
Abstract
Summary
Telemedicine services must be designed and implemented with the users in mind. When conducting telerehabilitation, factors such as age, education and technology experience must be taken into account. In addition, telerehabilitation must also accommodate a range of potential patient impairments, including deficits in language, cognition, motor function, vision and voice. Telerehabilitation technology and treatment environments should adhere to universal design standards so as to be accessible, efficient, usable and understandable to all. This will result in improved access to a wider range of telerehabilitation services that will facilitate and enhance the rehabilitative treatment and recovery of people living with varying levels of injury, impairment and disability.
Introduction
Telemedicine services usually involve a patient, a clinician, some form of medical information and a method of data transmission. While the details (e.g. the diagnosis of the patient, the specialty of the clinician[s], the content and format of the medical information, and how and when the information is transmitted) will vary depending on the application, there are high-level goals such as patient satisfaction, security of medical information, device usability and clinician adoption which are common to all telemedicine services.
In studying the human factors of telemedicine, it is helpful to use a macroergonomic approach. Unlike microergonomics, which considers only the users and their relationship with technology, macroergonomics is a top-down approach which considers the human–technology relationship relative to the organizational structure and external environment in which it occurs. 1 By focusing equal attention on the four subsystems (personnel, technology, organization and environment) (Figure 1), valuable insight can be obtained into how telemedicine programmes operate and how they can be optimized.
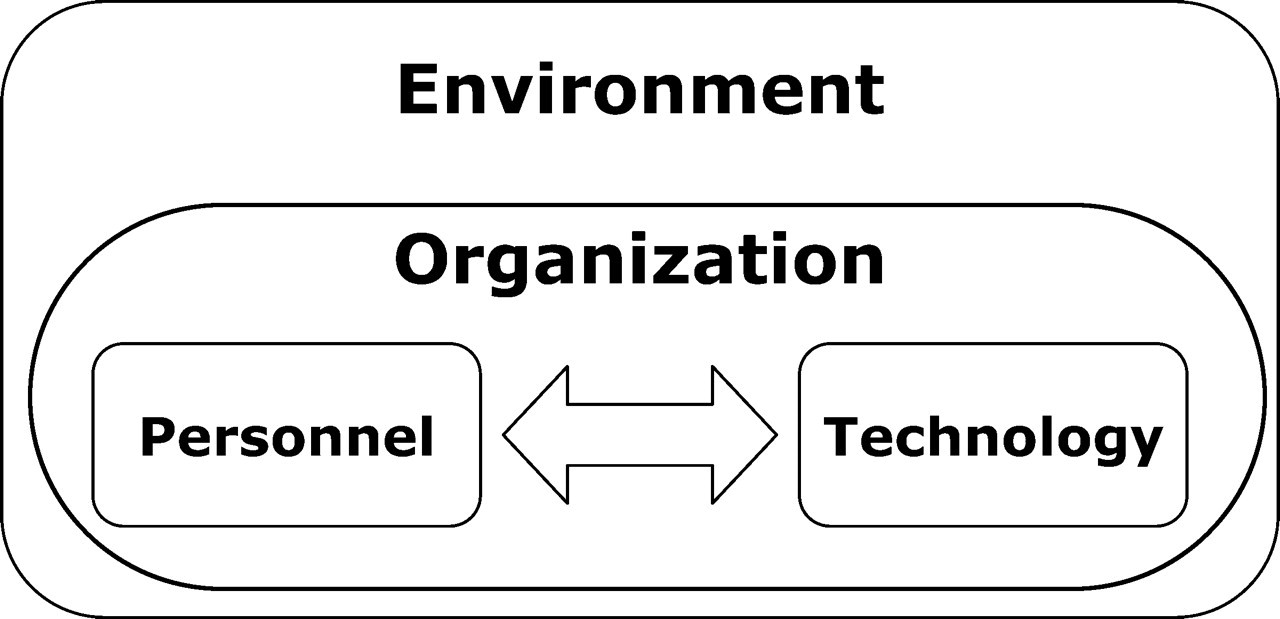
Macroergonomic model of relationships within telemedicine subsystems
An important human factor in telemedicine is the role that personnel play in all stages of planning, training and implementation. In telemedicine programmes, the definition of personnel (or ‘users’) is broad and encompasses the entire range of people involved in a telemedicine encounter, which may consist of primary care and specialist clinicians, patients, administrators and support staff such as technical support personnel and caregivers. 2 Depending on the application, the number of users during a telemedicine encounter could be as few as two (e.g. a patient at home connected to a nurse at a monitoring centre) or as many as a dozen or more (e.g. a specialist consultation linking people at multiple sites). Each user's response to telemedicine will be affected by his or her own level of technical expertise, physical capabilities and organizational cultures.
Telerehabilitation
Telerehabilitation refers to the delivery of medical rehabilitation services and the support of independent living, using telehealth technologies. 3,4 It involves clinical disciplines such as speech-language pathology, occupational and physical therapy, neuropsychology, assistive technology and cardiac and vocational rehabilitation. Telerehabilitation patients include those with stroke, brain or spinal cord injuries, amputation and orthopaedic or developmental impairments. The types of telerehabilitation interventions that can be delivered are broad and include applications such as direct patient service delivery, 5,6 specialist consultation, 7,8 remote monitoring and home telehealth, 9–11 and telerobotics. 12,13 The demand for rehabilitation services is growing as a result of the aging population and improved treatment of patients with stroke, brain injury and other disabling conditions. Because of the increasing demand, as well as the problems of clinician shortages and decreased reimbursement, rehabilitation practitioners are turning to telerehabilitation as a way of improving access, enhancing the quality of care and reducing costs.
Human factors in telerehabilitation
It is essential that all telemedicine services are designed and implemented with the users in mind. While factors such as age, education and technology experience must be taken into account when conducting telerehabilitation, consideration must also be given to patients' impairment(s). Deficits in cognitive, gross or fine motor, visual, language or voice skills all play an important role in patients' ability to use the technology and their level of acceptance and adoption of receiving services at a distance. 4 Telerehabilitation technology should maximize a patient's abilities while minimizing the effect of any abilities that may have been lost or impaired. 14 One way to accomplish this is by applying basic universal design principles, for example, providing a large button telephone, offering alternative input methods to devices (such as a touch-screen or voice recognition), or using simplified large-text or graphic-based instruction manuals and troubleshooting guides.
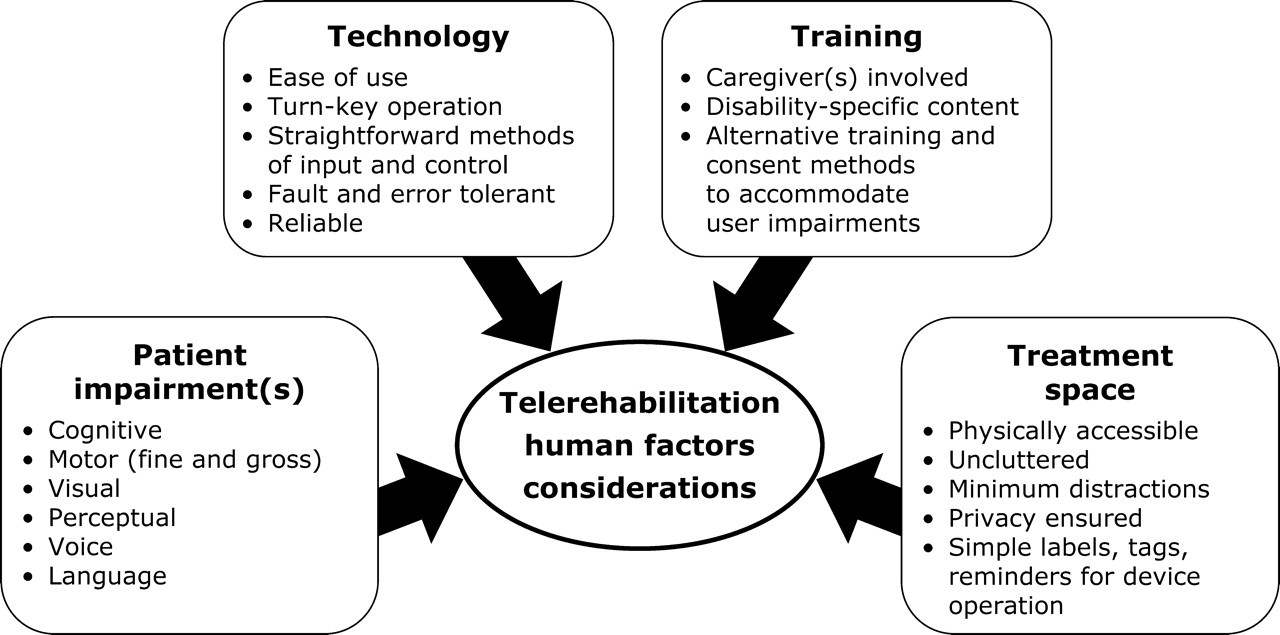
Key human factors for telerehabilitation applications
Telerehabilitation programmes must also account for the range of different clinician users who are involved in all aspects of service delivery. In addition to the consideration given to clinicians' technical knowledge, experience and training, matters such as professional licensure and professional scope of practice must also be recognized and addressed. The American Speech–Language–Hearing Association and the Canadian Association of Occupational Therapists are two professional associations which have tried to educate their members about telerehabilitation and to develop policies on the delivery of remote rehabilitation services. 15,16 It is paramount that telerehabilitation clinicians ensure that the services they intend to provide are within their professional scope of practice and that they possess the knowledge and skills required to provide them.
Other important human factors issues in telerehabilitation are the service delivery environment and the training of users. The design of a telerehabilitation space must allow patients with mobility aides such as walkers and wheelchairs to access the facility. In normal telemedicine practice, it is important to maintain an uncluttered environment and minimize distractions in the treatment space. 17 This is even more important for telerehabilitation patients who may have decreased levels of attention (e.g. following traumatic brain injury). In training telerehabilitation clinicians and support staff, attention must be paid to ensuring that everyone is familiar with disability-related matters and is comfortable about communicating with patients who may have impaired speech or language. For telerehabilitation patients, alternative educational techniques and informed consent procedures (e.g. simplified demonstration rather than course-based instruction) may be needed to ensure they are able to fully understand the procedures and the tasks that will be required of them.
Much as general medicine has seen a gradual shift towards preventative, proactive and continuous care, 18 rehabilitation has also become increasingly focused on the prevention of secondary complications. Rehabilitative care following a stroke, spinal cord or traumatic brain injury is often a lifelong process, with recovery occurring at different rates for each patient. Telerehabilitation for these patients can be approached using established techniques for disease management and care coordination. 19–21 Home health and monitoring technologies can be used to help reduce or avoid dangerous medical consequences (e.g. pressure sores in patients with spinal cord injuries) and re-hospitalizations. 22,23 While placing technology in the rehabilitation patient's home is the most direct way to improve access to care, it magnifies some of the considerations already mentioned and raises additional concerns as user roles become more dynamic and the service delivery environment becomes less controlled.
In the normal telemedicine delivery model, there are staff available at each site to assist users during the telemedicine encounter and help with the set-up and use of any equipment. However, the home environment is an unsupervised setting, with on-site assistance only available from the caregiver. Thus it is essential to provide training for caregivers who may be asked to act as an impromptu scheduler, clinician assistant, audiovisual technician or technology support person. Devices placed in the home must be simple to operate, reliable and have a high level of fault tolerance. Remote system diagnostics may be useful for troubleshooting and maintenance of the equipment at a distance. Patient privacy must always be protected, so as to comply with the relevant legal and regulatory requirements, and also to give patients confidence that they are active participants in their care, rather than being watched by ‘big brother’.
Given the broad scope of telerehabilitation, there is no single generic system that meets the needs of all applications; rather systems need to be flexible based on their entire context of use. Figure 2 summarizes and illustrates several major subsets of human factors considerations that should be used to guide planning and delivery of telerehabilitation applications. For example, in using a computer-based telerehabilitation system to deliver speech-language treatment to a stroke survivor, impairments in language, cognition and motor function necessitate a simple user interface (e.g. with large on-screen buttons and limited distractions such as toolbars and menus), an easy way to interact with the system (e.g. a touchscreen computer monitor) and an environment that does not distract the patient or detract from the ability of the clinician to deliver treatment.
Conclusion
Human factors and technology usability play significant roles in the utilization, acceptance and economic viability of telemedicine programmes generally. 2,14,24,25 Thus it is essential that theories of human factors and user centred design be applied to the planning and implementation of new programmes and the design of new devices. 26 This is supported by recent telemedicine practice standards and technical guidelines that incorporate human factors considerations. 27
Human factors principles are also central to the growth of telerehabilitation. With a diverse group of clinicians and patients, it is essential that all aspects of telerehabilitation service delivery be accessible, efficient, understandable and usable by all people regardless of their age, background or abilities. This will result in improved access to a wider range of telerehabilitation services that will facilitate and enhance the rehabilitative treatment and recovery of people living with varying levels of injury, impairment and disability.