
Abstract
Summary
We conducted a retrospective review to assess the potential for Emergency Nurse Practitioners (ENPs) to deliver telemedicine advice for minor injuries. Over a one-year study period, 835 patients from 15 minor injury units in community hospitals presented to the minor injuries telemedicine service and were seen via videoconferencing by a doctor at the Aberdeen emergency department. A case review showed that overall, ENPs were considered capable of treating 470 of 788 new presentations (60%). If children under 14 years of age and shoulder injuries were excluded, this figure rose to 84%. Assessment of all minor injuries via a telemedicine network by medical staff is unnecessary. An ENP-led service offers a realistic and attractive alternative.
Introduction
In recent years, the delivery of care for minor injuries in large Emergency Departments (EDs) has changed. Traditionally, all patients presenting to an ED would be seen by a doctor. However, several factors have made this system unsustainable. The European Working Time Directive and the introduction of Modernising Medical Careers have reduced the number of medical manpower hours available for clinical care. Also, the Department of Health has recently required EDs in the UK to ensure that patients are seen, treated, and admitted or discharged in less than four hours. This has led to alternative models for managing minor injuries, which make up the majority of the workload of EDs.
One model is service delivery by Emergency Nurse Practitioners (ENPs) and these have now become firmly established in routine working practice. 1,2 Working within agreed guidelines, they see, investigate, treat and discharge patients with minor injuries autonomously. Their activities are supported by senior ED staff, whom they may consult for advice. It has been shown that ENPs offer a safe and effective service for the treatment of minor injuries. 1
The minor injuries telemedicine network in Grampian connects 15 minor injury units (MIUs) in community hospitals to the teaching hospital ED at the Aberdeen Royal Infirmary (ARI) and has been described elsewhere. 3 Patients are seen in the MIUs mainly by community hospital nurses with minor injury training, and in a proportion of cases, they use telemedicine to obtain advice from the main Aberdeen ED. The telemedicine advice service in Aberdeen is staffed by middle grade medical staff and consultants. When the telemedicine service was established, all patients presenting directly to the Aberdeen ED were seen by a doctor. Subsequently, to relieve pressure on the ED in Aberdeen, ENPs were introduced there. However, this has led to an anomaly in which patients presenting directly to the teaching hospital ED may be seen by an ENP, but if referred via the telemedicine network from a community hospital, will be seen by a senior ED physician.
The aim of the present study was to assess the potential for ENPs to deliver telemedicine advice for minor injuries.
Methods
A retrospective study was undertaken. Using the current clinical remit of the ENPs in Aberdeen, a set of exclusion criteria for patients not eligible to be seen by a nurse practitioner was established.
Clinical details of all minor injuries teleconsultations referred from peripheral MIUs are recorded in a central database. Information about all consultations conducted over a one-year period beginning from August 2003 were entered into a spreadsheet. The ENP exclusion criteria were then applied to the database by two emergency medicine consultants to assess the potential for telemedicine advice to be primarily delivered by ENPs. Cases where there was insufficient data to decide if the case fitted the exclusion criteria were assumed to require a doctor.
Aberdeen has a children's hospital with an ED which sees all children aged under 14 years of age with minor injuries. While the same medical staff treat patients at both the adult and the children's EDs, the ENP service at the adult ED does not see children. The minor injuries telemedicine service, however, sees children of all ages. In addition, during the period studied, the ENP service was developing and was limited in the range of injuries it dealt with. The range of conditions has subsequently been expanded.
Results
Over the one-year study period, 835 new patients from peripheral MIUs presented to the minor injuries telemedicine service and were seen via videoconferencing by a doctor at the Aberdeen ED. Forty-seven patients had already been assessed locally by medical practitioners and referred for specialist opinion and were excluded from further analysis. Of the remaining 788 new patients, 436 (55%) were male. The median age of the patients was 28 years (range 1–96). The diagnosis in the majority of cases was either fractures or soft tissue injuries affecting the limbs (Figure 1).
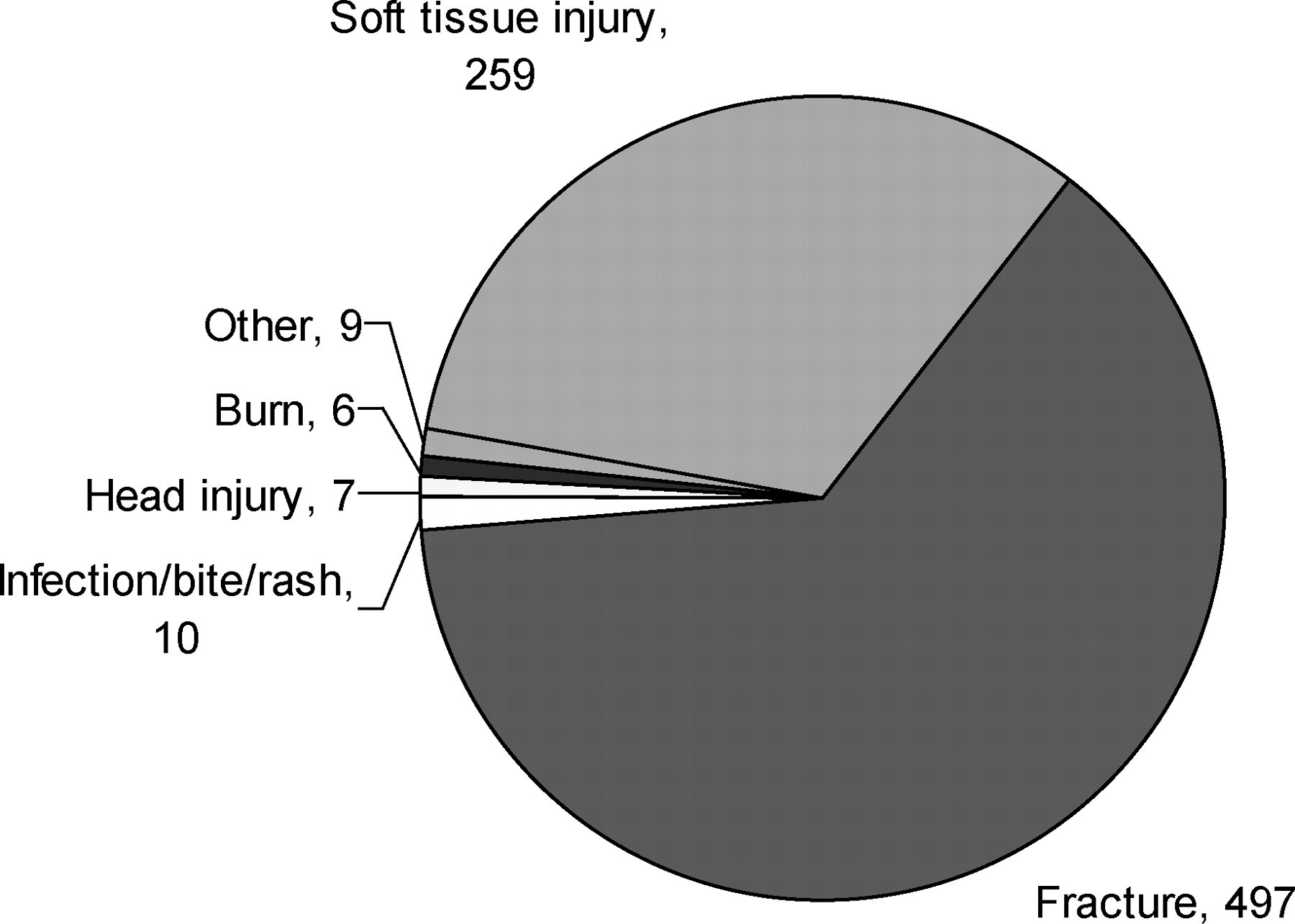
Injury type (n = 788)
The case review showed that overall, ENPs were considered capable of treating 470 of the presentations (60%). The excluded diagnoses are shown in Figure 2. A few of the cases were excluded for more than one reason.

Excluded diagnoses (n = 338)
Of the 318 excluded patients (40%), most did not satisfy the ENP criteria, either because they were too young (n = 167) or had sustained injuries involving the shoulder area (n = 65) which was outside the remit of the ENPs at that time. If children aged under 14 years were excluded from the analysis, the ENPs could have assessed 76% of the remaining cases. Exclusion of shoulder injuries would increase the proportion to 84% of cases.
Discussion
The use of telemedicine to deliver minor injuries care has been shown to be safe, effective 4 and does not require acquisition of any special skills. We have shown that ENPs have the potential to independently manage 60% of all patients referred to the Grampian minor injuries telemedicine service from MIUs over a one-year period, and up to 84% of cases if children under the age of 14 years and shoulder injuries are excluded from analysis. The success of ENPs in emergency medicine has already resulted in protocols being extended to increase the number of conditions and injuries treated. Similarly, ENPs in general EDs treat both adults and children. 5 This further enhances the potential for a primarily ENP-delivered minor injuries telemedicine service to be developed.
The Scottish Government's policy document ‘Better Health, Better Care’ 6 advocates generic competencies across professional boundaries and the increased use of telemedicine in delivering safe, cost-effective care as close to the patient's home as possible in Scotland. Assessment of all minor injuries via a telemedicine network by medical staff is unnecessary. An ENP-led service offers a realistic and attractive alternative.
Footnotes
Acknowledgements
We thank the Scottish Centre for Telehealth for support.