
Abstract

Acute myocarditis is a complication of influenza A H1N1 infection and signs of cardiac dysfunction in a patient diagnosed or suspected to have the infection should alert the clinician to myocarditis and its complications.
Case Report
A forty-six year old man presented to the Emergency Department with sudden onset chest pain and palpitations following flu like symptoms for three days. His previous medical history included diabetes mellitus, epilepsy and paroxysmal atrial fibrillation. He had undergone two elective DC cardioversions for Atrial Fibrillation (AF) and coronary angiography two years ago at another hospital which had demonstrated unobstructed coronary arteries and preserved left ventricular systolic function. His admission medications included warfarin for stroke prevention.
On admission he was noted to have a heart rate over 200/minute, blood pressure 110/70mm of Hg, temperature 39.2°C and 97% oxygen saturation on room air. There were no clinical signs of heart failure. Electrocardiogram (ECG) revealed regular broad complex tachycardia with right bundle branch block morphology and a ventricular rate greater than 250/minute (Figure 1). His bedside blood glucose was 9.9mMol/L.

ECG on admission showing ventricular tachycardia
As the patient was relatively well with a stable blood pressure the emergency physician initially diagnosed the rhythm to be of supra-ventricular origin (SVT with aberrancy). Adenosine was administered intravenously in an attempt to terminate the tachycardia in incremental doses of 6 mg and 12 mg without effect. The rhythm was then correctly diagnosed as ventricular tachycardia (VT). The patient continued to experience chest pain and was cardioverted using a single 50J synchronized DC shock. ECG post cardioversion revealed AF with ventricular rate of 125bpm (Figure 2). The corrected QT interval (QTc) was normal and there were no epsilon waves. The patient had presented to the hospital during the pandemic wave of H1N1 influenza A (swine flu) when several cases were being identified in the community. Given his prodrome of viral symptoms, myalgia, malaise and fever, he met the criteria for clinical diagnosis of H1N1 influenza A virus infection. Antiviral therapy in the form of Oseltamivir was started empirically and he was admitted to hospital for monitoring and supportive care. Nasal swabs taken from the patient later confirmed the diagnosis of influenza A H1N1 infection. Cardiac Troponin on admission was elevated at 0.04 microgram/litre (normal <0.02).
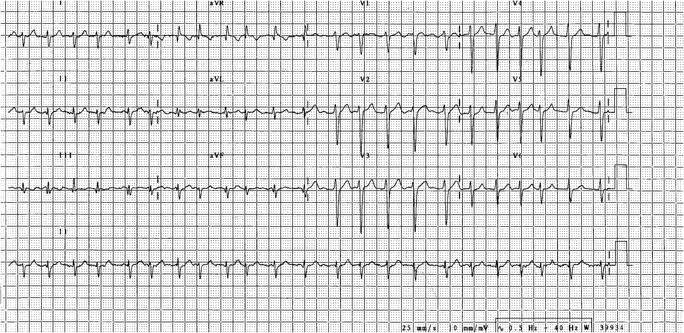
ECG after DC cardioversion showing atrial fibrillation
Other relevant blood results included Sodium 140 mmol/L, Potassium 5.1 mmol/L, Urea 7.9 mmol/L, Creatinine 77 micromol/L, Magnesium 0.85 mmol/L and CRP 19 mg/L. Oseltamivir was continued for ten days during which he remained free of further symptoms and arrhythmias. He made a good recovery and coronary angiography was performed which once again confirmed normal coronary arteries. Left ventriculography and trans-thoracic echocardiography demonstrated mildly impaired left ventricular function with global hypokinesia. Cardiac magnetic resonance scan was considered, but this would have required transferring the patient who was being nursed in isolation to another centre and would not have impacted the management and was therefore not pursued. A programmed VT stimulation test was performed as per Wellen's protocol. 1 Sustained monomorphic ventricular tachycardia could not be initiated and the test was negative. A diagnosis of monomorphic VT secondary to active myocarditis caused by influenza A-H1N1 was made retrospectively. He remained in AF and warfarin was continued indefinitely on discharge. He has remained well to date.
Discussion
Myocarditis is an inflammatory disease of the myocardium caused by a variety of etiological factors of which viruses are commonly implicated in developed countries. The cardiac presentation is variable and includes a spectrum of disorders from asymptomatic ECG changes to severe disease characterized by cardiogenic shock and sudden death. 2,3 A viral prodrome of fever, myalgia and muscle tenderness often precede viral myocarditis. 3 Myocardial biopsy and histology remains the gold standard for diagnosis. But often a presumptive diagnosis of myocarditis is made based on the clinical scenario and supportive evidence from imaging modalities such as echocardiogram and magnetic resonance. The histology may show varying degrees of mononuclear cellular infiltrates often associated with myocyte necrosis and disorganization of the cytoskeleton. 3 Treatment of myocarditis includes specific therapy aimed at the cause and nonspecific therapy aimed at clinical manifestations such as heart failure and arrhythmias. The prognosis of myocarditis depends on the cause and severity of the disease. Unsurprisingly, patients who present with the disease in the more severe end of the spectrum have a higher risk of death and complications in the short term, but once recovered from the acute phase their long term prognosis tends to be better than those with less severe forms of the disease. 4
The true incidence of viral myocarditis and specifically those caused by influenza virus strains remains unknown. Although previously it was thought that myocardial inflammation occurs in up to 10% of patients with acute influenza, Greaves et al. in their study used cardiac troponin as marker of myocardial injury in influenza infected patients and concluded that the incidence is considerably lower. 5 There have been a few case reports of H1N1 virus causing myocarditis in adults 6–8 and a case series of fulminant myocarditis in children. 9 In a review of 838 children admitted to paediatric intensive care unit with H1N1 infection, the prevalence of myocarditis was noted to be 1.4%. 10 H1N1 influenza associated myocarditis appears to present with more severe disease, with most reporting fulminant myocarditis and acute heart failure. Our patient presented with a life threatening arrhythmia although he was not in cardiogenic shock. To our knowledge there has not been any similar cases reported.
This case illustrates the dramatic presentation of H1N1 flu in a previously asymptomatic adult. Treatment of the life threatening arrhythmia followed by antiviral therapy and supportive care led to a good outcome in this case. More cases of H1N1 flu are expected in the coming years as the virus is expected to circulate as a seasonal flu virus. In patients suspected of having influenza the clinician needs to be alert to signs of myocarditis and consider appropriate supportive care and anti-viral therapy. Broad complex tachycardia in such patients is likely to represent VT and needs to be treated without delay. In H1N1 influenza, associated myocarditis there should be a low threshold for escalation of care to intensive therapy unit and use of ventilatory/circulatory support as the long term prognosis is often very good once the acute phase of the illness is over.
DECLARATIONS
Competing Interests
None declared
Funding
No funding was received in relation to the case report
Ethical Approval
Written informed consent to publish was obtained from the patient or next of kin.
Guarantor
James Barry
Contributorship
All three authors were closely involved in the conception of the case report and in its editing.
Acknowledgements
None