–69 age groups for men and the 55–79 age groups for women.
Three randomized controlled trials have shown that faecal occult blood testing (FOBT) every two years has the potential to reduce colorectal cancer mortality in a target population by up to 20%. 2 For individuals attending at least once for screening by FOBT, the reduction in the risk of dying from colorectal cancer is 25%. 3 Evidence for colorectal screening was reviewed by the National Screening Committee (NSC), which recommended that two pilot studies be set-up to evaluate mass population screening. 4 In 2000, the UK Colorectal Cancer Screening Pilot was launched in England and Scotland to evaluate the feasibility, practicality and acceptability of introducing a biennial FOBT screening programme within the National Health Service (NHS) for people aged between 50 and 69 years. These pilots reported favourably 5,6 with very similar results to the randomized trial in Nottingham. 7
Following government approval, a NHS Bowel Cancer Screening Programme (biennial FOBT screening for people aged 60–69) is being phased in over three years in England beginning in 2007, whereas a Scottish Bowel Screening Programme began in 2007, inviting people aged 50–74 years. In England 8 , the programme is being rolled out nationally and will achieve nationwide coverage by 2009. Five programme hubs operate a national call and recall system to send out FOBT kits, analyse samples and despatch results. Each hub is responsible for coordinating the programme in its area and works with up to 20 local screening centres. The screening centres provide endoscopy services and specialist screening nurse clinics for people receiving an abnormal result. Screening centres are also responsible for referring those requiring treatment to their local hospital multidisciplinary team. Currently (2008), the English programme offers screening every two years to all men and women aged 60–69. People over 70 can request a screening kit when the programme reaches their area. From 2010, screening will be extended to include individuals aged 70–74, including people never screened and those who have had a previous test.
In this paper, we examine the likely impact of bowel cancer screening. We have chosen to do so for the population of England (which accounts for some 84% of the UK population), but the results will be broadly applicable to the whole of the UK, despite variations in the precise screening programmes in the different countries, and mortality rates approximately 20% higher in Scotland than in England, and 9% higher in Wales.
METHODS
Projections of cancer incidence and mortality
Mortality rates from colorectal cancer (ICD 10 codes C18–C21) in England for 1971–2005 and incidence rates for 1975–2004, by sex and five-year age group, were projected until 2025 and 2024, respectively, using the NORDPRED package.
9
Briefly, rates are projected into the future using age–period–cohort modelling of past trends. Møller et al.
9
compared different methods of projecting the modelling of past trends and found that the best predictions were made using the so-called power cut-trend model. The power model assumes that the rates depend on the sum of individual effects raised to the power of 5, so the model becomes

Effect of screening
The effects of screening were drawn from the results of a computer model of the colorectal cancer screening programme, commissioned by the NHS Cancer Screening Programmes on behalf of the Bowel Cancer Screening Working Group, from the University of Sheffield School of Health and Related Research (ScHARR). 10,11 The model uses a state transition approach to simulate the lifetime experience of individuals with normal healthy epithelium, through to the development of low-/high-risk adenomatous polyps, through to the development of malignant carcinoma and eventual death. The model is divided into a series of discrete health states that represent the underlying natural history of colorectal cancer and the impact of screening in reducing colorectal cancer incidence and mortality. The benefits of screening are modelled (i) through the avoidance of cancer in individuals who have adenomatous polyps with malignant potential removed following a positive screening test and (ii) through the identification of patients who have preclinical colorectal cancer detected through screening who would have otherwise presented symptomatically at a later stage of the disease. Some of the parameters used in the development of this model were derived from the Nottingham trial; 7 however, the majority of model parameters were drawn from the literature; they are described fully in the original articles. 10,11 The sensitivity of the FOBT to detect colorectal cancer was set rather low, at 41%, and a variety of assumptions (based on literature reviews and expert opinion) were made concerning the natural history of polyps and the ability of screening to detect them. As in all modelling, some input parameters were unknown, or quantitative data were sparse, so that their values were calibrated against the production of realistic outputs.
The model output is in terms of mortality and incidence rates of colorectal cancer for a hypothetical cohort of individuals passing through life with current risks and natural history of colorectal cancer, with and without the implementation of screening. Results were obtained for biennial screening with FOBT between ages 60–69, 60–74 and 70–74 under two different assumptions concerning compliance and attendance with screening. These were the following.
Scenario 1. A ‘realistic’ scenario, whereby there will be 20% of individuals who will never attend (non-compliers), whereas a random 60% of the remainder, who are eligible for screening, attend at each round; Scenario 2. An ‘optimistic’ scenario, with the same level of non-compliance, but 80% attendance among compliers at each round. For both scenarios, the model assumes that 80% of persons with a positive FOBT will attend for follow-up examination (colonoscopy with removal of any polyps or cancers detected).
To simplify the estimation of the effects of screening at the national level, it was assumed that
Screening begins in 2007, and one-third of the population at risk enters the programme in that year, and one-third in each of the next two years (2008 and 2009); Screening takes place at ages 60–69, with no additional testing at ages above or below these ages; In 2010, screening is extended to include individuals aged 70–74, including persons never screened and those who have had a previous test.
The ScHARR model simulates the effects on incidence and mortality of a period (5, 10 or 15 years) of biennial screening introduced at a specific age (60 or 70) on a single birth cohort as it ages. The relative risk of mortality (or incidence) following one, two, three, etc. tests is relatively independent of the age at first test, so we can simulate the situation where, as in the NHS Bowel Cancer Screening Programme, individuals in a whole age group (60–69, 70–74) enter the programme in a specific year.
Sensitivity analysis
The effects of different assumptions concerning the sensitivity of FOBT were examined by comparing outcomes based on a uniform distribution of values for polyps (in the range of 0–10%) and for cancer (in the range of 30–50%). Results of the most and least favourable outcomes from the range of possibilities provide the extreme values around those from the base-case analysis (FOBT sensitivity of 5% for polyps and 41% for cancer). We also examined the projected outcome of screening under the assumption that 90% of screen-positive individuals would attend for diagnostic colonoscopy (rather than the base-case 80%), and assuming that sensitivity of FOBT for polyps is 0% (which allows the relative effects of detection of occult cancer and pre-cancer [polyps] in the base-case model to be quantified).
RESULTS
Figure 1 shows the age-specific mortality rates from colorectal cancer in England, as observed in 1971–2005 and projected until 2025. The expected rates, in the presence of screening according to Scenario 1, are also shown. In the age groups being screened (60–69, from 2007), some reduction in mortality rates is obvious at once (in 2008), and the benefit in terms of reduced mortality becomes greater at 65–69 than at 60–64, because of the larger number of tests that the older individual will receive. Eight years after screening is introduced, the reduction in mortality at ages 70–74 exceeds than that at 60–69; by 2025 (19 years after screening is introduced), the reductions are 25% at 70–74 and 21.4% at 65–69. The effects of screening are also marked in the older age groups: mortality reductions of 24.5% at ages 75–79, 11.5% at 80–84 and 2.3% at ages 85 and older, although of course benefit at older ages is not seen until several years after screening is introduced.
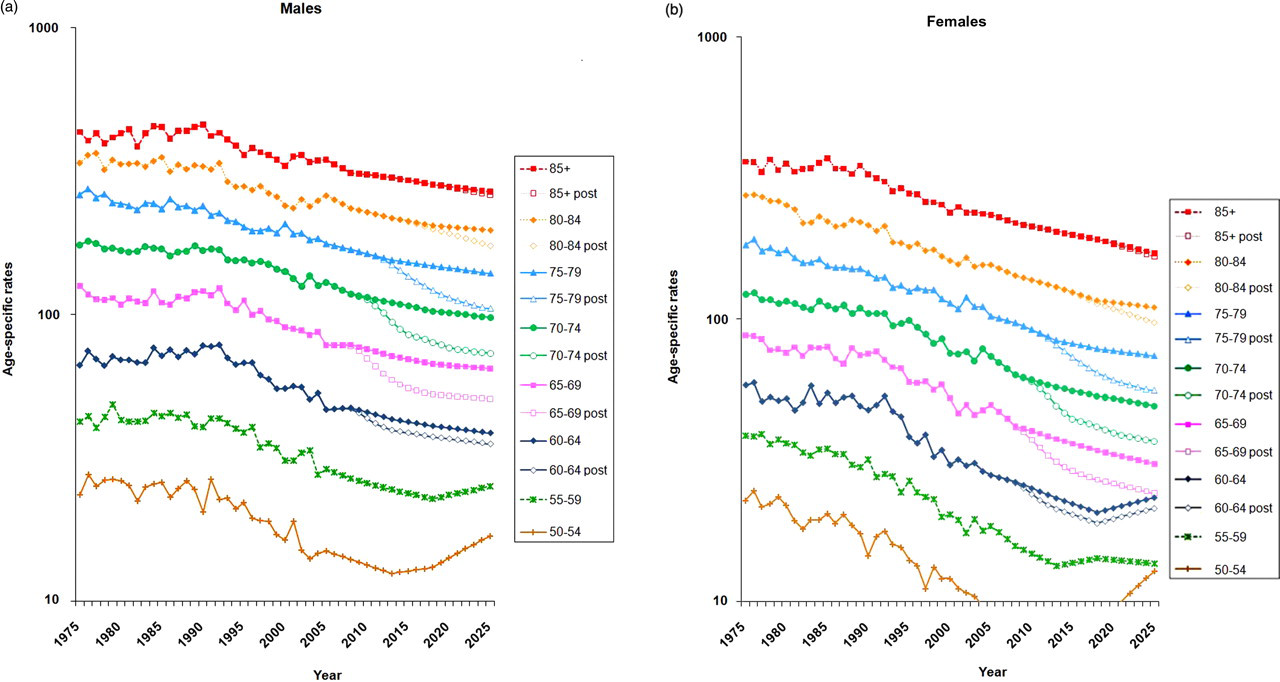
Projections of age-specific mortality rates (per 100,000) for colorectal cancer in England: with and without screening (at ages 60–69 from 2007/2009 and 60–74 from 2010). (a) Males and (b) females
The ScHARR model also predicts an effect on the incidence of colorectal cancer, as the model is based on the natural history of cancer, from polyps, to invasive disease, to death. Screening will advance the diagnosis date for cancers, so that, immediately following a test, there will be an increase in incidence, which will be compensated by a later fall. The detection and treatment of polyps should also result, after several years, in a reduced incidence of colorectal cancer. The model results are shown in Figure 2. Incidence increases in individuals being screened for the first time, which includes those in the age group of 60–64 after 2007. However, sometime after entering the programme, incidence is expected to fall. This is seen in the age group of 65–69 year about seven years after screening is introduced, and falls are evident too in older individuals, after they exit the screening programme.

Projections of age-specific incidence rates (per 100,000) for colorectal cancer in England: with and without screening (at ages 60–69 from 2007/2009 and 60–74 from 2010). (a) Males and (b) females
The predicted effects on age-standardized mortality rates of colorectal cancer, based on the two different two sets of assumptions about compliance and attendance, are shown in Figure 3. For males, the percentage reduction in the age-standardized mortality rate 19 years after screening is introduced (in 2025) is 13.1% in the ‘realistic’ scenario and 16.7% in the ‘optimistic’ one. The equivalent reductions for females are 11.8% (realistic) and 15.1% (optimistic).
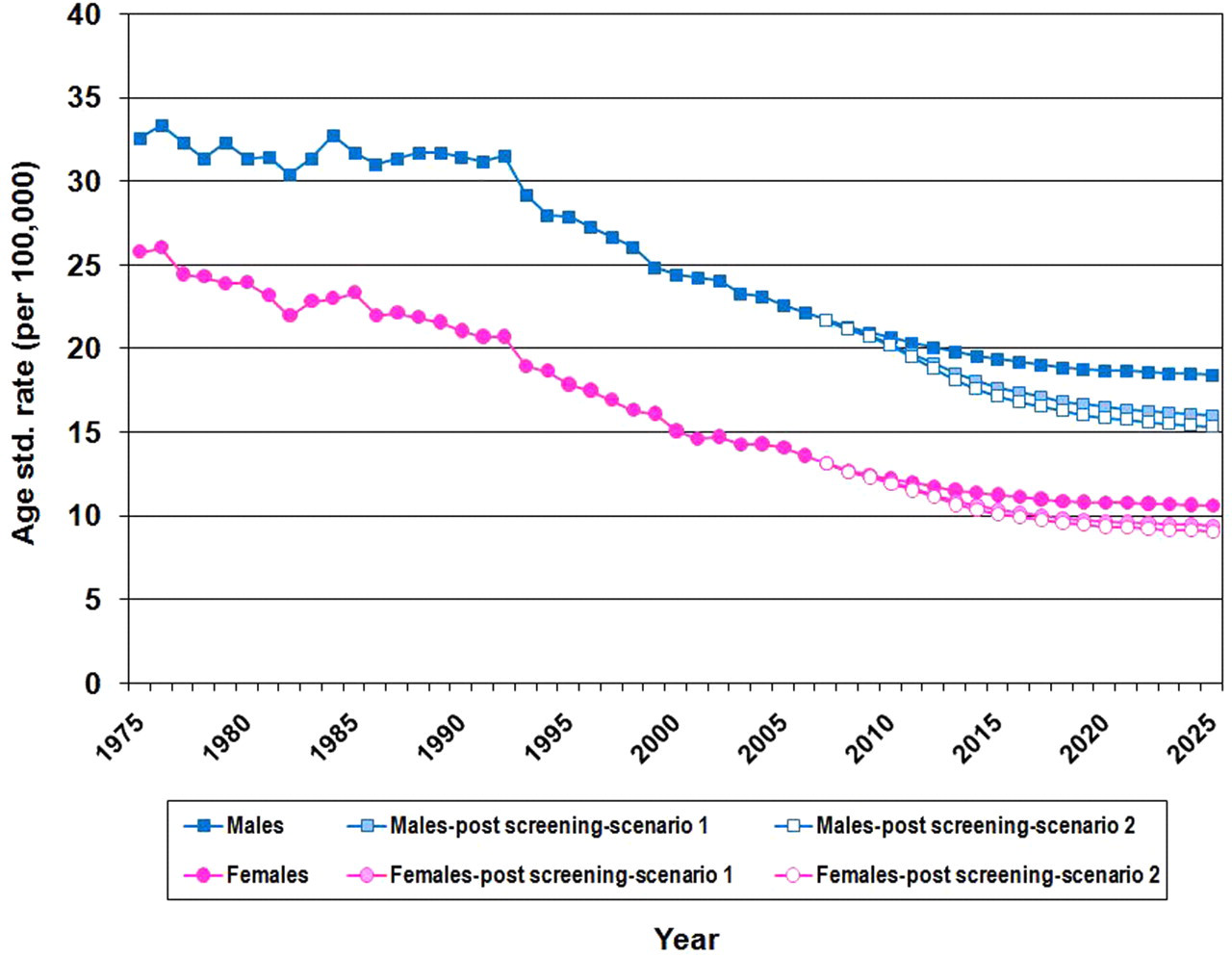
Actual and projected age-standardized (European standard) mortality rates per 100,000 for colorectal cancer in England, with and without screening at 60–69 from 2007/2009 and 60–74 from 2010/2012
In terms of number of colorectal cancer deaths prevented, the effect of screening, when considered as a percentage reduction, is rather similar. Figure 4a shows the results based on (the realistic) Scenario 1 (20% never attend and 60% of the remainder attend at each round). The percentage decrease in the number of deaths from colorectal cancer (at all ages), in the two different scenarios, is shown in Table 1. In the ‘realistic’ scenario, the number of colorectal cancer deaths is 13.3% lower than that without screening after 19 years in males and 11.7% lower in females. The cumulative savings over 19 years are 8% in men and 6.4% in women. In the more optimistic Scenario 2, savings in the numbers of colorectal cancer deaths are 16.9% and 14.9% in men and women, respectively, and the cumulative savings after 19 years are 10.2% and 8.2%.
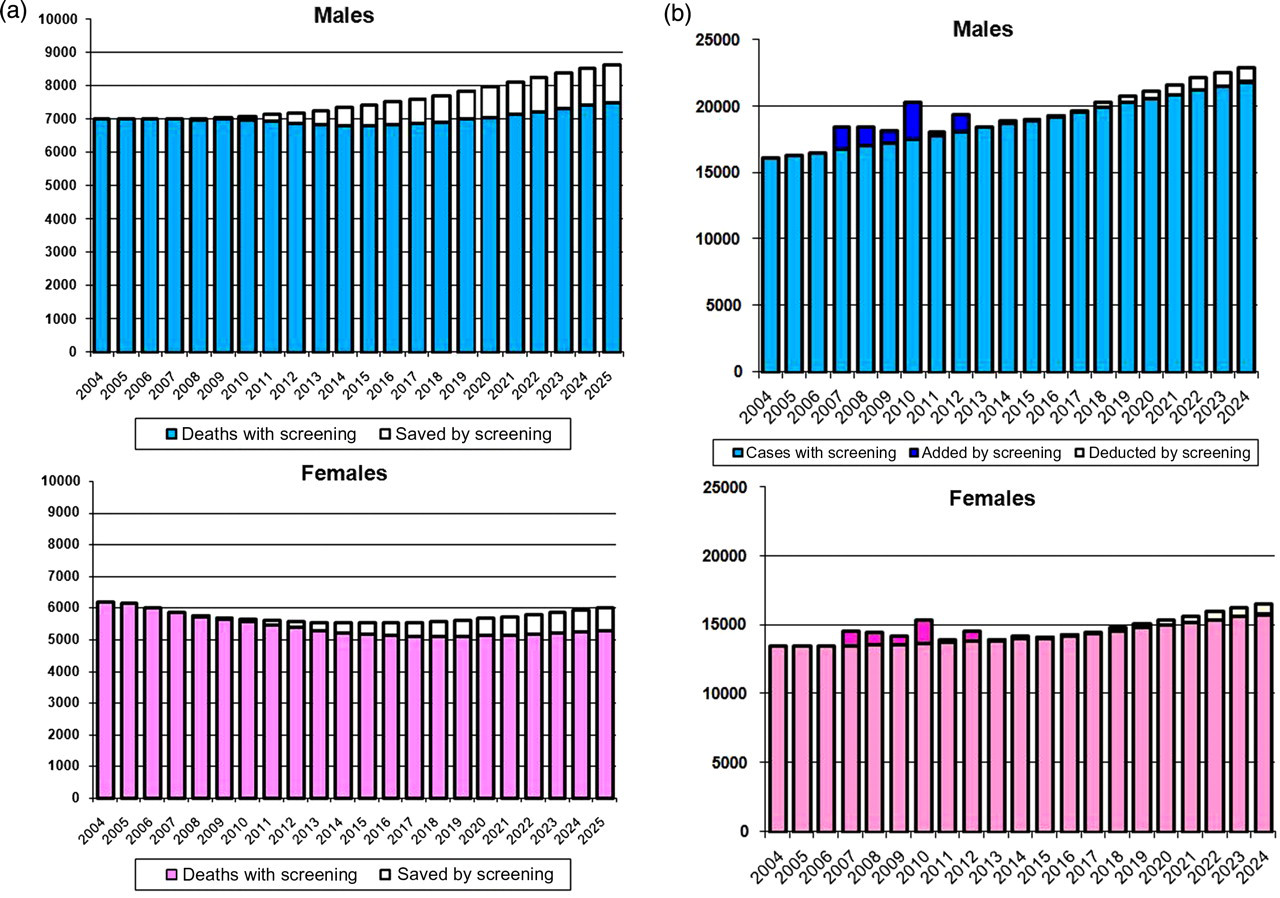
Annual numbers of (a) deaths from and (b) cases of colorectal cancer, with and without screening. Screening: 60–69 from 2007, 60–74 from 2010. 20% non-compliance, 60% attendance each round
Projected number of deaths at three periods (10, 15 and 19 years) following the introduction of screening in England, under two assumptions concerning attendance
With respect to the effects on cancer incidence, the model predicts that there will be an increase in the number of cases detected, due to screening, in the first 10 years after it is introduced. This is the result of advancing the time of diagnosis of invasive cancers by screening, so that they are detected earlier (and at a younger age) than they would otherwise have been. The incidence falls in older age groups, as many of the cancers that would have been diagnosed at these ages have been found (either as cancers or while still polyps) and treated. The model predicts that, after about 11 years, the net incidence is actually less than it would have been without screening. Figure 4b shows the predicted numbers of cases diagnosed in Scenario 1. The changes in the numbers of cases diagnosed are shown for the two scenarios in Table 2. The cumulative number of extra cases reaches a maximum of 10 years after screening is introduced, and then gradually diminishes. By 18 years after screening is introduced, the total number of additional cases that have been diagnosed is small – an additional 1% of cases in men and 0.7% in women in the ‘realistic’ Scenario 1 and 1.5% and 1.1%, respectively, in the ‘optimistic’ Scenario 2.
Projected number of new cases at four periods (5,10, 15, and 18 years) following the introduction of screening in England, under two assumptions concerning attendance
Table 3 shows the results of the sensitivity analyses for Scenario 1 (20% non-compliance and 60% attendance). With respect to the sensitivity of FOBT for polyps and cancer, we show the extremes of all possible outcomes (most and least favourable). If 90% (rather than 80%) of FOBT-positive individuals attend for colonoscopy, more incident cancers (and more polyps) are detected, and there are modest gains (of 12–13%) in mortality reductions. If screening were ineffective in detecting polyps, the number of deaths avoided 19 years after the programme is introduced would be approximately 10.3% (rather than 13.3%) in men and 8.7% (rather than 11.7%) in women. Thus, approximately a quarter of the benefit of screening on colorectal cancer mortality 19 years after its introduction comes from its ability to reduce incidence through the removal of polyps, with three-quarters coming from early detection of cancer per se.
Percentage changes in mortality and incidence after biennial screening at ages 60–69, then (after three years) at 60–74. Scenario 1: 20% non-compliers (never attend), 60% attend each round
DISCUSSION
Projections of cancer rates are essential in planning and evaluation of cancer control interventions, both in helping to set priorities for interventions and evaluating their outcomes – for example, by comparing the numbers that would have occurred in the absence of an intervention with those that actually occurred. A variety of methods have been used. 12 The NORDPRED programme, used in our study, was shown to be the best approach when projections were compared with observed future trends in a retrospective analysis of data from the Nordic countries. 9 It has been used to prepare projections of cancer incidence in England, based on registry data up to 2003. 13 The model takes into account age, period and cohort effects, and checks for departure from linearity in the observed period effect, so avoiding the projection of changes occurring in the distant past into the future, if these have, in recent years, stopped affecting the rates. The power model used in our study also dampens the potential exponential increase in rates that would be projected using the standard log-linear Poisson model. The arbitrary reduction of the ‘drift’ component of the model in each five-year period aims to simulate a progressive diminution of the effects on incidence (and mortality) of factors that are the cause of changes in risk (whatever these may be).
In order to model the effects of screening, it might appear that the results of the randomized trial carried out in Nottingham would provide the most appropriate data. However, the trial involved a limited number of subjects aged 45–74 (76,000) who were offered screening three to six times at two-year intervals (and 76,000 controls) and followed up for varying periods for up to 18 years (maximum). The results are described in Hardcastle et al. 7 and Scholefield et al. 14 and numerical data from the latter study were kindly made available by Dr Sue Moss. Among those offered screening, the proportion of subjects accepting at least one test was almost 60%. After 11 years, there was a 13% reduction in colorectal cancer mortality among those offered screening (27% for those who were screened at least once). There was very little difference in the incidence of colorectal cancer between the screened and control groups. The results seemed to be unrelated to age or sex (implying that the degree of protection is much the same throughout the life). These data cannot, however, be used to model the effect of screening on the population. This is mainly because neither is it possible to deduce the effect on mortality of one, two, three, etc. tests, nor can they be used to model how the reduction in risk persists over time following cessation of screening. In addition, the pattern of compliance with screening in the Nottingham trial is not likely to resemble what will be observed in practice as the screening programme is implemented. For example, individuals who were invited to take part in the trial and who did not accept were not initially followed up with a further invitation. In breast screening, roughly 25% of women who did not accept their first-round invitation accept at least one later invitation, and it can be assumed a similar pattern of behaviour will be present in those invited for bowel cancer screening.
Owing to these limitations, the analysis presented in this study draws on the results of a mathematical model developed to evaluate the cost-effectiveness of various bowel cancer screening programmes in England. 11 The use of such models is commonplace in addressing health-care policy questions as a means of bringing the evidence to bear on the decision problem. In particular, the use of a modelling framework allows for the consideration of all relevant comparators, the synthesis of the full range of relevant evidence, the use of an appropriate horizon and a comprehensive analysis of uncertainty surrounding the current evidence base. 15 However, as with any model-based analysis, the ScHARR screening model is underpinned by a number of assumptions regarding the natural history of colorectal cancer, the characteristics of the FOBT and the behaviour of the screen-eligible population, which may limit the validity of the analysis. Most notably, the evidence used to model the natural history of colorectal cancer is subject to considerable uncertainty and several parameters were based on model calibration rather than direct empirical evidence. Tappenden et al. 11 evaluated this uncertainty through the use of scenario analysis and probabilistic sensitivity analysis. These analyses suggested that the impact of alternative assumptions regarding natural history and test characteristics did not change the conclusions of the health economic analysis. In this paper, we examine a range of possible assumptions concerning test sensitivity and present the most extreme possible outcomes. Although this shows how far the parameter assumptions could change the results, they are very unlikely – the base-case analysis (which was based on the expectation of the calibration of uncertain natural history parameters) represents the most likely scenario.
With respect to the modelling of programmatic aspects, we have incorporated in this paper the effects of different rates of compliance and attendance. The model assumes that the percentage of persons found to be FOB-positive who are followed up by colonoscopy would be 80%. This is very close to the observed values in the UK pilot study, where it was 80.5% and 82.8% at the first (prevalent) and second (incident) screening rounds, respectively. 6
The benefits of screening seem modest when considered in terms of the percentage of the predicted number of deaths from colorectal cancer that might be avoided by a programme of biennial FOBT at ages 60–69, than at 60–74: a decrease in the expected numbers of colorectal cancer deaths of 13–16% in men and 12–14% in women (depending on the assumptions about attendance and compliance). The sensitivity of the FOBT in detecting cancer that was used in the ScHARR model producing the above results was rather modest (41%). The value was chosen based on findings from some large studies in the USA. It represents the percentage of colorectal cancers that are detected by an FOBT. In the English pilot study, 6 the sensitivity of the test at the first screening round was about 60% – but this was based upon the diminution in the number of cancers detected within two years of that test.
It is clearly important to consider the different results that would follow different patterns of compliance with screening and attendance. In fact, attendance is not likely to be random, as even among those who will comply, individuals who respond to a first call for screening are more likely to respond to further ones. The ScHARR model is not able to reproduce this effect (by making probability of attendance conditional on previous attendance). In the ‘realistic’ scenario for which results are presented, the proportion of the population undertaking a first test would be 48%, but by the second round, 67% of the population in the target age range will have participated at least once and by the third round, 75% will have had one or more tests. The UK Colorectal Screening Pilot 5 suggest that compliance with screening may be rather better than was observed in the Nottingham trial, in which 53.4% of subjects participated with the first test offered, whereas in the pilot study it was almost 60%. In the ‘optimistic’ scenario, 60% of individuals in the population would appear for a first test, by the second round, 77% of the population would have had one or more tests and by the third round, it would be 79%. Probably, performance would be somewhere between these two options, but one might hope to attain the ‘optimistic’ level. In the breast cancer screening programme, for example, 75% of women aged 55–59 have had a test within the last three years, whereas in the cervical cancer screening programme, 79% of eligible women aged 25–64 in England had been screened at least once in the previous five years and 88% in the previous 10 years. 16
The model predicted a reduction in incidence several years after the introduction of screening. This was not observed in the Nottingham trial, although the number of subjects under observation were too few to detect the lower cumulative incidence in the screened group 13 years after onset of screening, as the model predicts. In the Minnesota trial in the USA, however, a significantly reduced incidence was evident after about eight years of annual screening and 10 years of biennial screening. 17 However, in that trial, the FOBT (guiac) was read after rehydration. This increases sensitivity (and decreases specificity) to the point where most of the population had undergone colonoscopy by the end of the trial. Neither the Nottingham 7 nor Funen 18 trial used rehydration, nor does any modern programme, including the UK, either in the pilot or in the programme mode.
A further major difference would be in the acceptance pattern likely to be seen in a screening programme running over many years. While it is true to say that people who accept the first invitation are more likely to accept subsequent invitations, there are undoubtedly many people who respond erratically and others who will respond when invited in a later screening round, although they have never responded before. For example, in the Minnesota study, 17 only 50% of participants accepted every invitation, but 90% underwent at least one round of testing. In the NHS Breast Screening Programme, about 25% of women who have not accepted their previous invitation will respond when re-invited.
CONCLUSION
The decrease in mortality from colorectal cancer expected from implementing a programme such as that currently being introduced in England (13–17% in men and 12–15% in women) may seem modest in relation to the logistic complexity and resources required. However, colorectal cancer is the second most common cause of cancer death in the UK, so that the annual saving in numbers of lives is not negligible – 1800–2400 per year by 2025 in England (equivalent numbers are 2200–2700 in all over the UK). In addition, one might anticipate reduced disability, resulting from less intensive treatment with fewer long-term sequelae (such as colostomies), as non-fatal cancers will be diagnosed at earlier stages. The national programmes currently rely upon FOBT testing – the only modality whose efficacy has been demonstrated in randomized trials, but it is possible that when the results of ongoing studies (such as the use of flexible sigmoidoscopy 19 ) become available, policy may change.