
Abstract
Summary
A total of 140 obese patients (mean age 14 years) participated in a structured treatment and teaching programme (STTP) in hospital, with the aim of weight reduction. At both the start and finish of the STTP, patients underwent clinical and psychological examination. During an average hospital stay of 35 days, their mean bodyweight decreased from 82.4 kg to 76.0 kg (P < 0.001). Patients were then followed up with a telemedicine support programme. During the next 12 months, the acceptance of the telemedicine support programme declined from 93% to 46%. The body mass index was 30.5 kg/m2 at admission and 27.7 kg/m2 at 12-month follow-up (P < 0.05). In parallel, wellbeing and treatment satisfaction increased, and there was a positive effect on eating behaviour and exercise. Intervention was needed in up to 64% of the children and adolescents who participated in the programme, most frequently due to poor results in exercise. Telemedical follow-up care and counselling seemed to be highly effective, and allowed not only an initial weight reduction, but long-term stabilization as well.
Introduction
The prevalence of overweight and obesity has increased markedly in the last few decades in most Western European countries and the US. 1–4 The association between obesity and the risk for development of cardiovascular diseases has also been recognized. 5 Studies have demonstrated the efficacy of lifestyle and behaviour modification in the short term, primarily for periods of up to six months. 6–8 One potential means of improving long-term outcomes is outpatient-based programmes with consequent ambulatory control 9 or telemedicine support strategies. For example, Williamson et al. demonstrated in overweight adolescent African American girls a clear benefit from an Internet-based behavioural intervention. 10
We have developed a telemedicine support programme, TeleObe, with the aim of producing an initial reduction of body weight and long-term stabilization.
Methods
The study was conducted in two phases.
Phase one
In the first six months of 2005, a total of 140 children and adolescents hospitalized for weight reduction were consecutively recruited from the Department of Diabetes and Metabolic Diseases, Inselklinik Heringsdorf GmbH, Seeheilbad Heringsdorf. Ethics permission was not required. The characteristics of the patients are shown in Table 1. During hospitalization, over a period of 4–6 weeks the subjects participated in a structured treatment and teaching programme (STTP). The STTP was designed according to the published guidelines. 11 The learning programme consisted of 49 sessions and offered instruction by physicians, psychologists and educators specializing in nutrition and exercise. Theoretical learning was combined with outdoor activities like mountain-biking, sailing, walking, jogging, swimming, football, basketball and beach volleyball. In addition, there was a special programme lasting three days designed for the parents of the children.
Baseline characteristics of the 140 children and adolescents enrolled in the study
At the start and finish of the STTP, patients underwent clinical and psychological examination. Body mass index (BMI) and BMI-SDS (a BMI standard deviation score 11 ) were calculated. A psychological examination was conducted using standardized questionnaires to assess wellbeing and treatment satisfaction (WHO-5), depression 12 and motivation.
Phase two
After discharge, patients were followed up by the telemedicine support programme. The programme integrated standardized data assessment, data collection, visualization and recommendations for further treatment by using Internet services and/or a mobile phone. Its core was a module which summarized the patients' clinical and psychological data, changes in BMI, BMI-SDS and/or psychological variables. Feedback by the physician was given to patients periodically.
The telemedicine support programme was highly interactive. Periodically (after 4 weeks, 3, 6, 9 and 12 months) patients received reminders by email and/or mobile phone. They were advised to complete standardized questionnaires about bodyweight, lifestyle, eating behaviour, exercise and psychology. The results were analysed automatically to identify trends and potential problems. Based on this information, a physician specifically trained in the treatment of overweight and obesity in children and adolescents determined whether intervention was required. Criteria for a negative tendency, and thus the need for intervention, were scores in at least one domain below the lowest tertile. Intervention could also be started at the patient's request. After a decision to intervene, a strategy was designed and begun. This intervention consisted of either Internet and/or counselling by telephone performed by a physician, a psychologist or an educator in nutrition or exercise. In some cases, complex interventions involved physicians, psychologists and/or educators specialized in exercise and nutrition. Either an intervention was performed once at the follow-up examinations (3, 6, 9 and 12 months after STTP, if the problem disappeared afterwards) or very frequently (each day or up to every second day).
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS 13.0).
Results
Phase one
Children and adolescents were hospitalized for an average of 35 days (SD 5). During this period they participated in the STTP. Their mean bodyweight decreased to 76.0 kg (SD 18.9) (P < 0.001). Their mean BMI decreased to 27.9 kg/m2 (SD 5.0) (P < 0.001) and BMI-SDS decreased to 2.11 (SD 0.62) (P < 0.001).
For those children and adolescents (n = 30) who participated in the STTP for only four weeks (due to restrictions of the National Health Care Insurance), the mean weight reduction was less (6.5 kg, SD 2.4) than in the other patients who completed six weeks (n = 110) (7.5 kg, SD 3.0). This difference was significant (P = 0.035).
There were significant correlations between BMI at onset and BMI at the time of hospital discharge (r = 0.98, P < 0.001), BMI-SDS at onset and BMI-SDS at hospital discharge (r = 0.98, P < 0.001), patients' age and BMI at onset (r = 0.43, P < 0.001), patients' age and BMI at hospital discharge (r = 0.46, P < 0.001), and the BMI-SDS at onset (r = 0.45, P < 0.001) and BMI-SDS at hospital discharge (r = 0.48, P < 0.001). There was also a correlation between the duration of the participation in the STTP and weight reduction (r = 0.25, P < 0.001).
Phase two
The acceptance of the telemedicine support programme was 93% six months after the onset of the trial and 46% after 12 months. There was a significant decrease in acceptance between month 9 and month 12 (P = 0.043). However, in the patients who participated in the telemedicine support programme (i.e. analysis to treat), there was a stabilization of both BMI (Figure 1) and BMI-SDS after discharge (Figure 2). At 12 months, all the variables were significantly lower than at the beginning of the trial (body weight: P = 0.010, BMI: P < 0.001, BMI-SDS: P = 0.001).
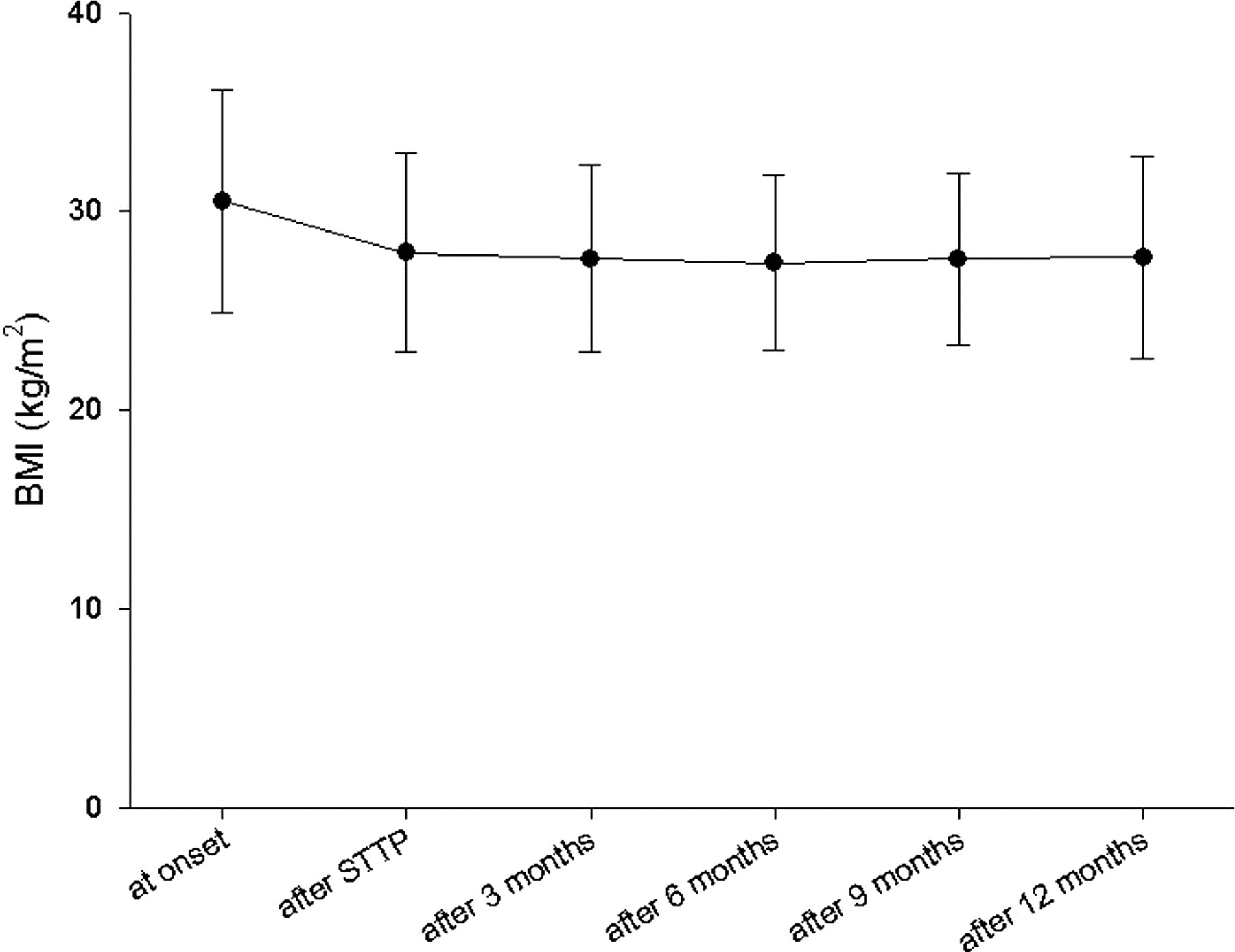
Changes in BMI during the trial (mean ± SD shown)
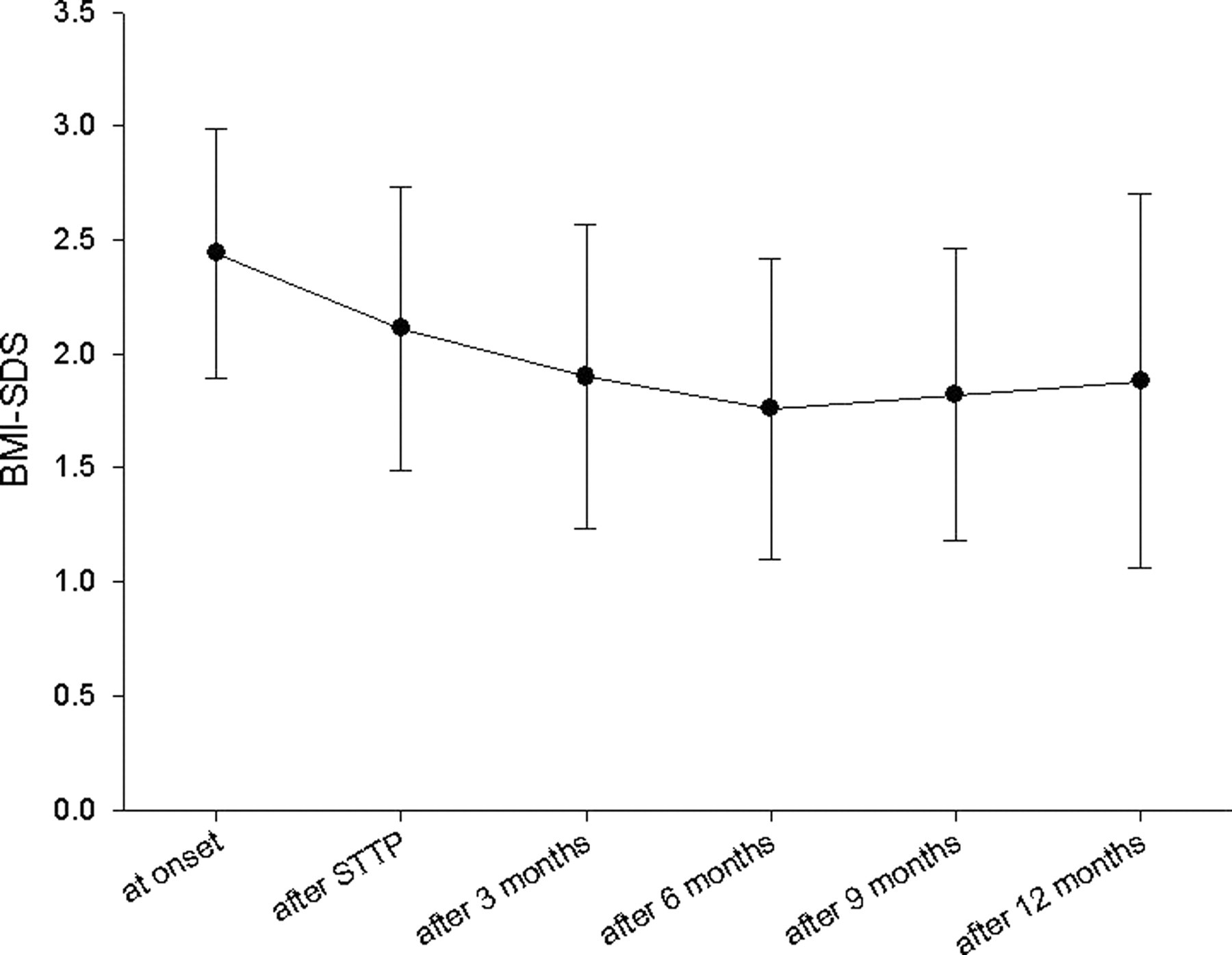
Changes in BMI-SDS during the trial (mean ± SD shown)
Psychological variables
During the follow-up period the different domains of psychological variables showed different behaviour. Wellbeing and treatment satisfaction increased between onset and six months after hospital discharge. In contrast, immediately after onset of the intervention, depression scores decreased significantly and remained stable up to the nine months follow-up. However, during the same period motivation decreased, although there was an increase in the eating behaviour scores, i.e. the subjects changed their eating habits in a positive way. A similar tendency was observed in the exercise scores (Table 2).
Changes in patients' wellbeing, depression score and the scores concerning eating behaviour and exercise during the trial (P vs value at onset)
Intervention
During the follow-up period an intervention was needed in up to 64% of the patients. The most frequent reason for intervention was poor results in exercise. The next most frequently needed intervention was for the subjects who reported low wellbeing and dissatisfaction with treatment. Although the initial scores and the scores of wellbeing/treatment satisfaction during the maintenance period were relatively high, up to 14% of patients needed an intervention to be started due to problems in this domain. There were no correlations or associations with the depression and/or motivation scores. The number of patients with intervention and the domains are shown in Table 3.
Interventions domains during the follow-up period (n [%])
Effect of the STTP for parents
Parents of 57 of the 140 children and adolescents participated in the special programme for a period of three days. Comparing the baseline characteristics and the results during the follow-up period, there were no significant differences between children and adolescents whose parents participated in the STTP and those whose parents did not.
Discussion
In the last 20 years, rates of overweight and obesity in both adults and children have risen sharply. 1–4 Increasingly it is emphasized that weight reduction and control should begin as early as childhood and adolescence. 5,11 In the present trial, a structured treatment and teaching programme following national guidelines 11 was developed and proven to be effective. The first inpatient phase demonstrated that subjects were able to achieve a significant weight reduction of about 7 kg. However, this effect is not too surprising. Other programmes 6,13 have shown similar results. Moreover, the improved results of longer inpatient duration and its correlation to the extent of weight reduction can easily be explained by the effects of continuous stimulation, strong intervention in lifestyle and eating behaviour and the dynamics of patient integration into a group setting.
More interesting, however, are the longer term results of the project. In contrast to other studies 6,14 where weight increase has occurred following hospital discharge, TeleObe demonstrates the possibility of weight stabilization. Looking at the results 12 months after participation in the structured STTP, children and adolescents' weight, BMI and BMI-SDS were still similar to, or even lower than, the values at hospital discharge.
Previous trials in Germany 15 and the US 10 have demonstrated strong acceptance and the efficacy of Internet-based intervention, including Internet counselling, counselling by telephone, mobile phone or via SMS. In particular for children and adolescents, computer and other technologies are well liked, easily accepted and frequently used. Such devices allow patients to be mobile, interactive and independent of direct face-to-face contact and control. In both the German 15 and the US project, 10 acceptance of the telemedicine support programmes was generally more than 70%, which is similar to the present trial. Children and adolescents used TeleObe mainly to have swift and convenient contact with staff, to be able to discuss problems and to receive further advice. Contact was designed only to happen at months 3, 6, 9 and 12 following STTP, but actually occurred in daily phone calls and/or emails. This ability to have frequent telemedical counselling is perhaps the principal reason for the success of the programme.
Another indicator of this positive effect is the fact that the extra training for parents provided by the STTP did not seem to have any influence. In other studies a positive influence of training for parents was shown by Brownell et al. 16 and Golan et al. 17 In TeleObe this positive effect was only present in some domains. Perhaps the groups were too small to detect differences in body weight, BMI and BMI-SDS, or perhaps, more simply, the effect of the STTP for parents was small.
In conclusion, although the present trial was a longitudinal study without a control group, telemedical follow-up care and counselling seemed to be highly effective. Telemedicine allowed not only an initial weight reduction, but long-term stabilization as well. Telemedicine support was highly accepted by patients and was also able to improve psychological determinants.
Footnotes
Acknowledgements
The project was supported by a grant from the Innoregio, DISCO-initiative, German National Ministry of Science and Education (grant no. 03i2727).