
Abstract
Objectives
Routine screening for rubella susceptibility is recommended in the UK so that women found to be susceptible can be offered immunization in the post partum period. We demonstrate the use of newborn dried blood spot samples linked to routine vital statistics datasets to monitor rubella susceptibility in pregnant women and to investigate maternal characteristics as determinants of rubella seronegativity.
Setting
North Thames region of England (including large parts of inner London).
Methods
Maternally acquired rubella IgG antibody levels were measured in 18882 newborn screening blood spot samples. Latent class regression finite mixture models were used to classify samples as seronegative to rubella. Data on maternal country of birth were available through linkage to birth registration data.
Results
An estimated 2.7% (95% CI 2.4%–3.0%) of newly delivered women in North Thames were found to be seronegative. Mothers born abroad, particularly in Sub-Saharan Africa and South Asia, were more likely to be seronegative than UK-born mothers, with adjusted odds ratios of 4.2 (95% CI 3.1–5.6) and 5.0 (3.8–6.5), respectively. Mothers under 20 years were more likely to be seronegative than those aged 30 to 34.
Conclusion
Our findings highlight the need for vaccination to be targeted specifically at migrant women and their families to ensure that they are protected from rubella in pregnancy and its serious consequences.
Introduction
During the last decade the UK has experienced large-scale migration from Asia, Africa and Europe. Many countries in these regions have either no national rubella vaccination programme, or sub-optimal vaccine uptake as in parts of Southern and Eastern Europe.4,5 As a large proportion of international migrants to the UK reside in London, 6 the proportion of women susceptible to rubella infection is likely to have increased. Studies of rubella immunity during pregnancy have shown that in the UK women from minority ethnic groups are more likely to have low or undetectable rubella antibody levels than those from other groups.7–9
The uneven uptake of MMR vaccine across the UK and especially in London is cause for concern. Since 1999, MMR uptake among 24-month-old children in London has remained below 80%, 10 the minimum uptake required in the long term to prevent rubella virus circulation.11,12 In some localities within London, first-dose MMR uptake was less than 70% in 2006–2007. 10 Low uptake of MMR vaccine has already been linked to several measles outbreaks in London (see for example Atkinson et al. 13 and Ashmore et al. 14 ), and one death in England in 2006. 15 The European region of the World Health Organization has set a target for elimination of rubella and reduction of the number of congenital rubella cases to less than 1/100 000 by 2010. 16 In order to achieve and maintain this low incidence, rubella control measures, particularly MMR uptake among children in the UK and in other European countries needs to be improved.
All pregnant women in the UK are offered antenatal screening for rubella susceptibility.17,18 However, data routinely collected from the antenatal screening programme are not currently disaggregated by maternal characteristics, 19 and reliable data on maternal country of origin are not available. Furthermore, as the cut-off values used in the antenatal screening programme to indicate rubella susceptibility in pregnancy are designed to identify all women requiring vaccination, using such data may overestimate prevalence of seronegativity as it includes false positives.
Data on rubella antibody levels for women of reproductive age, disaggregated by age group, country of birth and area of residence, are required to identify groups at increased risk of infection. As maternal IgG antibodies are transferred to offspring across the placenta,21,22 newborn antibody levels can be used as a proxy for maternal antibody concentration. We carried out a seroprevalence study among newly delivered women using residual dried blood spot samples from routine newborn screening. As coverage of screening is very high, these samples provide a large and nearly unbiased sampling frame for serosurveys and eliminate the need for further sample collection, which may be costly and introduce bias. The samples used in this study were collected in the North Thames area, which includes a large part of north and central London, and is a region with low MMR uptake and a substantial non UK-born population.
Methods
All newborns in the UK are offered screening for rare disorders at five to eight days of age, using whole blood spot samples collected on filter paper cards. 23 Coverage of newborn screening is estimated to be close to 100%. 24 Newborn screening samples collected in the North Thames region of England were used in this study. After completion of routine newborn screening a further blood spot is punched from the screening cards into 96-well plates for the HIV unlinked anonymous surveillance programme. 25
For logistical reasons the sampling unit was the well plate, rather than individual samples. In order to achieve 95% confidence intervals for the prevalence of rubella susceptibility with a precision to within 2.5% of the value of the estimated prevalence among Sri Lankan pregnant women (the groups with the highest prevalence of rubella susceptibility in a previous study 9 ), around 20 000 newborn dried blood spot samples were required. A random sample of 220 plates was taken, containing 19,781 of the approximately 55,600 samples tested for HIV in the first and third quarter of 2004. Samples which were repeats, HIV-positive or those for which parents had declined screening or HIV testing were excluded before analyses (n = 899).
As part of the HIV testing protocol, dried blood spots are eluted in 170 μl PBS-Tween 20 solution. The residual eluates from HIV testing were tested for rubella IgG antibody according to the manufacturers’ instructions using a commercial enzyme-linked immunosorbent assay (ELISA; Diesse, Siena, Italy), which has been validated for use on dried blood spot samples. 26 Antibody concentrations are given as optical density (OD) ratios (i.e. the optical density of the sample, divided by a reference sample with a known antibody level of 10 IU/ml), which are adjusted for inter-plate variation.
Statistical methods
The specificity of antibody assays may be compromised in serosurveys in which alternative specimens to serum are used, and cut- off values provided by the manufacturer to identify seronegative samples may therefore not be applicable.27,28 Instead, we constructed latent class regression finite mixture models to the distribution of rubella IgG levels to estimate the proportion of seronegative samples. Similar models have been applied in analyses of data from other serosurveys to define a seronegative population.27–29 Details of these models are described in the Appendix. The samples allocated to the component with the lowest mean of the optimal mixture model were assumed to be seronegative.
In order to take account of sampling design, the standard error of the estimate of the proportion of seronegative women was adjusted using the svy functions in STATA 9.0. Maternal age and PCT of maternal residence at delivery are available from screening card data. A robust algorithm, linking screening card data and birth registration records held by the Office for National Statistics, has been established for the HIV unlinked anonymous surveillance programme25,30 to provide additional information on maternal country of birth. As maternal age was missing from 31% of samples after completion of data linkage, it was imputed using multiple imputation by chained equations with the Mice package 31 in the R software, assuming that maternal age data were missing at random. Five imputations were undertaken, creating five multiply imputed datasets.
In order to evaluate the independent effect of maternal characteristics on the odds of rubella seronegative status, defined as allocation to the component of the mixture model with the smallest mean based on posterior probabilities, logistic regression analyses were carried out, also using STATA version 9.O. 32 The logistic regression model was constructed as a mixed effects model, with plate as a random effect to take account of variation in assay conditions by plate. These analyses were undertaken separately for each of the five imputed datasets; coefficients were then combined using the mijoin and mini commands in STATA33,34
For the purpose of logistic regression analyses, maternal age was coded into age groups (<20, 20–24, 25–29, 30–34 and 35 years and over) and maternal country of birth into seven world regions (UK, other Europe, Sub-Saharan Africa, South Asia, Americas, North Africa and West and Central Asia, and East and South East Asia and Oceania). Maternal residence at delivery within the North Thames area was coded into a five category variable; North West, North Central and North East London, Essex, and Bedfordshire and Hertfordshire. The former three are urban areas, whereas the latter two mainly cover suburban and rural localities.
This study was approved by the London Multi-Centre Research Ethics Committee (MREC).
Results
Rubella antibody concentrations from 18882 newborn blood spot samples received in the screening laboratory and anonymously tested for HIV between January and March, and July to September 2004 were included in the analysis, representing around 33% of the approximately 56600 screening samples received in the screening laboratory and tested for HIV in this period. Record linkage to birth registration data was achieved for 18410 (97.5%) samples. Maternal area of residence at delivery was available for 18750 samples (99.3%). After linkage, maternal country of birth was available for 18324 mothers (97.0%), 11195 (61.1%) of whom were born in the UK. The median maternal age (interquartile range) was 30 years (25 to 34 years), before imputation and in the five multiply imputed datasets.
From the mixture model it was estimated that 509 of 18882 samples were allocated to the component with the smallest mean; thus we estimated that 2.7% of specimens in our study sample (95% confidence interval [CI] 2.4%-3.0%) were seronegative to rubella IgG antibody. Table 1 shows the proportion of seronegative samples, as defined by the latent class mixture model, by maternal characteristics and adjusted odds ratios for the odds of rubella seronegative status.
The number of seronegative samples by maternal characteristics and adjusted odds ratios by maternal country of birth, age and SHA where registered at delivery

Wald test P values
P < 0.001
p = 0.044
p = 0.009
Number & proportion seronegative by age group based on maternal age distribution before imputation (n = 12813)
Odds ratios have been combined from the five multiply imputed datasets are adjusted for each of the other covariates and random variation by plate (n = 17985)
Recently delivered mothers aged less than 20 years of age, were more likely to be seronegative to rubella than those aged 30–34. Mothers born abroad, particularly those born in Sub-Saharan Africa and South Asia, were more likely to be seronegative than those born in the UK. Women resident in North West London were also at increased risk of being seronegative, compared with the baseline area of North East London. The combined estimate of the intraclass correlation coefficient ρ was 0.05, indicating that around 95% of the variation in maternal seronegative status was due to variation in maternal characteristics, and 5% due to variation between plates.
Discussion
We used dried blood spot samples left over from newborn screening to estimate maternally-derived rubella IgG antibody level as a proxy for maternal seronegative status in the North Thames area of England, a setting of high international migration and suboptimal MMR uptake among children. An estimated 2.7% of newly delivered women in North Thames were categorized as seronegative to rubella. This definition was derived from a latent class regression mixture model. Women born abroad were more likely than UK born women to be seronegative, with those born in Sub-Saharan Africa and South Asia at highest risk. Women under 25 years, particularly those under 20 years, were significantly more likely to be seronegative than women giving birth in their early thirties. We also found that women resident in North West London were at significantly greater risk of being rubella seronegative; however there were no significant differences between the two suburban/rural regions (Essex and Bedfordshire and Hertfordshire) and the baseline area of North East London, which is highly urbanised and includes parts of central London. The increased odds of being seronegative to rubella among women born abroad can be explained by the absence of rubella vaccination programmes in their country of origin. The majority of countries in Sub-Saharan Africa and South Asia have not implemented selective or universal rubella immunization programmes, 35 and MMR vaccination has only recently been included in the national schedules in countries in Central and South America and East Asia. In some countries in Eastern and Southern Europe, although rubella vaccination has been in place, uptake has been suboptimal.36–38
Giraudon et al. 39 reported that 4% of women screened negative to rubella antibody in London through the antenatal screening programme in 2004. Our estimate is slightly lower than this. However these two prevalence estimates may not be directly comparable, as the aim of the antenatal screening programme is to identify women in need of vaccination, and hence the cut-off used to define rubella seronegative status may be higher than that used in the present study. 20 It has also been reported in previous British studies that a high proportion of children with congenital rubella have mothers of Asian background 8 , and that women who are from a minority ethnic background are more likely than white British women to be seronegative to rubella.7,9 The use of data linkage in this study allows us to estimate the prevalence of rubella susceptibility in pregnant women by country of birth thus reflecting the effect of different immunization policies.
Country of birth was used as an indicator of maternal migrant status, but the date of entry to the UK is not known for women who have migrated. It was therefore not possible to estimate the prevalence of rubella seronegative status separately for newly arrived migrants and long-term residents although it is likely that the prevalence in the former group is higher.
Residual newborn screening samples are a useful resource for monitoring maternal susceptibility to rubella in the general population. Due to the very high coverage of newborn screening, these samples provide a large and near-universal sampling frame with which to estimate maternally acquired rubella IgG antibody using relatively inexpensive methods. Although it was not possible in this study to make a direct comparison between rubella IgG levels using paired samples of maternal sera and newborn dried blood spots, a high level of agreement between maternal and newborn rubella IgG levels has been demonstrated elsewhere.22,40,41
Latent class regression finite mixture models allow estimation of the proportion of women with low antibody levels who are at increased risk of infection, but avoid using cut-off values that may be less accurate when alternative dried blood spot samples rather than serum are used. 27 The proportion of seronegative samples by maternal region of birth could be estimated as the samples were linked to birth registration data. This is the first study of rubella seroprevalence in pregnant women in which such data linkage is used, providing a more specific indicator of maternal background than those used in previous studies. It is unlikely that a study of this size with minimal bias and relevant demographic information would have been feasible without data linkage between health service and vital statistics datasets.
The main limitation of this study is the lack of data on parity, as it is not on the public record of the birth registration form in England and Wales and is not recorded for unmarried women. Parity is associated with rubella immunity in pregnancy 9 as post-partum vaccination is recommended for women who screen rubella susceptible in pregnancy. Thus women delivering their second or subsequent child would be expected to be immune if the screening programme is effective. The observed relationship between maternal age and rubella seronegative status may therefore be attributed to the antenatal screening programme, as older mothers are more likely to be giving birth to their second or subsequent child. However, this would only apply to women previously pregnant in the UK, and no reliable information is available regarding the proportion of women who take up post-partum rubella vaccination. The inclusion of parity on the public record of the birth registration form would allow future studies to explore further the influence of maternal age and parity on rubella seronegative status in pregnant women.
The aim of the current UK antenatal screening programme for rubella antibody is to identify susceptible women who require post-partum vaccination. However, post-partum vaccination only protects women who have delivered previous children in the UK, and susceptible migrant women arriving in the UK pregnant or prior to becoming pregnant will remain at increased risk of infection. As childhood vaccination uptake has been suboptimal in London for several years, outbreaks are now more likely, and spread to pregnant women is a risk, particularly if other family members are susceptible. Supplementary vaccination activities targeted particularly at newly arrived migrants and their families, preferably at their first point of contact with UK health-care services, are required to prevent a rubella outbreak spreading to susceptible pregnant women.
Footnotes
Acknowledgements
This study was funded by the Medical Research Council, grant number G0300654. This work was undertaken at the UCL Institute of Child Health which receives a proportion of funding from the Department of Health's NIHR Biomedical Research Centres funding scheme. In addition, The Centre for Paediatric Epidemiology and Biostatistics benefits from funding support from the Medical Research Council in its capacity as the MRC Centre of Epidemiology for Child Health.
Latent class regression finite mixture models
Latent class regression finite mixture models 42 were fitted to the full dataset (n = 18882) of rubella IgG antibody levels to characterise unidentified subpopulations according to their susceptibility. Before the models were fitted, natural logarithms were applied to the optical density ratio values to adjust for a right-skewed distribution.
The mixture models fitted were:
where y denotes log antibody levels and π k . is the weight of the k-th component in the mixture. Normal distributions were assumed for the mixture model components. The models were fitted using the flexmix library 43 in the R software. 44 The Bayesian Information Criterion (BIC) was used as the basis of the model selection strategy to determine the number of components in the optimal mixture model.
Models were fitted assuming up to five components. The optimal mixture model, based on minimization of the BIC, had four components, as shown in Table 2.
Figure 1 shows the densities of the four components of the optimal model, the total density of the rubella IgG levels in the 18882 samples, and the means (μ) and component weights (π) for the four components.
The density of the components of the optimal mixture model, with their means and weights, and the total density function of rubella IgG antibody levels (expressed as natural logarithms of the optical density ratios). Total n = 18882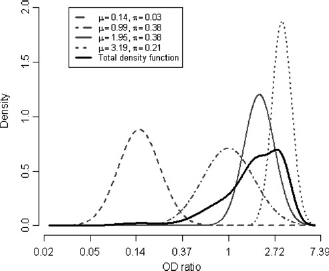
By using the Flexmix library to construct the mixture models, it is possible to calculate the probability of belonging to each component for every observation, known as posterior probabilities. The posterior probabilities can be estimated as follows: the probability that observation j is allocated to component i is given by:
We used equation (3) to assign each observation to the mixture model component for which the posterior probability was maximized. The individuals with observations assigned to the component with the smallest mean were assumed to be seronegative.