
Abstract
We simulated a cardiopulmonary resuscitation (CPR) scene with a manikin and used two 3G videophones on the caller's side to transmit video to a laptop PC. Five observers (two doctors with experience in emergency medicine and three paramedics) evaluated the video. They judged whether the manikin was breathing and whether they would give advice for CPR; they also graded the confidence of their decision-making. Breathing was only visible from certain orientations of the videophones, at distances below 150 cm with good illumination and a still background. Since the phones produced a degradation in colours and shadows, detection of breathing mainly depended on moving contours. Low camera positioning produced better results than having the camera high up. Darkness, shaking of the camera and a moving background made detection of breathing almost impossible. The video from the two 3G videophones that were tested was of sufficient quality for telephone CPR provided that camera orientation, distance, illumination and background were carefully chosen. Thus it seems possible to use 3G videophones for emergency calls involving CPR. However, further studies on the required video quality in different scenarios are necessary.
Introduction
In the last few years, digital cameras have been integrated into mobile phones, the Universal Mobile Telecommunications System (UMTS) has been introduced and the availability of third generation (3G) mobile phones mean that video telephony is now possible for most people in industrialized countries. The question therefore arises how such videophones could be used for emergency calls.
Sudden cardiac death is a medical emergency, which requires treatment by cardiopulmonary resuscitation (CPR) within a few minutes. 1 Unfortunately survival rates are low (5–10%). 2 Survival decreases by 7–10% for each minute that CPR is not provided. 3 The rate of bystander CPR is very low, 4 so emergency call centres have attempted to increase bystander CPR by giving advice to the caller via telephone. This is called ‘telephone CPR’.
Telephone CPR increased the number of bystander CPR attempts, but different studies showed that it took too long for CPR to be provided. 5–7 The need for CPR was often not identified by the dispatcher or the caller, 6,8 and mistakes made by the caller were not detected by the dispatcher. Many of these problems were due to the limitation that there was only an audio connection between the caller and the dispatcher. After the availability of videotelephony via mobile phones, there was interest in their potential for telephone CPR.
Unfortunately, 3G videophones still have a very poor video quality. They use Quarter Common Intermediate Format resolution (176 × 144 pixels) and a frame rate of 5–15 frames per second due to the limited network bandwidth (64 kbit/s for video). The present study was designed to find out if this video quality was suitable for telephone CPR and how 3G videophones should be used to get the best results.
Methods
We simulated a CPR situation with the manikin and established a video call to a simulated emergency centre. A 3G videophone was connected to a laptop computer via a UMTS wireless card. The videos of the emergency calls were recorded on the laptop's hard disk for later review. The video recordings were shown to five observers (two doctors, three paramedics).
The variable of interest was breathing, since this is important for the decision whether to start CPR. Checking of breathing became even more important after checking the pulse was omitted from resuscitation guidelines in 2005. 2 We investigated breathing while changing orientation of the camera, distance and height. We also changed the tidal volumes and circumstances, while keeping the camera orientation unchanged. Finally we changed the illumination, background and the type of the camera.
The medical professionals were told to look at breathing and give their opinion about whether they would give the advice to start CPR or not. They were reminded to think of the importance of their decision and that it might be better to start CPR if they were in doubt.
We also asked them to rate their confidence in the decision on a five-point scale:
extremely sure, would not wish a better video quality; sure decision and would also be able to distinguish between sufficient and insufficient breathing; sure decision but would not be able to distinguish between sufficient and insufficient breathing; decision was possible but very close to guessing; decision impossible.
A standard resuscitation manikin was used (Rescue Anne Manikin, Laerdal Medical AS, Trondheim, Norway) as the patient and a SV900D respirator (Siemens-Elema AB, Solna, Sweden) for the simulation of breathing. The 3G videophones used by the caller were the N90 and the N93 UMTS videophones (Nokia Corporation, Helsinki, Finland). The N90 has one built-in camera and the N93 has two cameras. To simulate the dispatcher's side we used a laptop computer (TravelMate 8204WLMi, Acer Incorporated, Hsichih, Taiwan) with an integrated camera and a UMTS card (E620 PCMCIA, Huawei Technologies Co. Ltd, Shenzhen, China). For receiving video calls on the laptop we used the software VT-Phone version 1.2.2.008 (Dilithium Inc., Petaluma, USA). For recordings of the video calls for later evaluation we used BulentScreenRecorder 3.2 software (BSRSoft). The videos were shown to the evaluators with the K-Lite Codec Pack Media Player Classic version 6.4.9.0.
Design of experiments
Five experiments were conducted:
Experiment A: The breathing volume was kept constant, and the camera position was changed using three different heights, eight distances and five orientations. The heights of 140, 60 and 0 (ground level) cm simulated the mobile phone in the hand of a standing person, a kneeling person or the phone lying on the ground, respectively. We used distances of 20, 30, 50, 100, 150, 200, 250 and 300 cm. Five orientations were tested: (1) view from the head; (2) view 45° from the head; (3) view 90° from the side; (4) view 45° from the feet; and (5) view from the feet. All recordings in experiment A were done with a tidal volume of 500 ml, since this is usual for normal breathing. We used a ventilation frequency of 10 /min. Videos were recorded with and without ventilation. The recording time for each video was 30 s since a decision to start CPR should not take longer.
Experiment B: The camera position was kept unchanged, while we used different tidal volumes (100, 200, 300, 400, 500, 600, 700, 800, 900 and 1000 ml). We used three different cameras and three different light levels: (1) full light: light in the room dimmed to maximum intensity; and (2) low light: light in the room dimmed to minimum intensity; and (3) no light: light in the room switched off, with some poor light from outside.
Experiment C: The tidal volumes from experiment B were used, while the background was changed: (1) white background; (2) green background; and (3) moving background. For the white and green background different wallpapers were used. To obtain a moving background we filmed an outside street scene with moving cars and projected the video on the wall with a data projector.
Experiment D: The tidal volumes from experiment B were used, while the camera was shaken.
Experiment E: The tidal volumes from experiment B were used with a new camera position. The camera was placed on the abdomen of the patient.
Results
Experiment A
All evaluators were able to detect breathing from 20 cm distance up to 100 and even 150 cm distance in some cases, if the camera was orientated from the shoulder, side or pelvis at ground level or at 60 cm height (Figure 1). Other positions did not have a 100% detection rate, even at short distances. At 200 cm distance, the detecton rate was below 50% in most cases. The positions from the head and from the feet produced the worst results for short distances.

Experiment A, N90 phone with ventilation on
Experiment B
All evaluators were able to detect breathing at a minimum of 500 ml tidal volume with the N90 phone in a good light (Figure 2). For the high quality camera of the N93 and the low quality camera of the N93, 100% detection rate was possible at a tidal volume of 300 ml. In bad light conditions there was no situation where all the evaluators could detect breathing with the N90, while it was possible from 800 ml of tidal volume for the N93 camera.

Experiment B, at different illumination levels with different phones
Experiment C
With a white background, all evaluators judged correctly from 500 ml tidal volume (Figure 3). With a green background, all evaluators judged correctly even at a tidal volume of 300 ml. With a moving background there was no tidal volume where all evaluators assessed correctly. The majority was able to detect breathing at a tidal volume of 800 ml.
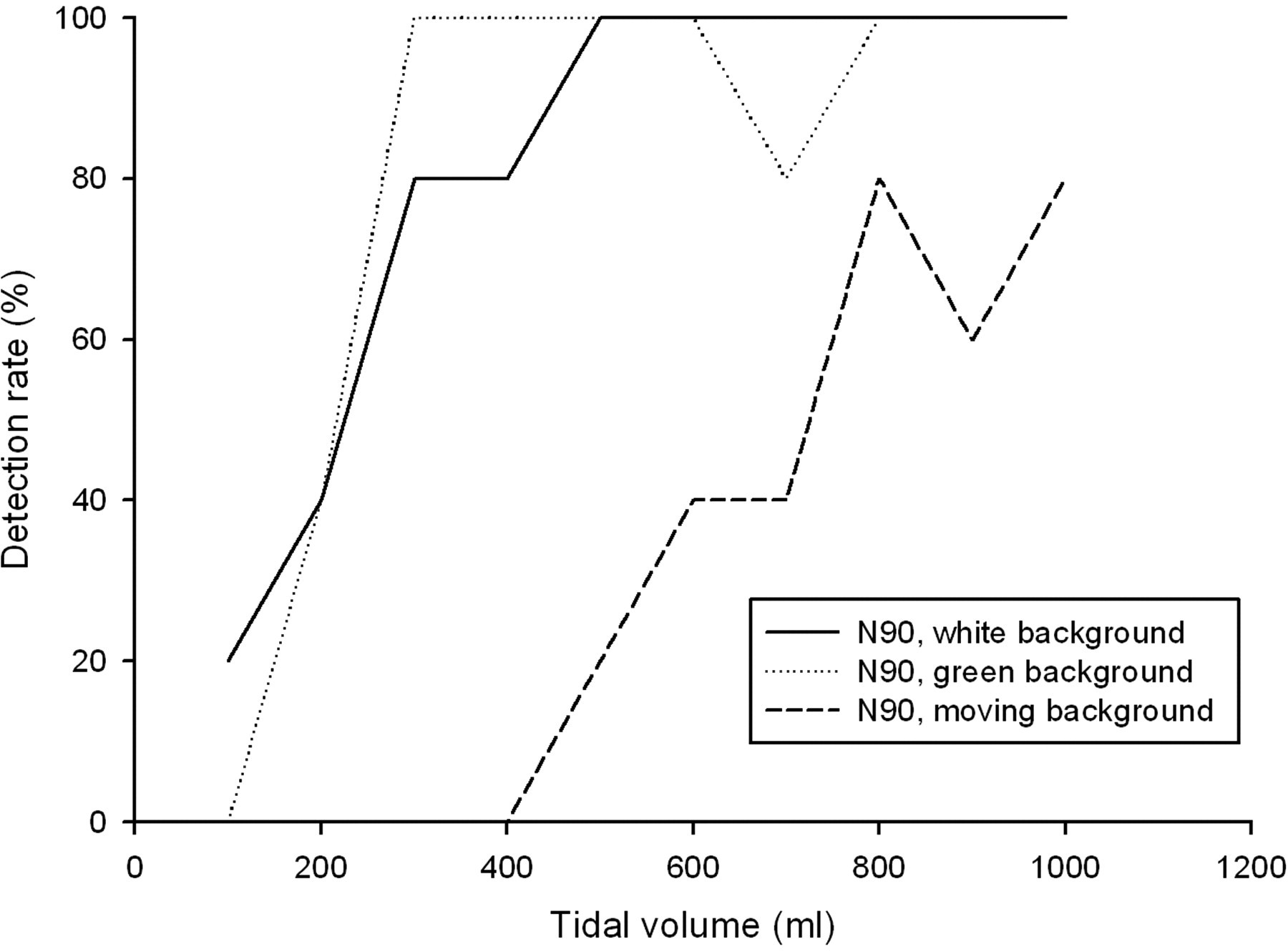
Experiment C, using different backgrounds
Experiment D
With the fixed camera, tidal volumes of 500 ml were detectable by all evaluators (Figure 4). For freehand use of the camera, tidal volumes of 800 ml were necessary. With an actively shaken camera, the majority of the evaluators were not able to detect breathing.
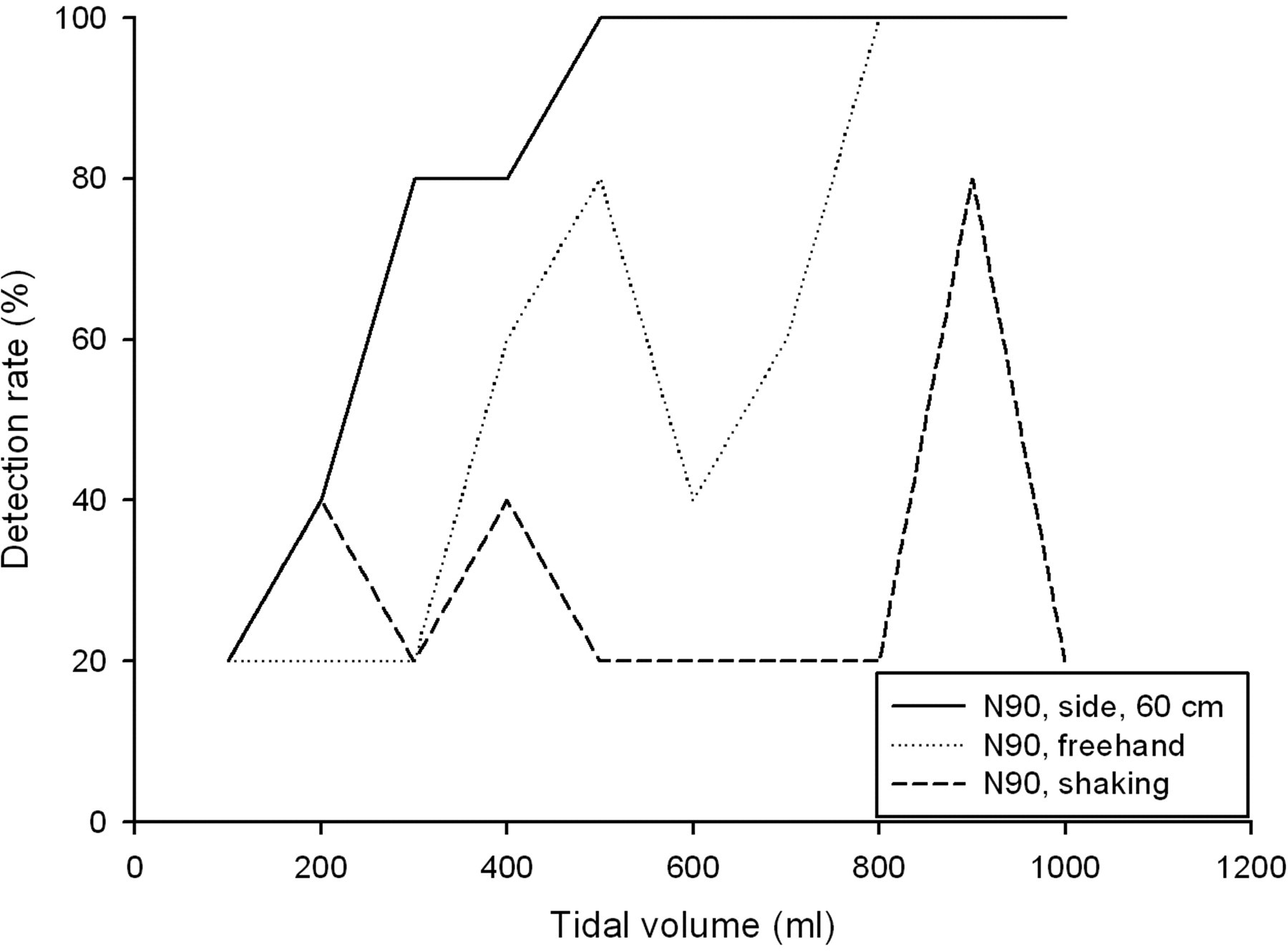
Experiment D, with and without camera-shake
Experiment E
If the camera was placed on the abdomen, all evaluators were able to detect breathing even at low light levels from 200 or 300 ml (Figure 5). If the camera was placed at the side of the patient, a tidal volume of 500 ml was needed for 100% detection rate. At lower light levels, 700 ml were needed to obtain detection rates above 50%. One hundred percent were not reached at that position.
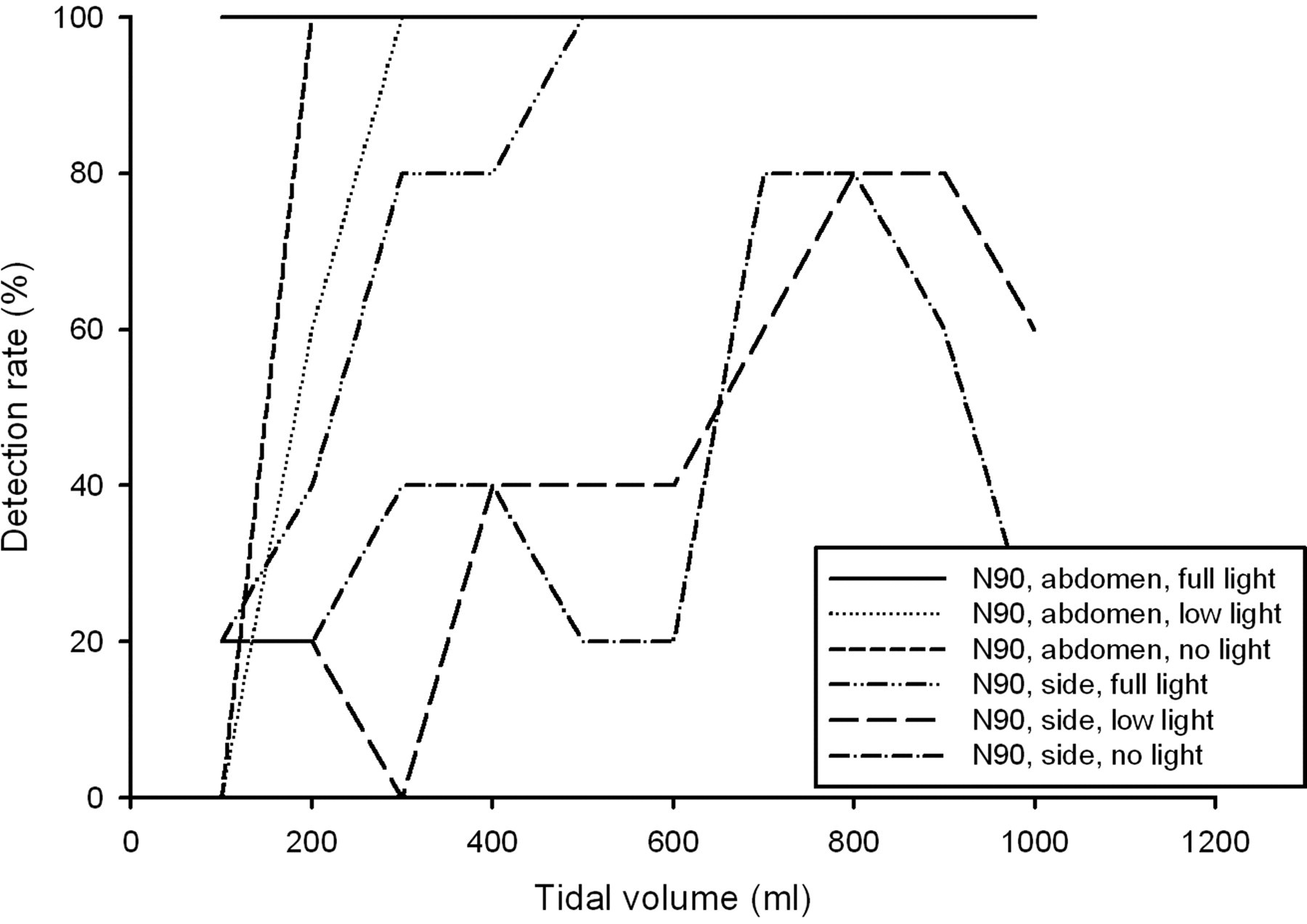
Experiment E, with camera on the abdomen and at the side
Discussion
In the present study it was obvious that the video quality of the 3G phones tested was poor. This is not surprising due to the low resolution. Nonetheless it was possible to see breathing under some conditions.
The video recordings were examined carefully to find out why there were some positions with better results. In experiment A, the position with the camera from the head at ground level had disadvantages because the head was in front of the chest and made chest movements almost invisible (Figure 6). Camera positions with a height of 140 cm had disadvantages compared to the lower positions. While it was possible to watch moving contours at low heights, changes in colours and shades have to be used to detect breathing from higher positions. Since the 3G phones have poor colour performance, these views have a disadvantage.
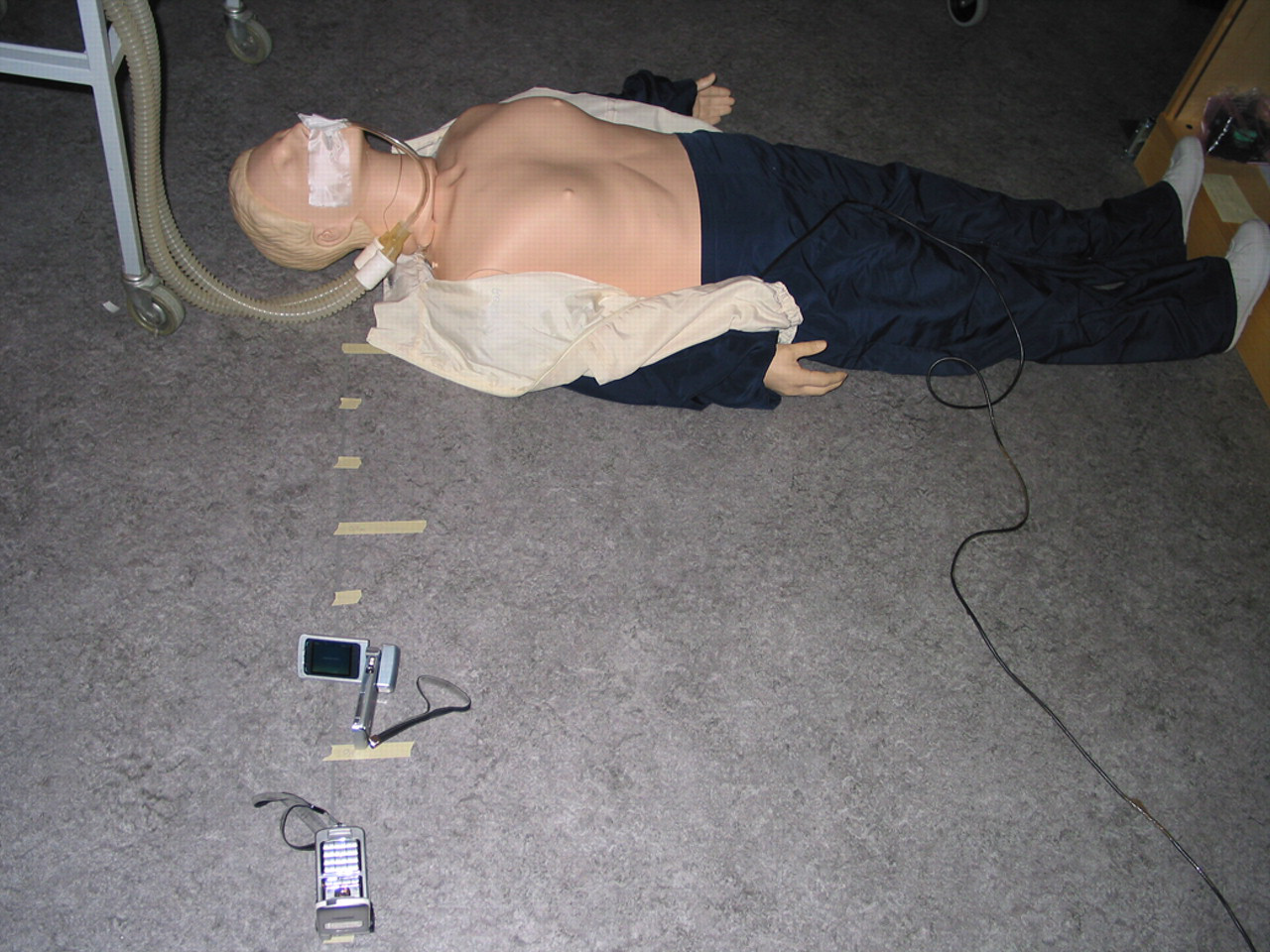
3G phone being used at ground level
In experiment B the bad results at low light levels seemed to be due to noise in the pictures. While it was still possible to see the lying person even at low light levels, the detection of breathing was very hard because noise in the pictures could not be discerned from breathing movements.
The green background in experiment C had an advantage compared to the white background because it produced higher contrast with the white skin of the manikin, and moving contours could be detected more easily. The moving background produced the worst results since the compression algorithm decreased the picture quality, especially in situations with much movement. Block sizes became so big that it was impossible to see small breathing movements.
Since it was necessary to observe movements amounting to a few pixels in the pictures in order to detect moving contours, freehand camera use or active shaking made it impossible to identify small movements in experiment D.
In experiment E the position of the camera on the abdomen of the manikin had advantages, especially at low light levels. This was caused by the short distance to the rising chest, so even a small chest movement represented a big movement in terms of camera pixels.
Conclusion
Use of 3G videophones appears to be a promising method of improving the quality of CPR. Their video quality is good enough for use in telephone CPR under the best circumstances, but conditions have to be checked carefully. If conditions are good, even very small tidal volumes of 300 ml are detectable by most evaluators and tidal volumes of 500 ml are detectable by all evaluators. The present study also showed that camera orientation, illumination, shaking and background movements can influence the video quality so much that the reliability of the results is limited if the circumstances are not ideal.
There were some differences in the detection rate between the different cameras of our two videophones. Further work on how other new videophones behave, especially at low illumination intensity, is required.
We discovered other factors for the usability of 3G videophones which should be considered. It seemed to be practical to use the inside camera of a flip-phone, since it was easier to place it in a good viewing position. The colour perception of some 3G videophones is so bad that the cameras cannot give a realistic impression of the patient's skin colour and could lead to misinterpretation when making a diagnosis. Further studies about the importance of colour perception for telemedicine are required.
According to our results we would recommend a camera position with a distance between 50 cm and one meter and an orientation from the side or shoulder at low heights (Figure 6). As well as a better detection rate, these orientations also have the advantage that other important parts of the CPR like the chin-lift manoeuvre may also be observable. Placing the camera on a fixed item should be favoured since shaking caused worse results in our tests. If there is doubt whether the subject is breathing, the best position in our tests was with the camera placed on the abdomen of the person.
Despite these limiting factors, it should be kept in mind that it is the CPR which is most important and not the video quality. The caller should not be put under too much stress with handling a mobile phone in this situation. The caller should concentrate on the CPR itself. Even if breathing is not detectable under bad conditions any additional information that is given by video telephony could be an advantage for CPR. Other information in the video about what is going on might also help the dispatcher to provide additional advice.
In summary, it seems possible to use 3G videophones for emergency calls involving CPR. However, further studies on the required video quality in different scenarios are necessary.
Footnotes
Acknowledgements
We thank Gunnar Hartvigsen, Stein Roald Bolle, Eli Arild, Elisabeth Ellefsen Sjaaeng, Jeremiah Scholl, Per Hasvold, Terje Solvoll, Alexander Schmidt, Sebastian Ruhdorfer, Martin Bretschneider, Matthias Feuerecker, Karl Acker, Dilithium Networks and thesilver.net for making our experiments possible.