
Abstract
Summary
With the increase in demand for high quality medical services, the need for an innovative hospital information system has become essential. An improved system has been implemented in all hospital units of the Yonsei University Health System. Interoperability between multi-units required appropriate hardware infrastructure and software architecture. This large-scale hospital information system encompassed PACS (Picture Archiving and Communications Systems), EMR (Electronic Medical Records) and ERP (Enterprise Resource Planning). It involved two tertiary hospitals and 50 community hospitals. The monthly data production rate by the integrated hospital information system is about 1.8 TByte and the total quantity of data produced so far is about 60 TByte. Large scale information exchange and sharing will be particularly useful for telemedicine applications.
Introduction
The idea of a unified health-care information infrastructure has received considerable attention due to advances in digital communications and hospital information technologies. There is also a strong demand for high quality health-care services to be provided without the usual limitations of time and location. This will require dynamic linkages between health-care units such as patients, doctors, nurses and other staff, as well as linkages between homes, community hospitals and large scale tertiary hospitals. 1 The integration of hospital information infrastructures, both within and between hospitals, will be necessary to provide patients with continuous medical services. Both wired and wireless communication channels will be required.
As the first step towards interoperability between health-care units, we have investigated the large-scale integration of hospital information systems in the Yonsei University Health System.
Methods
All data produced at the hospital should be digitally recorded, stored and communicated if health-care data are to be exchanged efficiently within the hospital and outside the hospital. To meet this requirement, an integrated hardware infrastructure was developed which provided safe paths for data delivery; for outside the hospital communication, high bandwidth networks were employed, such as FTTH (optical fibre to the home) and VDSL (very high speed digital subscriber lines). For within hospital communications, wired (an optical fibre-based backbone network) and wireless LANs were used. For access to physicians through mobile devices, CDMA (Code Division Multiple Access) and WIBRO (Wireless Broadband Internet) were used. In addition, since the data must be protected from unauthorized access, a VPN (Virtual Private Network) based security system and SID (smart card-based patient identification) system was applied.
While the hardware infrastructure guaranteed the safe delivery of the electronic data, the software architecture provided users with an understandable representation of the delivered data. 2 The implemented architecture had a three-tier structure: a tier for PC users, a business logic tier for the application server and a data access tier for the database server. Within this structure, an XML-based web architecture was applied to provide flexibility during the exchange of data in a common format and security, including the authentication of the user and encryption for data protection. 3 The major problem during the process of integrating the software architecture was the stable delivery of the real meaning implied in the data. SNOMED-CT (Systematized Nomenclature of Medicine Clinical Terms) and ICD (International Classification of Disease) 9/10 were used as the standardized medical terminology in the hospital information system.
With the appropriate hardware infrastructure and software architecture, the hospital information system was implemented, by interconnecting various agents through the hospital portals, terminal servers, mobile devices and desktops. Due to the diverse forms of data exchange among multiple units, adapted agents were used for the interconnections. The interconnections have different forms whether it is within the hospital or outside the hospital. Within the hospital, the PACS (Picture Archiving and Communications Systems) including general radiology PACS, cardiology PACS and dental PACS, CDMS (Cardiac Data Management System), POES (Physician Order Entry System), EMR (Electronic Medical Records) and ERP (Enterprise Resource Planning) system are used for the delivery of patient data and efficient management of human resources. Outside the hospital, any patients, community hospitals or physicians away from the hospital may access information via the hospital portal. The information system thus required the integration of various technologies and infrastructures (Figure 1).
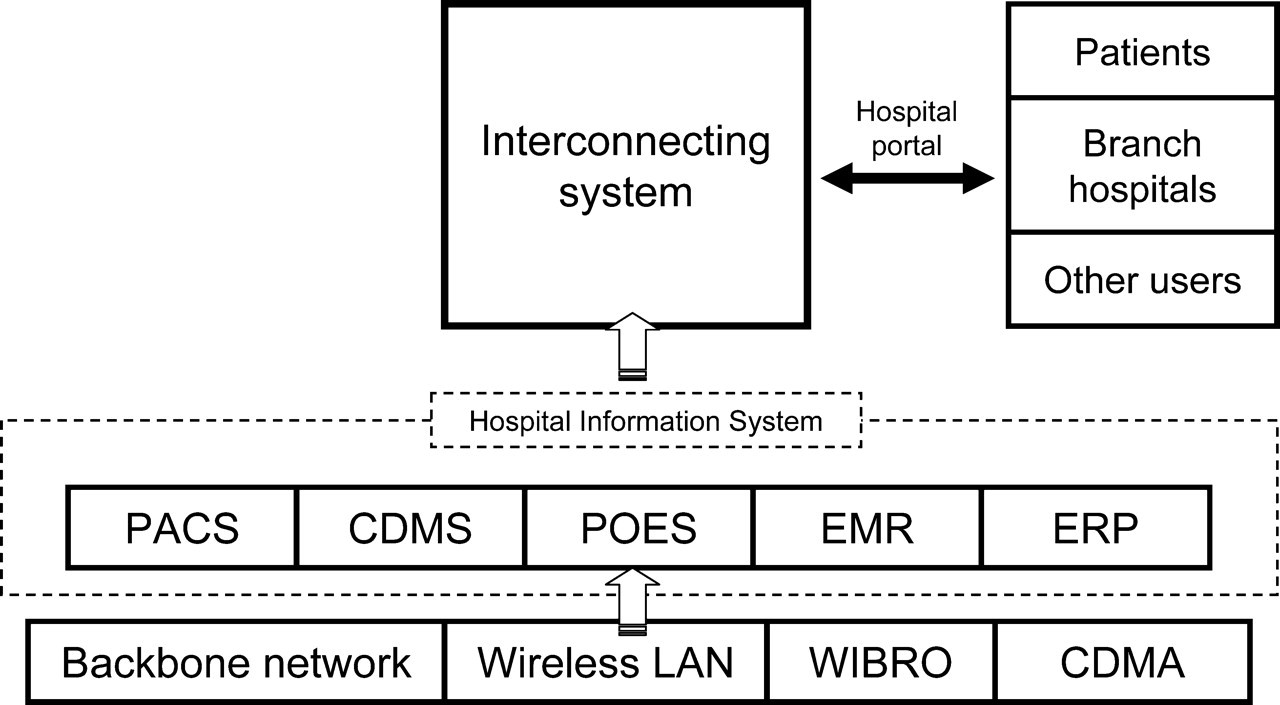
Architecture of the integrated hospital information system
Results
A large-scale hospital information system was first integrated in November 2005. There were two tertiary hospitals and 50 community hospitals. The monthly data production rate by the integrated hospital information system is about 1.8 TByte and the total quantity of data produced is about 60 TByte at the time of writing. The number of staff in the hospital and the number of patients who have visited can be judged by the number of smart ID cards issued. From November 2005 to October 2007 there were 8216 staff and 560,731 patients. The integrated system turned out to be essential for exchanging and supporting multi-unit health-care services.
Discussion
In terms of interoperability, diverse system integration was the first step in seeking the interoperability required for a ubiquitous hospital information system. In the interests of technical interoperability, we organized the intranet and Internet of the hospital. For within-hospital communications, hybrid wired and wireless networks using an optical fibre based backbone and wireless LAN infra- structures were installed. For outside hospital communications, high speed wired backbone networks were utilized, as well as WIBRO and CDMA-based 3G cellular networks. One of the main problems in any hospital information system, the security necessary to ensure the privacy of patient data, must be managed carefully. 3 Access to patient data should be allowed only to an authenticated person. The SID system was fully implemented for this purpose. In addition, the access and use of patient data is limited to the appropriate physician and all data-access is recorded electronically.
In addition to integration of components of the hardware infrastructure for technical interoperability, the integration of the software architectures requires semantic interoperability. Because of the differences in the descriptions of the terminologies, the smart integration of these discrepancies is also important. Thus special agents using terminal server-based interfaces such as the BizTalk server and .Net architecture like the web-server-based interface were used to permit data exchange and to support health-care services between different health-care units. The data exchange and management are performed by means of XML messages, SNOMED-CT or ICD 9/10. Process interoperability coordinates work flow of the care teams so that they are able to access information to treat the patient in the most effective and safe way possible. The CDR (Clinical Data Repository) for medical research and CDSS (Clinical Decision Support System), based on the EMR, which alerts the physician to drug conflicts, duplicated orders or any incomplete medical records, can be considered as the result of process interoperability. In addition, ERP is imported for good interoperability in the view of the administrators of the hospital. The mobile system of the hospital also improves the quality of medical services from the hospital. Access to patients' electronic records via mobile phone allows physicians to give medical instructions or advice even when outside the hospital.
The realization of a full-digital hospital environment with secure means of identification and sufficient communication capability is a prerequisite for supporting health-care data exchange and individualized health-care services. There remain many other matters to be considered before the implementation and operation of large-scale hospital information systems. The inclusion of diverse hospital information systems, communication and network infrastructures, and software components enable information exchange among multiple health-care units in an efficient and secure manner as well as forming a basis for supporting individualized self-care without the limitations of location and time. Those information exchange and sharing capabilities are particularly useful for telemedicine applications. The digital representation of patient information can facilitate cooperative patient care among multi health-care units through a telemedicine system.
Footnotes
Acknowledgements
We thank the Yonsei University Health System. The study was supported by a grant from the Ministry of Health and Welfare, Korea (A020608).