
Abstract
Summary
We reviewed five years' experience of providing ground-to-air medical advice for commercial passenger aircraft. A total of 273 events occurred in-flight where further advice was sought. The most common age group resulting in calls were from those aged 21–30 years, who generated 38 calls (16%). The 273 cases included gastrointestinal conditions (26%), neurological (22%) and cardiovascular events (14%). Most incidents were managed conservatively in-flight with oxygen and/or other medications. Aircraft diversion occurred on 9% of occasions; cardiovascular and neurological emergencies were the major cause of this. Collaboration between aviation providers should be considered to develop a common database of in-flight emergencies so that contents of medical kits can be standardized in order to improve the quality of care in the air.
Introduction
Commercial air travel continues to increase in popularity. The introduction of low-cost airlines has led to increasing numbers of passengers, many of whom are elderly with chronic disease conditions. A concomitant increase of in-flight emergencies has resulted. 1 There has been speculation in the media regarding the effects of the aircraft environment contributing to pathology in passengers. 2 Cabin crew are required to be competent in first aid and advising on minor ailments. Medical equipment is available on all commercial passenger aircraft and normally consists of a section for first aid and a further section for use by any doctor offering assistance. However, many clinicians responding to in-flight emergencies do not routinely deal with emergencies in their day-to-day practice and most have no specialist knowledge of the in-flight cabin environment and facilities available to treat passengers. 3 The consequences can be inappropriate treatment and unnecessary diversion of aircraft.
This has led to the emergence of commercial companies offering immediate access to emergency physicians who can provide ground-to-air medical advice. One UK company, the International Medical Centre, utilizes staff at the Emergency Department of Aberdeen Royal Infirmary to provide ground-to-air medical advice. Airlines subscribing to the service are supplied with a specially designed pro forma to complete for all in-flight emergencies. The form ensures that the maximum amount of information is passed to the doctor, in a structured and methodical way, as quickly as possible. If the radio connection is of poor quality, information may be transmitted in alpha-numeric form. Advice is then given on probable differential diagnosis, treatment to be given while in-flight and whether there is any indication for the flight to be diverted from its course.
We report five years' experience of providing ground-to-air medical advice in this way.
Methods
We conducted a retrospective analysis of the case records for all calls received by the service between 1 January 2001 and 31 December 2006. All contacts for in-flight medical advice were recorded on the aircraft and at the advice centre. Details, including demographics of the patients involved, presence of any health-care professionals on the flight, action taken and medications utilized were entered into a database for analysis.
Results
There were 354 reported events recorded over the five-year study period. There were 273 (77%) calls made during flight and 73 (21%) calls made before the aircraft departed. In eight (2%) cases, there was insufficient data to ascertain when the event occurred and they were excluded from subsequent analysis.
Of the 273 events occurring in flight, gender was recorded in 263 cases. One hundred and forty-six (56%) patients were women. The mean age of the 236 patients in which it was recorded was 42 years (range 1–87).
The most common age group resulting in calls were from those aged 21–30 years, who generated 38 calls (16%) (Figure 1). The fewest calls were received for the age group 5 years and under, with only 12 (5%) calls taken. Gastrointestinal/endocrine cases most frequently resulted in a request for assistance (Figure 2). Six calls were assigned a value of ‘Other’ where they did not fit into any other category, including two passengers with nail glue in their eyes and four calls in which the matter had been resolved by the time contact was established.
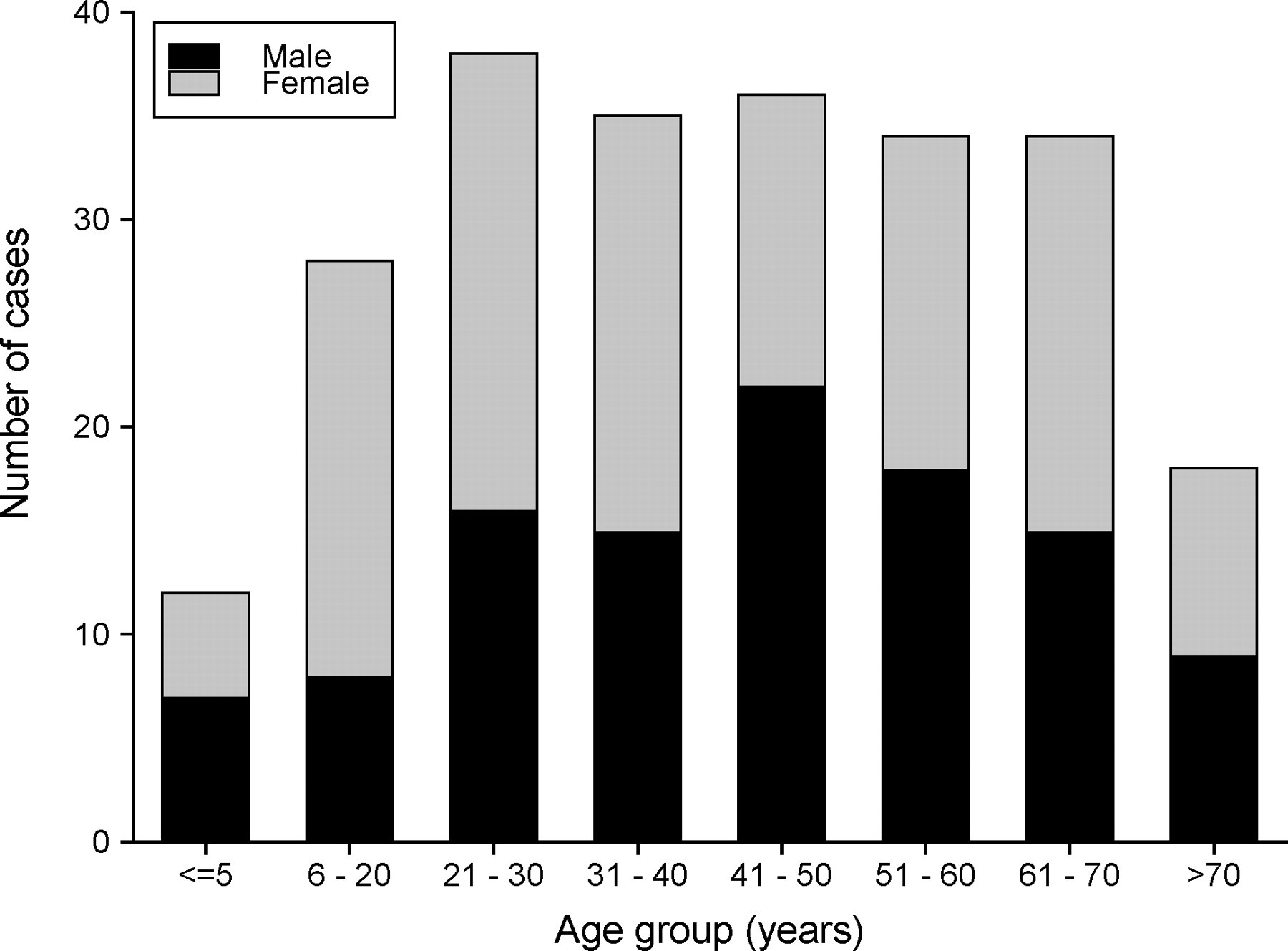
Age and gender of patients
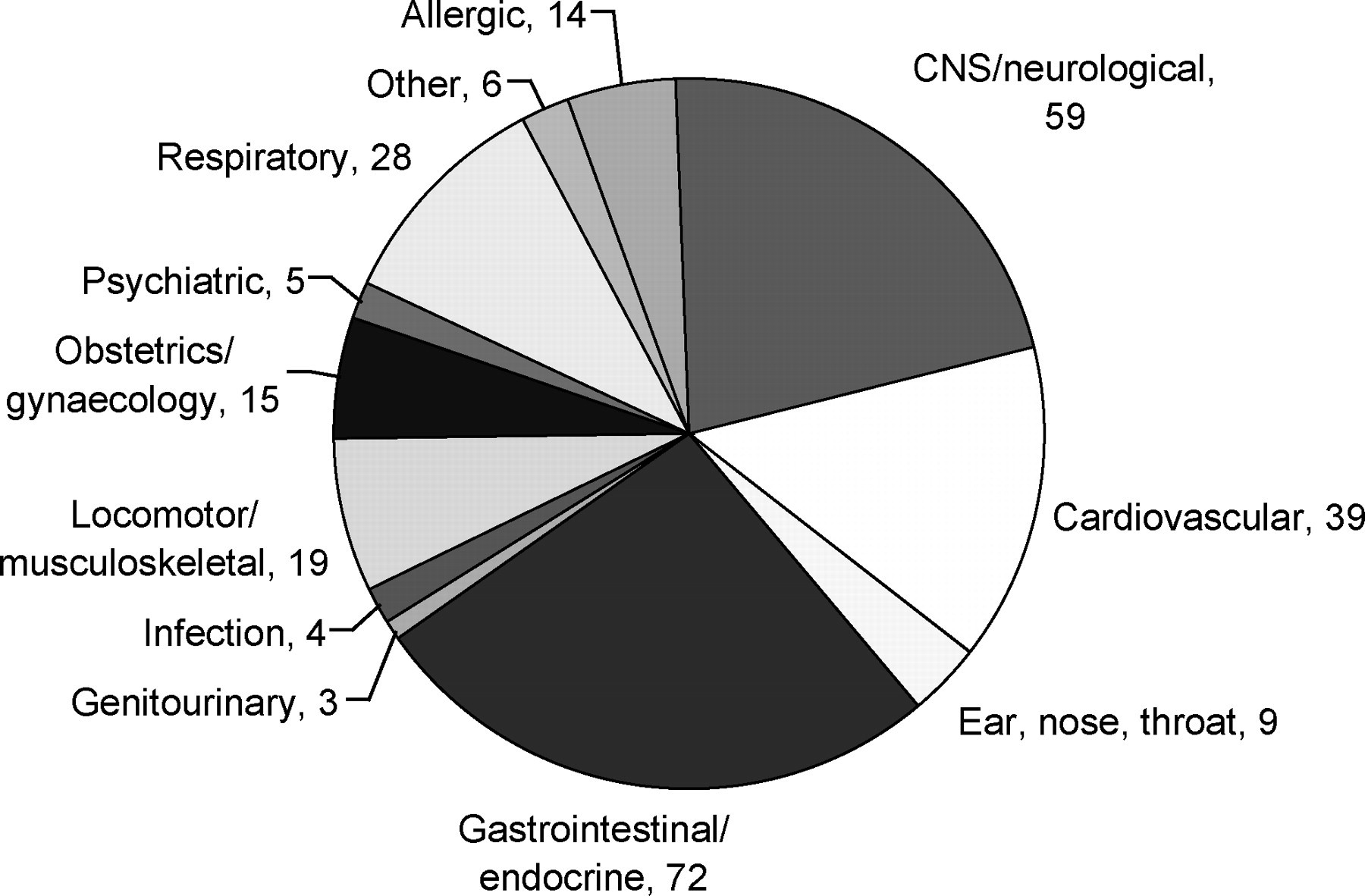
Illness/complaint category (n = 273)
Details of the initial care given by the on-board personnel prior to contact were recorded in 233 (85%) cases. Oxygen was the most frequently given ‘medication’ in the management of in-flight medical emergencies, being received by 104 (45%) passengers (Figure 3). A further 39 were given oxygen on the basis of the ground-based medical advice.
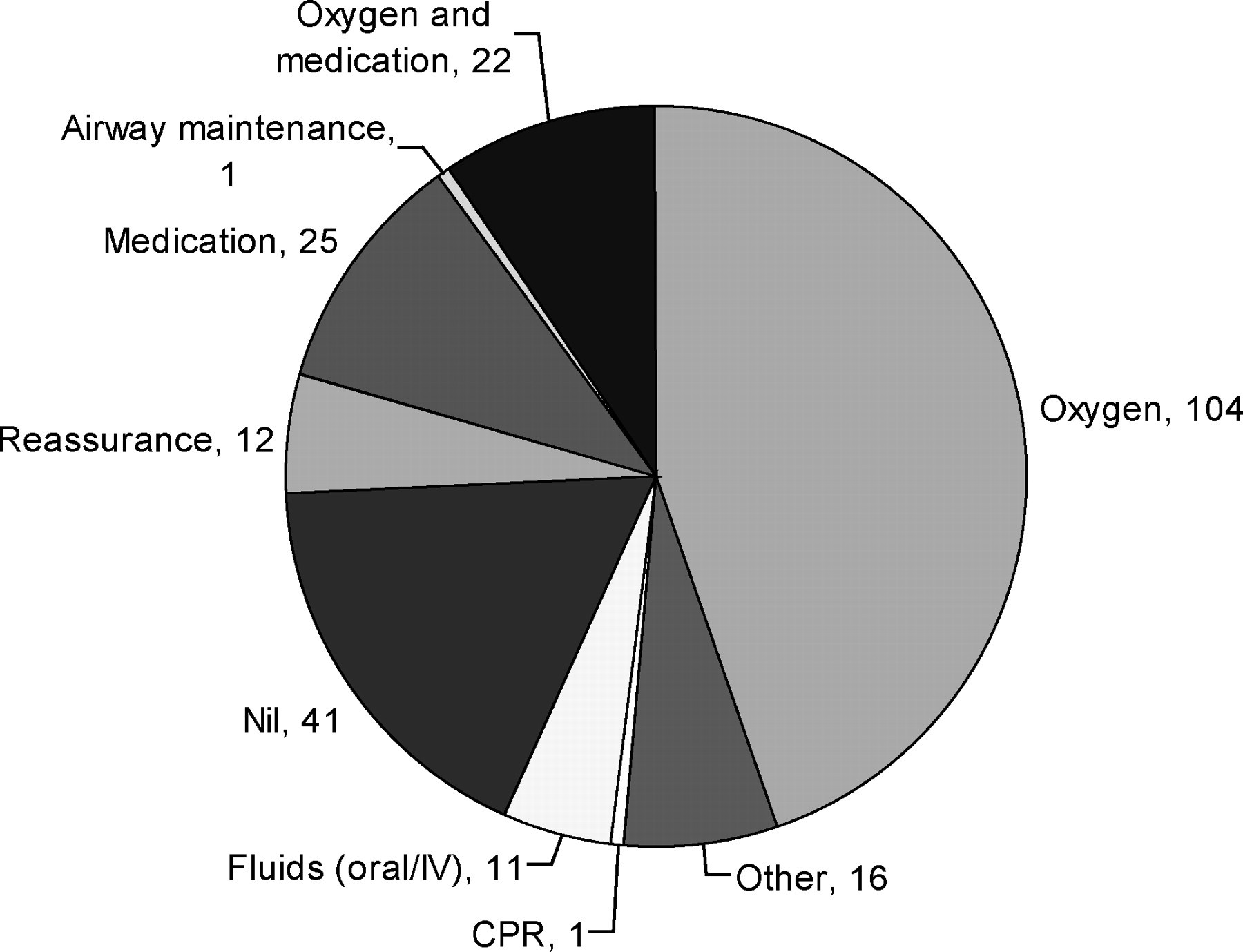
Initial care given on board (n = 233)
In all cases, including both prior to contact and on the advice of ground-based medical teams; analgesia was given in 17% of cases. This included the use of paracetamol and non-steroidal anti-inflammatory drugs, as well as other forms of analgesia, including those given parenterally. Fluids were required in 31 passengers (9.5%) (Table 1).
Medications administered to passenger (initially or after contact with ground-based medical advice)
Diverted flights
Of the 273 in-flight emergency calls, the aircraft was diverted to an airport other than the scheduled destination on 24 occasions (9%). The mean age of the ill passenger in diverted flights was 54 years (range 20–74).
Cardiovascular causes represented the greatest cause for diversion with 11 diversions (29% of cardiac cases were diverted), followed by neurological cases (12% of CNS/neurological cases were diverted).
There were 145 (53%) recorded incidents where there was found to be another health-care professional (i.e. doctor, nurse or allied health professional) on board during the in-flight event. The presence of other health-care professionals was not associated with an increase in the rate of diversions (χ2 = 2.9, P < 0.10). Passengers currently taking medications were associated with an increased rate of flight diversion (χ2 = 8.7, P < 0.003). The age of the passengers did not affect diversion rate with no significant difference between patients over the age of 51 years and those under the age of 51 (χ2 = 2.6, P < 0.11).
Discussion
Modern aircraft cruise at altitudes of 35,000–43,000 feet (10,700–13,100 m). The aircraft cabin is pressurized to the equivalent of 6000–8000 feet (1950–2400 m). For structural reasons, the cabin cannot be pressurized to an equivalent of sea level. Thus there is less oxygen available in the cabin and a reduction of about 10% in the saturation of haemoglobin occurs. This reduced partial pressure of oxygen is of no consequence to a fit individual, but may affect those with cardiovascular or respiratory disorders. However, our data suggest that most medical emergencies arising in flight are not as a result of the cabin environment but due to pre-existing illness or first presentation of a self-limiting condition.
Age did not appear to be a significant factor in the group of patients studied. The majority of in-flight incidents were managed by the use of oxygen and simple medications alone. Many patients with pre-existing disease will be carrying relevant medication with them. However, many patients store their medications in their hold luggage and so it will be inaccessible. 4 The contents of medical kits carried on board have mainly been determined by consensus among senior medical staff rather than being based on evidence. There exists the potential to develop evidence-based medical kits tailored to the likely problems to be encountered. Further study is required to see if the pattern of medical emergencies presenting in flight varies with the type or purpose of the flight, e.g. short versus long haul, chartered versus scheduled.
In the present study, diversion appeared more likely if the presenting feature was chest pain or loss of consciousness. The development of specific algorithms to assess these conditions combined with specialist ground-to-air advice (and possibly additional diagnostics on board) may reduce unnecessary, potentially hazardous and expensive diversions.
Pre-flight screening based on the likely conditions to be encountered in flight, and particularly those commonly resulting in diversion, may further reduce the likelihood of in-flight emergencies occurring. However, it is clear that there will still be a significant number of conditions which will present for the first time in flight. Fortunately, serious in-flight emergencies requiring ground-to-air medical support are relatively rare. However, this means that most reported studies 5–8 are of relatively small scale and varying definitions making extrapolation of the data to inform future training of air crew and contents of medical kits difficult. 9 The aviation industry as a whole should consider developing a common database for in-flight emergencies to improve the quality of care in the air.
The commonly held belief that in-flight emergencies are contributed to by the cabin environment and an aging passenger population was not supported in the present study. Most in-flight emergencies may be managed by oxygen, simple medications and ground-to-air support. Future research by the aviation industry has the potential to further improve management of in-flight emergencies with resultant benefits for passengers and the airline.
Footnotes
Acknowledgements
We thank First Call Ltd who supplied the data. We also thank Mrs Ann Kelman and the Scottish Centre for Telehealth for support.