
Abstract

Videoconferencing is a well known modality for health-care delivery. However, little quantitative information has been published about videoconferencing usage by health-care professionals in Scotland and technically it is difficult to gather such data. Nonetheless, this type of information is of great interest to NHS managers and health economists, in the light of the new NHS performance targets 1 (HEAT, Health improvement, Efficiency, Access and Treatment). For example, patients being managed by videoconferencing may not have to travel. This is likely to provide efficiency gains, as in Scotland some patients may have to travel long distances, which may also necessitate an overnight stay away from home. There are additional environmental benefits of not having to travel, such as the avoided carbon dioxide emissions.
We have developed a simple web-based questionnaire to assess videoconferencing usage among health-care professionals in Scotland. We distributed it by email to a convenience sample of 125 doctors known to use videoconferencing. A total of 45 (36%) responded. We did not attempt to contact the non-responders.
Almost half of the responders were hospital doctors, about one-quarter were GPs and about one-quarter were other allied health professionals involved in videoconferencing health-care delivery (see Figure 1). All responders to the questionnaire were based in Scotland: there were 40% from the main teaching hospital in Aberdeen, 12% from district general hospitals in Scotland, 12% from Minor Injury Units in the north-east and the remainder from primary care settings.
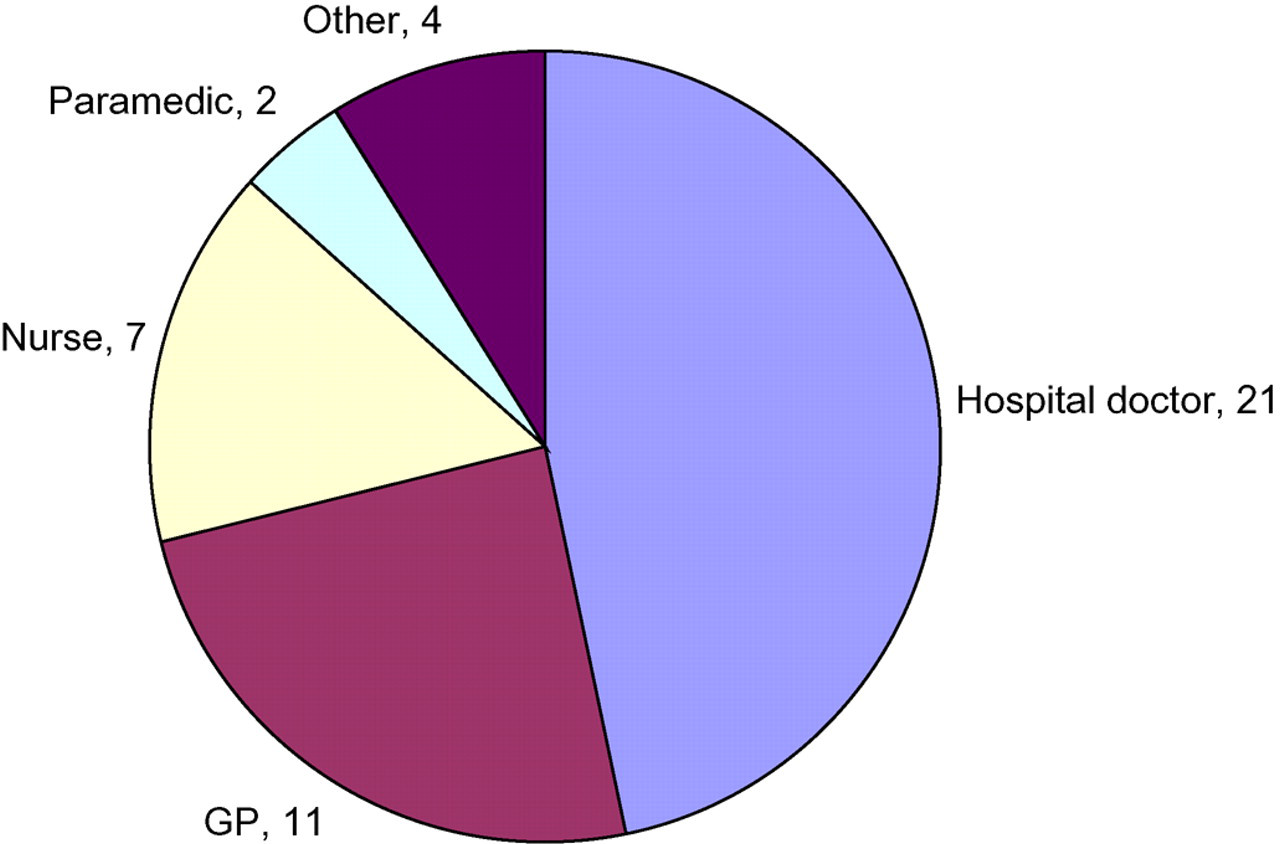
Respondents' jobs (n = 45)
The responders were asked to estimate how often they took part in a videoconference: the median value reported was 1 per month (interquartile range, IQR 1–3). They were also asked to specify when they last took part in a videoconference. Thirty respondents provided a reply, and the median interval since their last videoconference was 21 days (IQR 2–29). That is, the median frequency with which the respondents reported participating in videoconferences was 18 times per year.
The most common use of videoconferencing was reported to be clinical service delivery (35%). 28% of respondents used it for administrative meetings and 23% used it for education, while 15% did not specify a particular use.
The questionnaire asked respondents to score their general experience of videoconferencing in Scotland, using a Likert scale (1 = very poor to 5 = very good). The median response was 4 (see Table 1). The majority (67%) felt that their general experience of videoconferencing usage in Scotland was either good or very good; no one felt that the experience was very poor (i.e. to be avoided at all costs).
General experience of videoconferencing (n = 42)
Finally, we asked what could be done to improve videoconferencing in the future or encourage more frequent use. The main themes that were mentioned were:
Technical (21 respondents); Accessibility for all (10); Educational, e.g. videoconferencing etiquette/chairing meetings, how to use systems, spreading the word to non users (20); Universal/standardising equipment across Scotland (5).
Email surveys of this sort appear to be a relatively easy method of obtaining quantitative information about videoconferencing usage from practitioners. It was reassuring that the two estimates of the average rate of videoconferencing made by the respondents appeared to be internally consistent. Our best estimate of the videoconferencing activities of the 45 respondents therefore is that about two-thirds of them were participating in videoconferencing on approximately 18 occasions per year. To turn this figure into an estimated network load for the Scottish NHS as a whole requires some further work, but an email survey appears to be a promising approach.