
Abstract
Objectives
To estimate the interval cancer incidence, its determinants and the episode sensitivity in the Norrbotten Mammography Screening Programme (NMSP).
Setting
Since 1989, women aged 40–74 years (n = 55,000) have been invited to biennial screening by the NMSP, Norrbotten county, Sweden.
Methods
Data on 1047 invasive breast cancers from six screening rounds of the NMSP (1989–2002) were collected. We estimated the invasive interval cancer rates, rate ratios and the episode sensitivity using the detection and incidence methods. A linear Poisson-model was used to analyse association between interval cancer incidence and sensitivity.
Results
768 screen-detected and 279 interval cancer cases were identified. The rate ratio of interval cancer decreased with age. The 50–59 year age group showed the highest rate ratio (RR = 0.52, 95% CI 0.41–0.65) and the 70–74 year age group the lowest (RR = 0.23, 95% CI 0.15–0.36). The rate ratios for the early (0–12 months) and late (13–24 months) interval cancers were similar (RR = 0.18, 95% CI 0.15–0.22 and 0.20, 95% CI 0.17–0.24). There was a significantly lower interval cancer incidence in the prevalence round as compared with the incidence rounds. According to the detection method the episode sensitivity increased with age from 57% in the age group 40–49 years to 84% in the age group 70–74 years. The corresponding figures for the incidence method were 50% and 77%, respectively.
Conclusion
Our study showed an interval cancer incidence of 38% and the episode sensitivity of 62–73%, depending on the method of calculation. Our results are of clinically acceptable level and concert with the reference values of the European guidelines.
Introduction
Estimation of the interval cancer incidence in a screening programme requires a routine for identification, collection and assessment of interval cancer cases. Reviews of the interval cancer incidence in randomized controlled trials and population-based screening programmes have been performed,2–6 as well as reviews on pooled data at regional, national and international level.7–12 However, a standardized and systematic epidemiological and radiological surveillance of interval cancers would be preferable for within-programme and between-programme comparisons and for quality control purposes. 13
Three entities of sensitivity in cancer screening have been defined: test, episode and programme sensitivity. 14 Test sensitivity is the test's ability to find a cancer in its detectable asymptomatic phase. Episode sensitivity applies to screening participants alone and indicates the ability of the full diagnostic process (the test and its histological confirmation) to detect cancer. Programme sensitivity indicates the proportion of cases identified by the screening programme in the total target population. Programme sensitivity depends not only on the sensitivity of the screening process but also on the coverage and compliance of the target population. All three concepts of sensitivity serve different purposes and are needed to describe the ability of the intervention to identify the disease in its detectable asymptomatic phase. Several studies indicate that sensitivity increases with age at invitation, recall rate and decreases with length of the screening interval.9,15,16
The objective of this study was to estimate the interval cancer incidence and its determinants and to estimate the episode sensitivity by the detection and incidence methods in the Norrbotten Mammography Screening Programme (NMSP). The definitions of terms used in this study are provided in Table 1.
Definitions of terms used in study
Methods
Setting
Norrbotten is the northernmost county of Sweden with an area of about 100,000 km2, a population density of 2.5 inhabitants/km2, a female population of 125,000 and an age standardized breast cancer incidence of 111.7/105 for the period 1995–2004. The target population consists of 55,000 women aged 40–74 years and accounts for 80% of the incident breast cancer cases in the county. The NMSP started in March 1989 and reached county-wide coverage by December 1991. Biennial screening is offered to women aged 40–74 years. The target population is served by three screening units, two mobile and one stationary. Early recall policy, that is six-month check-up instead of immediate assessment in case of equivocal screening findings, is not practiced. All breast diagnostics is delivered within the Swedish national health-care system and concentrated to the breast assessment centre at Sunderby Hospital in Luleå municipality. There is no opportunistic screening in the study area. The NMSP uses a dedicated computer programme to run screening. Screening data on individual level are regularly transferred to the Regional Oncologic Centre (ROC) in the municipality of Umeå that manages the database for Norrbotten County. The screening database is linked to the regional tumour register to get information on newly diagnosed breast cancers and to identify interval cancers. Further description of the programme can be found elsewhere. 17
The current study is approved by the Ethics Committee of Umeå University.
Statistical Analysis
The following outcome measures were calculated by age and screening round: the rate of screen-detected cancers, the rate of interval cancers (early and late), the rate ratio of interval cancers and the episode sensitivity. Overall and age-specific interval cancer rates (IR) per 10,000 screened were estimated using the number of interval cancers (IC) and the number of women screened (SCR) during the same period (IR = IC/SCR × 10,000). Early (0–12 months) and late (>12 months) interval cancer rates were estimated by screening round. The age-specific incidence trends of invasive breast cancer in Norrbotten county for the 19-year (1970–88) period preceding the start of the programme were estimated in a log-linear Poisson model. The intercept varied by age group but not the slope. Based on these estimates the background age-specific incidence rates could be predicted for the study period (1989–2002) and the expected number of breast cancer cases in screened women for a certain year could be calculated. The proportionate incidence or rate ratio (RR) of interval cancer was estimated as RR = IC/1.75E using matched age and calendar year for the expected annual number of breast cancer (E) and assuming the interval length to be 21 months (1.75 years). The 95% CI was approximated with
Results
The mean interval length was 21 months and it increased from 20.3 months in round one to 22.8 months in round six. The mean attendance rate was 82% (range 80–86%) and the mean recall rate was 2.0% (2.2, 1.3, 1.7, 2.2, 1.8 and 2.5 during round one to six, respectively). During the study period 1159 breast cancer cases, 1047 invasive and 112 in situ cases were identified. Screen-detected invasive cancers accounted for 73% (n = 768) and invasive interval cancers for 27% (n = 279). Out of 279 invasive interval cancers 47% (n = 132) presented during the first twelve months and 53% (n = 147) thereafter. Median time since the index screen was 14 months.
There was a good agreement between the observed and predicted age-specific breast cancer incidence during the screening period for all age groups except for the age group 50–59, where the observed incidence 1989–2002 increased more than the predicted curve based on the data from 1970–1988 (Figure 1).
Observed (obs) and predicted (pred) breast cancer incidence (inc) for women 40–49, 50–59, 60–69 and 70–74 years of age in Norrbotten County 1970–2002. The predicted breast cancer incidence 1990–2002 is based on the observed breast cancer incidence 1970–1988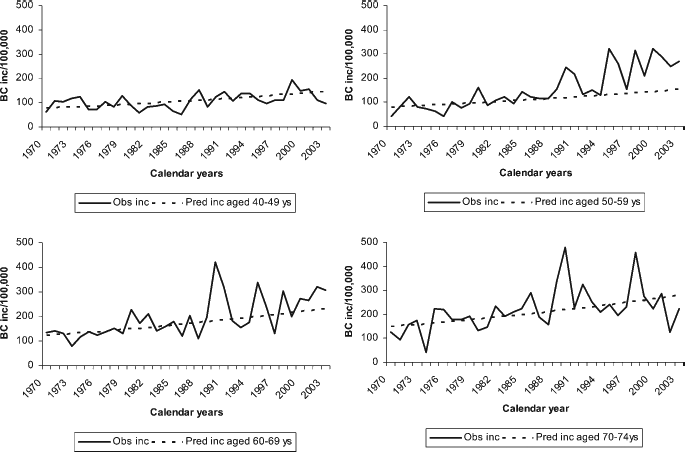
The overall screen-detected cancer rate was 29 per 10,000 screened, increasing from 14/10,000 for the age group 40–49 to 51/10,000 for the age group 70–74 years. The overall interval cancer rate was 11 per 10,000 screened. The overall interval cancer rate ratio was 0.38 (95% CI 0.34–0.44) decreasing from 0.50 (95% CI 0.40–0.62) in ages 40–49 and 0.52 (95% CI 0.41–0.65) in ages 50–59 to 0.27 (95% CI 0.20–0.35) in ages 60–69 and 0.23 (95% CI 0.15–0.36) in ages 70–74 years (Table 2).
Population size, number of screened women, screen-detected cancers (SDC) and interval cancers (IC), incidence rate/10,000 for SDC, IC, and predicted breast cancer (BC) based on the trend 1970–1988, rate ratio (RR) for IC and 95% confidence intervals (CI), sensitivity and 95% CI according to the detection and incidence methods in women 40–74 years in the Norrbotten Mammography Screening Programme (NMSP)
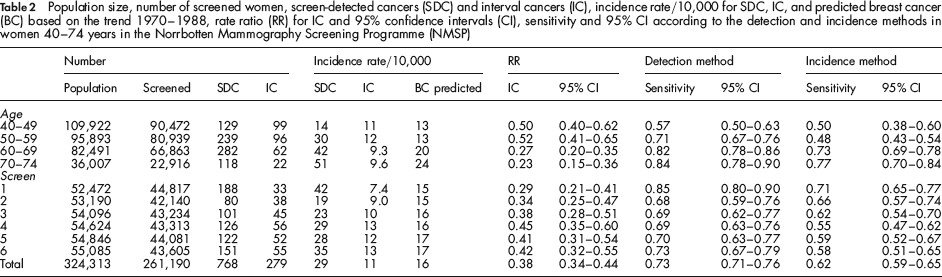
Screen-detected and interval cancer rates by age and screening round are shown in Table 2 and Figure 2. Screen-detected cancer rates increased while interval cancer rates remained constant across age. The screen-detected and interval cancer incidence rates increased with incidence rounds. The early (0–12 months) and late (>12 months) interval cancer rate ratios were 0.18 (95% CI 0.15–0.22) and 0.20 (95% CI 0.17–0.24) and varied by age and screening round (Figure 3). The RR for early interval cancers was lower in the 60–69 year age group compared with the 40–59 year age group, indicating a lower sensitivity of mammography in the younger age group. The RR for late interval cancers was directly proportional to the length of the screening interval. Overall episode sensitivity was 0.73 (95% CI 0.71–0.76) and 0.62 (95% CI 0.59–0.65) according to the detection and the incidence methods, respectively. Episode sensitivity varied by age at invitation to screening and by screening round (Table 2). The Poisson regression analysis showed that the likelihood for a tumour to be diagnosed at screening increased by increasing age and recall rate and it was higher in the first round compared with subsequent rounds (Table 3). The relative risk of interval cancer was significantly higher in the incidence rounds (relative risk = 1.6; 95% CI 1.1–2.4) due to an elevated risk of the late interval cancers by 2.3.
Incidence rate (IR)/10,000 of screen-detected cancers (SDC) and interval cancers (IC) by age (left) and screening round (right) in women aged 40–74 years in the Norrbotten Mammography Screening Programme (NMSP) Rate ratios (RR) of early (0–12 months) and late (13–24 months) interval cancers (IC) by age (left) and screen number (right) in women aged 40–74 years in the Norrbotten Mammography Screening Programme (NMSP)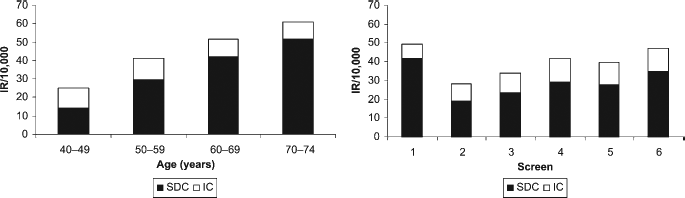

Relative risk and 95% confidence intervals (CI) for screen-detected cancers, early (0–12 months) and late (13–24 months) interval cancers in women 40–74 years in the Norrbotten Mammography Screening Programme (NMSP)

Discussion
In the NMSP the overall interval cancer rate was 11/10,000, constant by age, but increased from the prevalence screen to round four due to an increase of the late (13–24 months) interval cancers. The overall interval cancer rate ratio was 38% (early 18% and late 20%). The interval cancer rate ratio was 51% for women aged 40–59 years and 25% for women aged 60–74 years. Screen-detected cancer rates increased with age and recall rate. Episode sensitivity was 62–73% depending on the method applied and increased with age.
Only the late interval cancer rates were associated with screening round and thereby with length of the screening interval. The interval cancer rate ratio was inversely related to age. The interval cancer rate ratio in the 40–59 year age group was twice as high as in the 60–74 year age group. Sensitivity calculated by the incidence method is by definition 1 minus the interval cancer rate ratio. Both estimates are based on the predicted cancer incidence; thus their accuracy generally decreases by increasing follow-up time.
We had access to high quality incidence data from the Cancer Registry for a long period (1970–1988), which minimizes the random variation of the predicted curve and thereby also of our estimates. The detection method takes into account only cases from the screening programme; thus it is sensitive for both lead-time and overdiagnosis. Lead-time bias is mainly a problem during prevalence screen, i.e. in the first screening round and for women 40–42 years at invitation. In our study, sensitivity by the detection method was higher in the first round (0.85) compared with subsequent rounds (0.68–0.73) (Table 2). Such a clear pattern cannot be seen by the incidence method. For both methods the sensitivity increased by age; however, for the incidence method the estimate for ages 50–59 was low (0.48) due to the discrepancy between the observed and predicted incidences (Figure 1). We consider the detection method as more accurate for the estimation of episode sensitivity in our study because of the long follow-up period (1989–2002).
The European guidelines recommend that the acceptable and desirable levels of proportionate incidences of early and late interval cancer for women 50–69 years should be 30% and <30% and 50% and <50, respectively. 1 These estimates are calculated per year and not per screening round. To be able to compare our estimates, which are calculated per screening round, with the EU-guidelines we adjusted the denominator in our estimates to 1.0 and 0.75 times the number of invited women for early and late interval cancers, respectively. Our adjusted estimates of 33% and 47% for the early and late interval cancer rate ratio are in line with the acceptable level in the EU-guidelines.
Interval cancer proportionate incidence is the measure of choice for between-programme comparisons because it enables discarding geographical differences in breast cancer incidence. 18 However, programmes might differ from each other in inclusion criteria, coverage, compliance, age range, interval length, recall rate and underlying breast cancer incidence. International comparisons of interval cancers are important but should be made with caution because of the lack of standardized surveillance methods. 13 We could only locate two meta-analyses of interval cancers.16,19 A reason for that could be the lack of standardized methods and proper data. Taylor and co-workers’ meta-analysis of interval cancer incidence in randomized controlled trials and service screening programmes for women aged 40–49 showed that the proportionate incidences of the first-, and second-year interval cancers were 42% and 63% in the randomized controlled trials and 44% and 72% in the service screening programmes. 16 However, the studies included were, except for the New South Wales (NSW)-study (606 out of 1305 cases), small and followed-up for only two years which makes the interpretation difficult. Anyhow, our adjusted figures for the ages 40–49 were considerably lower than the corresponding figures for NSW (48% vs. 56% for early and 54% vs. 86% for late interval cancer). This difference can be due to the fact that women aged 40–49 were not actively recruited in the New South Wales (NSW)-programme, but they were screened on request (opportunistic screening). There was a striking similarity of the interval cancer rates by age between our programme and the NSW-programme (10.5, 11.1, 9.4 and 8.6 per 10,000 for the 40–49, 50–59, 60–69 and 70–79 year age groups). Taylor and co-workers’ comparisons of the first-year interval cancer proportionate incidences for women aged 50–69 years of the NSW data with the meta-analysis of randomized trials and service screening programmes combined gave 31% and 25%, respectively. 19 Our adjusted estimate of the first-year interval cancer proportionate incidence for the ages 50–69 was 26%. The estimates for aged 50–59 and 60–69 years were 33% and 28% in the NSW programme and 43% and 14% in the NMSP.
Within Scandinavia, both the Norwegian Breast Cancer Screening Programme (NBCSP) and the Finnish Mammography Programme (FMP) are comparable with ours. The NBCSP invites women aged 50–69 to biennial screening. With a participation rate of 79% and a recall rate of 3.6% the NBCSP achieved an episode sensitivity of 75% by the detection method. 20 Their invasive interval cancer rate was 18/10,000 and the overall interval cancer proportionate incidence was 49%. 11 The corresponding figures for NMSP for women aged 50–69 were 77%, 11/10,000 and 37%, respectively. In the FMP the design, participation rates and recall rates vary among the ten screening centres. 15 The FMP invites women aged 50–59 (90% coverage) and partly 60–64 (40% coverage) to biennial screening. The episode sensitivity in subsequent screens for women 50–64 years was estimated at 65% and 54% by the detection and incidence methods, results that are similar to our estimates for women aged 50–59 years for six screening rounds (71% and 48%). However, the overall interval cancer rate and the proportionate incidence for women 50–59 years were lower in the FMP than in our program (9/10,000 vs. 12/10,000 and 35% vs. 52%, respectively). Our study confirms the findings in earlier studies of an increasing sensitivity and a decreasing interval cancer proportionate incidence by increasing age. However, the women aged 40–49 constitute an important group from the screening perspective as they account for 35% of screened women and 20% of diagnosed cancers in Norrbotten county and the cure of one cancer case allows for many years of life gain.
The strengths of this study are the completeness and accuracy of interval cancer data, the wide age range and the long study period. The completeness of the Swedish cancer registry has been estimated at 99%. 21 To the best of our knowledge our study has the longest follow-up encompassing six screening rounds, i.e. 14 years. The wide age range facilitates comparison by age. The high attendance rate in the population-based screening programme strengthens the representativity of the results. The overall variation of recall rate and interval length in the NMSP is low and therefore the possibility to study their effect on interval cancer incidence is limited.
Our study showed that during the six rounds of the NMSP (1989–2002) the overall interval cancer incidence was 38% and the episode sensitivity was 62–73% depending on the method of calculation. The interval cancer incidence and episode sensitivity of the NMSP show a clinically acceptable level and are in concert with the reference values of the European guidelines.
Statement of Contributorship
All authors contributed to the design, writing and editing of this report. Bordás and Jonsson contributed to data collection. Jonsson was responsible for the statistical calculations.
Footnotes
Acknowledgements
This work was supported by The Lions Cancer Research Foundation, Umeå University and The Norrbotten County Council Research Foundation. The authors are grateful to the workers of the NMSP in Norrbotten county without whose work and cooperation it would not have been possible to carry out this study. The authors thank Mrs Gunilla Andersson for the clerical validation of interval breast cancer cases.