
Abstract
Summary
We evaluated the feasibility and accuracy of conducting occupational therapy home visits using the Internet. Studies were conducted at the homes of 40 patients who were scheduled to undergo a total hip or knee replacement: home visits were conducted, on the same day, by both a face-to-face therapist and an online therapist. The online therapist conducted the visit via a low-speed, dial-up Internet connection using a specially developed telerehabilitation system. This system combines real-time videoconferencing (320 x 240 pixel resolution) with a suite of calibrated assessment tools which the operator can use to measure real-scale angular displacement/velocity and linear distances during the videoconference. Both therapists completed a home environment questionnaire, assessed patients' transfer ability and measured the heights of six objects/pieces of furniture. For the questionnaire items which related to variables in the home environment, the mean percentage exact agreement was 98.9% (SD 2.6; range 90–100), while there was 100% agreement on the items related to transfers. The mean absolute difference in measured heights between the two therapists ranged from 0.1–3.3 cm. The results suggest that conducting pre-admission orthopaedic occupational therapy home visits via the Internet is both feasible and accurate.
Introduction
Osteoarthritis is the most common musculoskeletal disease in Australia and a leading cause of pain and disability, affecting about 25% of people aged over 65 years. 1 Total hip replacements and total knee replacements are frequently performed operations for osteoarthritis of the hip and knee and have been shown to be successful at reducing pain and improving function. 2,3 The incidence of these surgeries is increasing and is expected to continue to do so. 4
Before, during and after hospitalization for a hip or knee replacement, patients receive intervention from a multidisciplinary team. Occupational therapists are part of this rehabilitation team and home visits are one of the interventions typically provided by occupational therapists. Occupational therapists conduct home visits to assess patient safety, functional performance and the suitability of the patient's home environment. 5 Upon completion of a home visit, recommendations for home modifications and/or assistive equipment to improve the patient's safety and/or independence are made. The measurement of furniture heights is an essential component of orthopaedic home visits, as this ensures that furniture (including baths and toilets) is not too low, potentially causing hip dislocation postdischarge or difficulties performing transfers.
Although home visits are an important component of occupational therapy intervention, a major barrier to conducting them, even in metropolitan settings, is the travel time involved. As a result, therapists frequently rely on patients' description of their home environment when ordering assistive equipment. The accuracy of patients' descriptions and measurements are not verified. For patients who live in rural areas, home visits often cannot be performed due to the distance involved. The safety of these clients in their home environment is not assessed and modifications are usually recommended without the therapist seeing the patient's home. This is problematic as the therapist needs to observe the patient performing transfers and daily activities, ideally in their own home environment, to ensure that on discharge the patient will be able to perform necessary home tasks safely and as independently as possible. 5 If therapists are unable to observe a patient functioning in their home environment, their ability to make recommendations that will best suit the person, their occupations and environment may be compromised. Consequently, this may impinge on the patient's safety and functional performance.
At the time of planning this study, we were not aware of any existing research that had explored the feasibility of conducting occupational therapy home visits remotely. The aim of the study was to investigate the feasibility and accuracy of conducting occupational therapy home visits using the Internet.
Methods
Subjects
Between April and November 2005, all patients who were seen by an occupational therapist at the pre-admission clinic of a metropolitan hospital in Brisbane were screened for eligibility to participate in the study. Eligibility criteria were that the patient was: (1) scheduled to undergo a total hip or knee replacement at the hospital; (2) living independently in the community; and (3) assessed as ‘low-risk’ by the pre-admission clinic occupational therapist and would not receive a pre-admission home visit as part of routine care. Patients were considered to be low-risk if they lived with someone else, had not reported having a fall in the past 12 months, were not the carer of a significant other and had not expressed concerns about managing at home after the surgery. Ethics permission for the study was obtained from the appropriate committees.
Procedure
After a patient provided informed consent, a home visit was scheduled. Two research assistants, who were both occupational therapists experienced in conducting home visits, performed the home visits. One research assistant (face-to-face therapist) took the necessary equipment to each patient's house, set it up and established a dial-up Internet connection. Patients were invited to operate the equipment throughout the online home visit, and if they agreed, the face-to-face therapist explained and demonstrated the use of the equipment to them. Once this had been done, a second research assistant (the online therapist) who was located at the University of Queensland up to 50 km away, conducted an online visit. During the online visit, the online therapist communicated with the face-to-face therapist (or the patient if he/she was operating the equipment), directed them to take video pictures of various areas of the house, asked patients to demonstrate certain transfers, and took furniture height measurements using a measurement tool built into the telerehabilitation system. The online therapist also communicated with the patient and asked him or her questions. In real-time, the online therapist completed a home environment questionnaire. Immediately after the online home visit had been completed, the face-to-face therapist conducted a traditional face-to-face home visit and completed the same home environment questionnaire. During the online home visit, the face-to-face therapist was blinded to the measurements made by the online therapist.
Assessment
The Home Environment Questionnaire is a checklist that was developed by the occupational therapy department at the hospital where patients were recruited and is routinely used in clinical practice. There are 27 items about features of the home environment (Table 1), four items asking the therapist to observe and assess whether a patient can safely and independently perform various transfers (chair, bed, shower/bath and toilet), and two items assessing whether the patient uses a mobility aid (one item is concerned with inside mobility, the other with outside mobility). The response options for the 27 items that assessed the features of the home environment were either fixed choice (e.g. type of shower/bath – shower recess, shower over bath, bath, other), numerical (e.g. number of rails in the shower) or dichotomous (e.g. presence of bathboard – yes/no). The height of some pieces of furniture (main chair to be used postsurgery, bed, bath and toilet), along with the height from the floor to patients' popliteal crease (back of knee), was also measured as this enabled occupational therapists to determine the optimum height that furniture should be for patients postsurgery so that transfer ability was maximized and the risk of hip dislocation was minimized.
Percentage agreement for home environment items on the questionnaire between the online therapist and face-to-face therapist (n = 40*)
*Unless otherwise indicated in the table
Some of the information needed to complete the questionnaire was obtained by interview with patients (such as most frequently used access to the house), whereas information about other items was obtained through observation (such as location of shower handrails and transfer ability). At the conclusion of the online home visit, patients who operated the equipment were asked by the face-to-face therapist to describe how they felt about using the equipment.
Telerehabilitation equipment
Telerehabilitation assessments were performed via a low-speed (18 kbit/s) dial-up Internet connection using a telerehabilitation system (eHAB, University of Queensland, Brisbane) (Figure 1). This system combines real-time videoconferencing (320 x 240 pixel resolution) with a suite of calibrated assessment tools which the operator can use to measure real-scale angular displacement/velocity and linear distances during the videoconference. To enable the videoconference to continue while the patient/therapist mobilized throughout the home during the visit, a handycam (Sony, Australia), a wireless transmitter/receiver (Squizbiz, Melbourne, Australia) and a wireless headset (Sennheiser, Connecticut, USA) were connected to the telerehabilitation system. Real-scale linear distance measurements were made possible using a portable ultrasonic measurement device (Calculated Industries, Carson City, Nevada, USA) to record the distance between the wireless camera and the object which was to be measured. This distance was relayed verbally across the videoconference and was entered into the telerehabilitation system which used this information to perform a scalar calibration of the image. Once this was complete, the online therapist marked two points on the videoconference image relating to the distance that was to be calculated and the system computed the real-scale distance based on the scalar calibration.
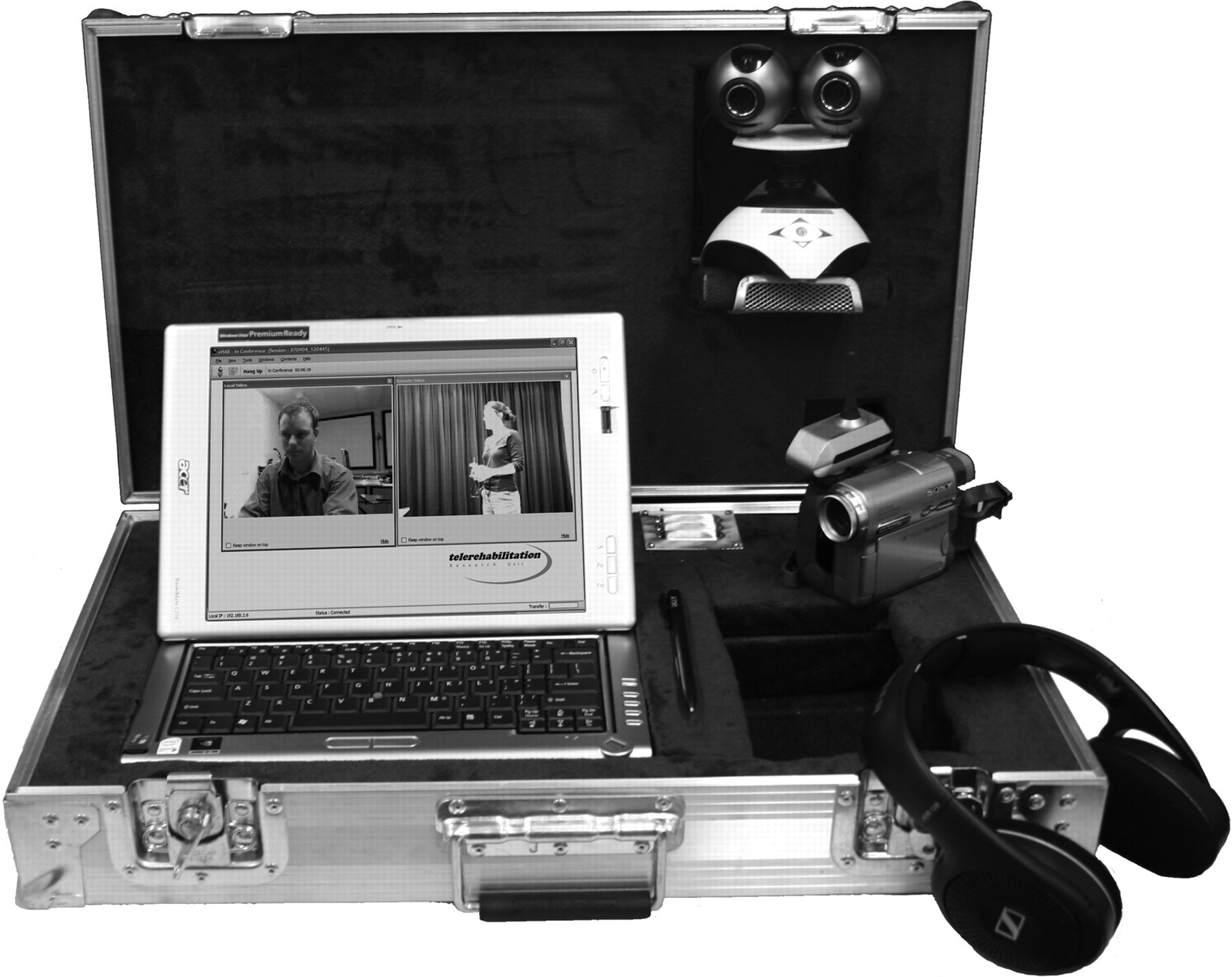
The telerehabilitation system
Data analysis
Data were analysed using the Statistical Package for the Social Sciences (SPSS version 11). The percentage exact agreement between the two therapists was calculated for the home environment items and the transfer and mobility aid items. For height measurement, the mean absolute difference between the online and face-to-face measurements was calculated for each item.
Results
Of the 148 patients who were screened for eligibility, 89 did not meet the inclusion criteria for the study. Of the remaining 59 potentially eligible patients, 19 did not provide consent, which left a final sample size of 40 patients. The patients' mean age was 68 years (SD 10, range 47–87) and 65% of patients were female. There were 12 patients (30%) scheduled to undergo a total hip replacement and 28 (70%) to receive a total knee replacement.
For the 27 questionnaire items related to variables in the home environment, the mean percentage exact agreement was 98.9% (SD 2.6, range 90–100). The percentage exact agreement for each of these items is shown in Table 1. There was 100% agreement between the two therapists for the four items related to patients' transfer ability (chair, bed, shower/bath and toilet) and the two items that assessed if patients used a mobility aid.
Table 2 shows the mean absolute difference in height measurements between the online therapist and face-to-face therapist for the furniture heights and the floor to popliteal crease measurement. The mean absolute difference in measured heights between the two therapists ranged from 0.14–3.33 cm. Table 2 also notes the frequency with which the online therapist was unable to obtain a height measure of some of the pieces of furniture.
Mean height of objects and mean absolute difference (cm) in height measurements between the online therapist and face-to-face therapist
Ten of the patients agreed to operate the equipment during the online home visit. All of these patients reported that overall, the equipment was easy for them to use, although there were a few difficulties noted. One patient reported some difficulty in understanding the online therapist at times because of audio delay and five patients reported difficulty being able to bend low enough to accurately line up the ultrasonic device when measuring the height of the step into the shower (four patients) or toilet (one patient) so the face-to-face therapist needed to operate the ultrasonic device to obtain these measurements.
Discussion
The results of this study indicate that it is feasible to conduct pre-admission orthopaedic occupational therapy home visit assessments using a telerehabilitation system. The accuracy of the online assessments was established by comparing these assessments with assessments performed in the traditional face-to-face manner. There was 100% agreement between the two therapists for 22 of the 27 questionnaire items that related to variables in the home environment. For the remaining five questionnaire items, agreement ranged from 90–97.5%. Two of these items related to the slope of the land in the patients' lawn and the online therapist was sometimes (in four of the visits) unable to accurately judge the slope. This difficulty probably occurred because the camera was carried and sometimes inadvertently held at a slight tilt, which made detecting the slope on a 2D image difficult. In two of the visits, the online therapist failed to report the presence of loose floor mats in the house and a bedroom nightlight. These errors may have occurred because detection of these objects required a general scanning of the room environment and the online therapist's view of the room was restricted to the areas of the room that she instructed the person operating the camera to film. In future studies, it is recommended that the online therapist instruct the person operating the camera to pan around the room with the camera on entering each room, so that objects such as these can be detected.
There was 100% agreement between the therapists for the four questions about patients' transfer ability and the two questions about patients' use of mobility aids. However, it is important to note that these questions were only a gross screen of patients' functional ability, not a detailed assessment of functional ability. Further studies should explore the feasibility and accuracy of conducting functional assessments (such as self-care and mobility assessments) using the Internet.
The mean absolute difference in measured heights between the two therapists ranged from 0.1–3.3 cm. To the best of our knowledge, there are no published values as to what height difference between therapists would be considered clinically acceptable. With the exception of bed heights (2.4 cm) and bath heights (3.3 cm), the difference between the two therapists on other measurements was less than 2 cm, a difference which is unlikely to be of clinical significance. When measurements are being taken for the purpose of organizing permanent home modifications (such as handrail installation), exact measurements are important, but that was not the purpose of the measurements that were taken in the present study.
There are a number of possible reasons that may explain the inaccuracies in height measurements that were found between the two therapists. First, the ultrasonic device was found to have aberrant behaviour when used on surfaces such as porcelain baths and this may explain the large variation in bath height measurements between the two therapists. Second, in some situations, due to the spread of the ultrasound beam, objects in the room other than the one being measured were detected and measured by the device. For example, it was noted that the device sometimes returned a measurement for the toilet cistern when a measurement of the toilet pan was intended. Consequently, this resulted in the incorrect horizontal distance from the object being used to calculate the vertical height of the object. Third, in some situations, there may have been parallax measurement error due to the camera not being held perpendicular to the item being measured. This was unavoidable in some situations, typically when the object/furniture was in a small room. This problem also resulted in the online therapist being unable to measure the height of some furniture in a few (10) situations (Table 2), because the layout of some rooms did not enable the object of interest to fit in the field-of-view of the camera. Two suggestions for overcoming some of these difficulties in future studies are: (1) the use of an alternative distance measurement device instead of an ultrasonic device; and (2) controlling parallax measurement error through education of users of the equipment and the development of protocols on the usage of the camera.
Although all of the patients who operated the equipment themselves reported that it was easy to use, difficulties with bending low enough to line up the ultrasonic device to measure some objects (most frequently the step into the shower) were experienced by five patients. Mounting the ultrasonic device and camera on a frame that enables the user to lower the equipment without having to bend may provide a solution to this problem.
The only other study that has explored the use of telerehabilitation to assess the home environment was conducted by Sanford et al. 6 and was published after planning for the present study had commenced. The online home visits that were conducted in Sanford et al.'s study used a videophone, video camera and wireless audio/video transmission equipment and assessments were conducted by both an in-home and online occupational therapist, although these were done up to two weeks apart. The aim of Sanford et al.'s study was to identify home modification needs and it was reported that the online assessment identified 86% of the home accessibility problems that were identified by the in-home assessment. There are a number of differences between the telerehabilitation protocol used in Sanford et al.'s study and that used in our study which limit comparison of the results. Unlike our study in which all aspects of the home visit were completed in the one online visit, the home visits that were conducted in Sanford et al.'s study involved a three-step process in which a disposable camera was provided to the patient/family before the visit to enable photographs of the home to be taken, a telephone or in-person interview was then conducted with the patient/family, and finally, the online home visit was conducted. Sanford et al.'s study used the case studies of three patients but the actual homes assessed in the study did not belong to the patients, but to hospital staff members. Furthermore, the patients were not present during the visits, the patients' functional abilities (such as transfers) in the home environment were not assessed and no measurements were able to be taken by the online therapist using the telerehabilitation system.
The present study demonstrates the potential for telerehabilitation to enable pre-admission orthopaedic occupational therapy home visits to be conducted using the Internet. However, some limitations of the study limit the generalizability of the results. The small sample size of 40 patients was recruited from a single metropolitan hospital and consisted only of people requiring a hip or knee replacement. Further research that involves patients with other medical conditions would be valuable as the difficulty of home assessments can vary according to clients' needs. Variation as to whether the equipment at the patient's house was operated by the patient or the face-to-face therapist may have introduced additional variables into the study that were not accounted for. Further research that involves patients (or their family) performing the set-up of the equipment and using it without the presence of study personnel would provide valuable information about the clinical usefulness of the system, as would a trial of the telerehabilitation system with patients who live in rural and remote areas. Nonetheless, the present study confirms the feasibility and accuracy of conducting pre-admission orthopaedic occupational therapy home visits using the Internet and this has important implications for the delivery of occupational therapy services to people who require home visits and live in rural and remote locations.
Footnotes
Acknowledgements
We are grateful for the support and assistance of Linda Hansen and the occupational therapists at the Queen Elizabeth II Hospital, and Laura Desha and Kathryn Wenham for conducting the home visits. eHAB is a trade mark.