
Abstract
E-health based on mobile wireless networks is called mobile e-health. Mobile e-health can facilitate computer-supported cooperative work, which encompasses tasks from email and instant messaging to wireless information sharing through broadband and telecommunication networks. In the development of cooperative management systems, the concept of ‘awareness level’ has been introduced. This is based on factors such as the location and actions of the user involved. Mobile e-health can help to achieve cooperation by providing the right awareness levels at the right time. The improved awareness levels allow health professionals to provide patient care with better quality and efficiency. Mobile e-health systems have the potential to take over the mundane tasks of the doctor so that better quality health services can be provided.
Introduction
E-health can be expected to make health services more efficient and improve access to care, especially for people with disabilities, for the elderly and for those in remote areas. It should benefit health-care providers, professionals and final users through higher quality of care and health promotion. It should also affect the cost of care by reducing redundancy and duplication of examinations, and making possible economies of scale. Thus e-health will be important to the goals of international development in bridging the gap between industrialized and developing countries. 1
E-health based on mobile wireless networks is called mobile e-health. The International Telecommunication Union (ITU-D) has promoted mobile e-health in developing countries at the IEEE Healthcom 2004 conference, which involved 20 countries. This led to the development of e-health kiosks for developing countries. The consortium undertook the trials of e-health kiosks in Tsunami-affected areas of Indonesia and India in 2005. 2 Our experience in this project formed the basis of the new cooperative management infrastructure described below.
Cooperative working
Computer-supported cooperative work (CSCW) provides business processes (i.e. health-care processes) with the possibilities of information technologies such as mobile wireless. 1 In the health-care context, patients and health professionals must work together (often from a distance) in order to diagnose and deliver the best possible solution to a health problem. With recent advances in information and communication technologies (e.g. intelligent agents), it is now possible for health-care professionals to work cooperatively. 1
E-health kiosks
In 2004 a collaboration began between the ITU-D and the IEEE Communication Society to promote e-healthcare in developing countries using wireless mobile information technologies. The work was intended to demonstrate how collaboration between industrialized and developing countries can lead to a successful e-health policy in developing countries, particularly in remote communities. 2
The collaboration covered three main activities: disaster telemedicine, epidemic control and bio-terrorism. However, disaster telemedicine received most attention because of the Tsunami which occurred just after the project was launched in September 2004. The work was supported by many organizations, including Technologie Sans Frontiers, IBM, Netstar and the Westmead Children's Hospital in Sydney.
The consortium developed e-health kiosks for use in remote locations in developing countries. Basically, the telemedicine system consisted of at least one fixed central community health-care unit, a number of movable/mobile health-care units (e-health kiosks, each with a power supply unit), PC servers, telecommunications infrastructure, Internet access and appropriate transport vehicles. 3 Trials were conducted at Banda Aceh in Indonesia in August 2005. The trial exposed severe limitations in the telecommunications infrastructure in Banda Aceh at that time.
The trial provided information about the requirements for a future mobile phone-based e-health kiosk. The proposed system would eliminate the need for an expensive laptop computer for building e-health kiosks for developing countries.
Cooperative management
Cooperative management is the term used to describe models, processes, notations and tools used for managing business processes (e.g. health care) that involve the collaboration of multiple human roles assisted by networked information systems. Many of these models and techniques have been borrowed from the area of CSCW. The concept of CSCW was first introduced in 1984. 1 At present, the field of CSCW encompasses tasks from email and instant messaging to wireless information sharing through broadband and telecommunication networks. Typically CSCW designs are realized using communication technologies and intelligent software agents. The term ‘agent’ is ‘an entity which functions continuously and autonomously’ in some domain that may involve interaction with other processes and/or agents. 4
Measuring cooperation
According to the old saying, ‘you can't manage something that you can't measure’, one of the most important considerations is defining a measure of cooperation. There have been some attempts to measure cooperation using the concept of awareness where each group member becomes aware of other members' activities by increasing ‘focus’ (information pull), and would make his/her activities known to other group members by increasing ‘nimbus’ (information push). 5,6 Although this idea offers some conceptual understanding of measures of cooperation, it is not adequate for the development of cooperative management systems.
Hence the concept of ‘awareness level’ has been introduced. This is based on factors such as the location and actions of the user involved (Table 1). Some matters raised about awareness include ‘what information to provide, how to provide that information, how to facilitate interruptions and how to allocate control of the information’. 4
Awareness levels
Awareness levels provide a measure of cooperation in the context of Cooperative Management. Hence we can say that the level of cooperation will be best if the humans involved have the right level of awareness. Typically awareness is supported through information and communication technologies, including various types of communication technologies (e.g. videoconference) and information processing tools (e.g. intelligent agents). Support for mobility adds a new dimension in supporting awareness.
Awareness level was the basis of the cooperative management methodology for e-business management and services (CoMENS) proposed by Ray. 5 This methodology has been tested in telecommunications and health care. 4,7
Without mobile e-health support, the interactions between patients and their doctors might take place as in the following scenario:
physiological signals from sensors on the patient's body are transmitted to a monitoring device. After a period of time has elapsed, e.g. a few days, the monitor is handed to the doctor who then analyses the results using a computer; any irregularities may be further escalated to a specialist who consults with the doctor; in the event that the diagnosis is serious, the doctor immediately alerts paramedics to attend to the patient.
The above scenario will work provided the doctor knows quickly about any changes in the patient's condition. This may be feasible in a hospitalized patient, but unlikely if the patient is at home. Hence this scenario has obvious problems in the case of patients suffering from chronic illnesses. As shown in Table 2, cooperation is not adequate because the levels of Awareness Levels Supported (ALS) in these interactions are different from Awareness Levels Needed (ALN) in the management of chronic illnesses.
Awareness levels in chronic illness. The interaction number is shown in column 1 (and the two involved roles connected by an arrow as shown in Figure 1). For example, in interactions 1 and 6, the doctor role needs a higher awareness level (4) than the awareness level supported (3)
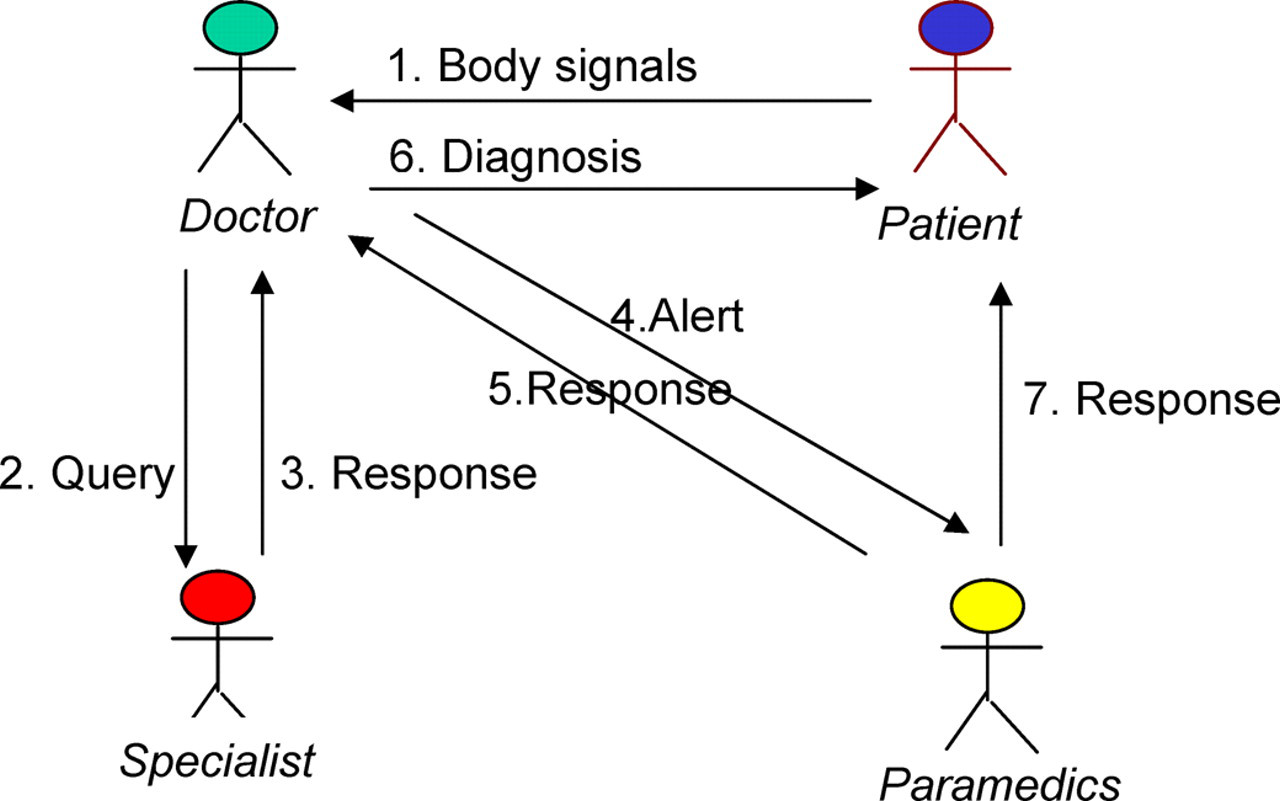
Remote patient health monitoring. The steps depicted are: (1) electronic monitoring devices send body signal data to the doctor; (2) the doctor interprets the data, generates a query and sends it to a specialist; (3) the specialist responds with a recommendation to the doctor; the doctor sends an alert for an action to the paramedics; (4) the paramedics respond to the alert; (5) the doctor sends the diagnostic details to the patient; (6) finally the paramedics send advice to the patient or visit the patient
ALN and ALS have two values corresponding to the interactions concerned. For example, interactions 1,6 are initiated from patient to doctor. Hence ALN = 1,4 signifies ALN = 1 for patient and ALN = 4 for the doctor. Thus ALN and ALS are different for all roles in all interactions. Hence the design solution will need to make ALS equal ALN in all interactions.
The main problem with chronic illness management lies with the sporadic contacts allowed between a patient and the doctor when the patient is not hospitalized. The patient could die of complications between these contacts and the doctor would not necessarily know. A cooperative management system overcomes the problem with multiple software agents representing different human roles, such as patients, doctors and nurses. 8
Interactions in m-health
The interactions in the scenario shown in Figure 2 occur sequentially as follows:
the patient has their body signals sent via Bluetooth to the patient agent; the patient agent forwards this information to the server agent; the hospital agent performs some processing and analysis and sends the results back to the patient; on comparing the patient's health history, the agent detects an abnormal pattern and alerts the doctor; the doctor formulates a query to ask regarding the problem; the server agent informs the correct specialist agent; the specialist receives the query; the specialist responds to the query; the answer is forwarded to the server agent; the answer is received by the doctor; a response is sent to the server to notify the agent of a necessary check-up; the paramedics' agent polls the server for a check-up; the server agent sends out a notification to the paramedics' agent; the notification is noted by the paramedics; the paramedics are able to respond to the situation; the response is forwarded to the server agent; the server agent informs the patient agent that help is arriving; the patient is notified of the diagnosis and the arrival of help; the paramedics reach the patient.
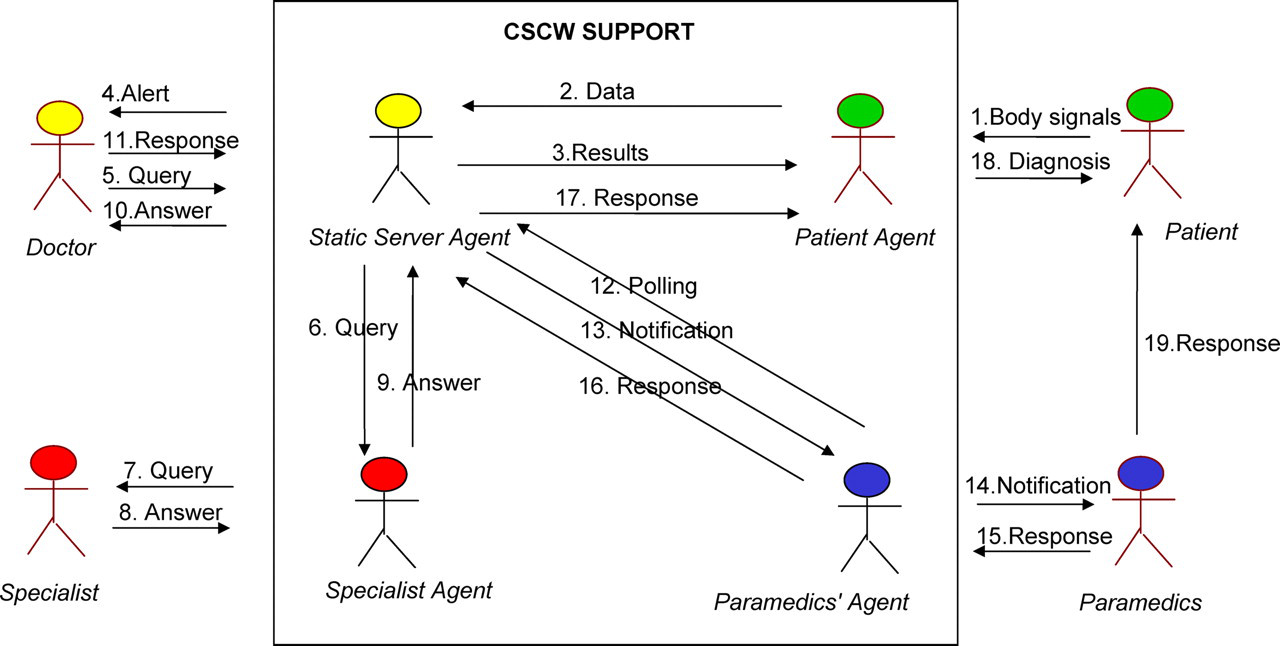
CSCW support provides intelligent agent interfaces for humans to communicate with. The steps depicted are: (1) signals from the patient's body are sent by wireless devices to the patient agent; (2) the patient agent converts the signals into data form and forwards the data to the server agent (representing the doctor, but implemented at a central server); (3) the server agent analyses the data and sends preliminary results to the patient agent; (4) the server agent also sends an alert to the doctor; (5) the doctor examines the alert and forms a query to the specialist; (6) the query is forwarded to the specialist agent; (7) the query is then forwarded to the specialist; the specialist examines the query and prepares an answer; (8) the specialist's answer is forwarded to the server agent; (9) the answer is then forwarded to the doctor; (10) the doctor's response is sent to the server agent; (11) the paramedics' agent keeps polling the server agent; (12) the server agent sends a notification upon receiving the response from the doctor; (13) the notification is forwarded to the paramedics for action; (14) the paramedics return a response; (15) the response is forwarded to the server agent; (16) the response is then forwarded to the patient agent; (17) the patient agent then sends a predefined diagnostic procedure to the patient to follow; (18) the patient in the meantime receives the paramedics' response
In traditional medical practice many of these activities would involve appointments and face-to-face meetings between the patient and the physician. In the scenario described here, the whole process is automated. Hence this process would be much faster than traditional modes of doctor–patient interaction that need to wait for the availability of the physician and other staff. Any routine checks can be performed by agents, freeing up the time of the health-care personnel involved to focus on more serious situations. Besides, coordination between health-care personnel can now be done via the cooperative management infrastructure using mobile e-health.
CSCW awareness matrix
As mentioned above, an awareness level can be used to determine the level of cooperation among agent and user participation. The event flows are listed in Table 3, which specifies for each one the previous and new communication mechanism used, as well as the associated awareness levels.
Awareness matrix
Mobile e-health can therefore help to achieve cooperation by providing the right awareness levels at the right time. The new awareness levels allow health professionals to provide patient care with better quality and efficiency. 9 Mobile e-health systems could take over the mundane tasks of the doctor so that better quality health services can be provided.
Future work
A CSCW-based awareness model for integrating mobile wireless technologies could improve health care for people all over the world, especially in remote communities. This is significant because mobile wireless technology is expected to play a major role in delivering health-care services to homes in the context of the ageing population of many countries. The proposed awareness model provides a framework for designing e-health systems and software for mobile e-health in a collaborative context. A methodology (CoMENS) based on this model has shown promise in a number of business sectors including health care. 4,7