
Abstract
Summary
We reviewed the literature on home telecare for elderly patients suffering from chronic diseases. Articles published between 1990 and 2007 were identified via the PubMed database. The literature search yielded 485 papers. After reviewing the title and abstract from each, 54 were selected for closer examination. They were published in 37 different journals. The number of papers increased from one in 1997 to 14 in 2006. The diseases in which home telecare had been used were diabetes (14 studies), heart failure (13 studies), cognitive impairment (dementia and/or Alzheimer's disease, 10 studies), chronic obstructive pulmonary disease (5 studies), chronic wounds (4 studies) and mobility disabilities (4 studies). Patients were generally satisfied with home telecare, but they preferred a combination of home telecare with conventional health-care delivery. Health-care professionals were positive about telecare. Users felt that on many occasions telecare led to a reduction in costs due to time savings and avoidance of travelling. Even though there were important benefits from home telecare, there are organizational, ethical, legal, design, usability and other matters that need to be resolved before widespread implementation can occur.
Introduction
The need for health care increases with age – four times as many people aged 85 years and over need daily care compared to those aged 65–74 years. 1 At the same time, it is unlikely that in the near future there will be enough nurses 2 or other health-care staff to provide adequate care. It is also possible that there will be a lack of facilities to accommodate them. The situation where neither health-care staff nor nursing homes are available is common all over the world. 3
The demanding task of elderly health care, especially for those suffering from chronic diseases, cannot be solved solely by conventional methods; other alternatives and more cost-effective technical solutions must be considered. Calculations in the US show that the ratio between the care in a person's home and the care in a nursing home is 1:25 in favour of the person's home. 4 Telemedicine in the home environment is usually described as home telehealth, 5 home-based e-health 6 or telehomecare. 7
Home telecare systems have been developed for elderly patients suffering from disabilities or chronic diseases such as heart failure, diabetes, asthma and chronic obstructive pulmonary disease (COPD). 8 Home telecare aims to increase an elderly patient's independence and quality of life, and produce cost savings for the authorities. We have reviewed the field.
Methods
We searched the PubMed database (1990–August 2007) for all relevant publications using the following search terms: {[elderly] AND [(telemedicine OR telehomecare OR telecare OR telehealth OR mobile information system OR remote health OR telemonitoring OR ehealth)] AND [(chronic disease OR diabetes OR dementia OR disorders OR COPD OR mobility OR disabilities OR heart failure OR wound OR cardiovascular OR renal OR impairment OR asthma)]}.
Papers were included if they appeared in peer-reviewed journals and/or reviewed international conference proceedings. Reports, non-reviewed journals, book chapters, newspapers and websites were not included in the review. All the abstracts of the papers were read by the two authors, who acted as independent reviewers, to decide if they were relevant.
The inclusion criteria were:
a home telecare system or methodology developed explicitly for elderly patients suffering from a chronic disease; a research project that tested the combination of home telecare with traditional health-care methods for chronically diseased elderly people; a qualitative study that evaluated aspects such as users' acceptance, legal and ethical issues; a comparative study with telecare and traditional home care or other approaches. simulation and theoretical models; distance care not utilizing home telecare technology or health-care support only via the ordinary telephone; distribution of information via the Internet; systems and methods developed for chronically diseased patients but not targeted at the elderly; home telecare systems that did not involve patients, e.g. teleconsultations between physicians with no patient present; home telecare systems for the elderly recovering from an acute condition, e.g. postoperative patients.
The exclusion criteria were:
When several publications were derived from the same research project, only the publication with the most recent results was included. The literature search was not language restricted.
Results
The literature search yielded 485 potentially relevant papers. After reviewing the title and abstract from each, 54 were selected for closer examination (Figure 1).

Selection process for the papers reviewed
Publication data
None of the selected publications appeared in conference proceedings, only in scientific journals. They were published in 37 different journals. The impact factors of these journals (n = 20) were 0.37 to 8.25. Ten articles (18%) were published in the Journal of Telemedicine and Telecare and seven (13%) in the Telemedicine Journal and E-health; four other journals had two papers published each (Table 1). In addition, four papers appeared in the IEEE Transactions series (two more IEEE Transactions journals that are not included in Table 1 published one paper each) and the rest were spread over a variety of other journals, mainly medical. The Journal of Telemedicine and Telecare had the first paper published in 1997.
Journals with at least two relevant publications
The number of papers increased from one in 1997 to 14 in 2006 (Figure 2). The majority of papers were produced in the US (n = 34) and Europe (n = 10). Third place was shared by Australia and Canada (n = 3). China, Korea and Taiwan produced four papers. Japan did not produce any publications, probably due to the fact that some studies appeared only in Japanese journals which were not indexed in PubMed. Sweden led the scientific publications in Europe (n = 2) and Germany published the first study in 1997.
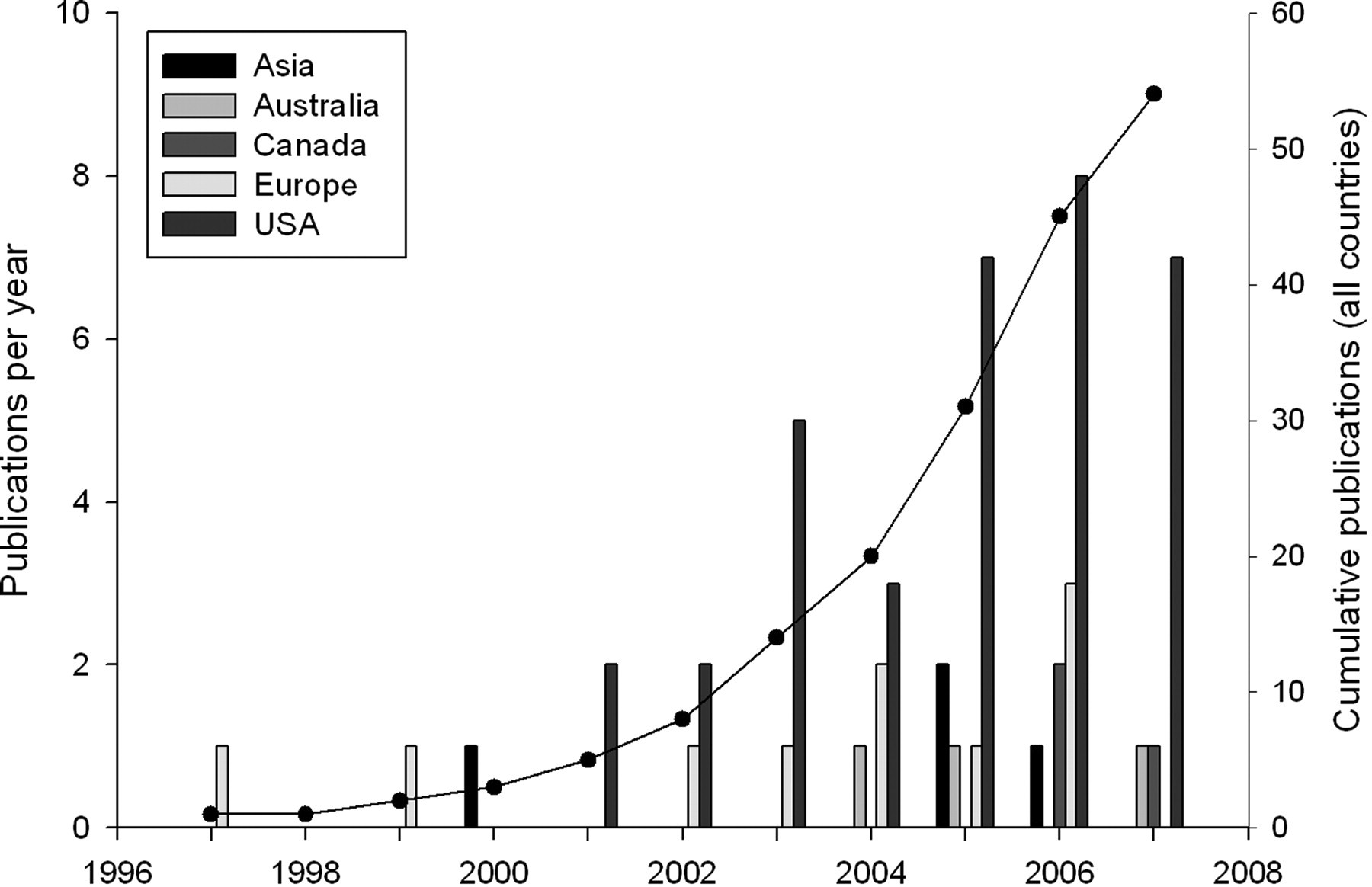
Publication rates in five regions
The articles were categorized as:
system description: any novel system that was developed for elderly suffering from chronic diseases; research studies: application of existing telemedicine applications or off-the-shelf products for home telecare of the elderly; comparative studies: comparison with traditional approaches, including clinical trials; qualitative studies: focus on user's acceptance, ethical considerations, potential role of systems; reviews.
Most of the reports belonged to the second category (24 publications). There were 12 comparative and seven qualitative studies. There were six papers about new systems development. There were five reviews that only partly covered the field.
Publication content
The diseases that had been studied were mainly diabetes (14 studies), heart failure (13 studies), cognitive impairments (dementia and/or Alzheimer's disease – 10 studies), COPD (5 studies), chronic wounds (4 studies) and mobility disabilities (4 studies) (Table 2). Some papers dealt with more than one disease or with disabilities in general.
Study details and main findings
SD, system description; RS, research study; CS, comparative study; QS, qualitative study; R, review; IG, intervention group; CG, control group; NS, not specified
*Number of users (patients [unless stated as caregivers, relatives and or healthy subjects]) involved in the study; patients categorized according to disease when specified
The majority of publications reported the use of telecommunication devices for assessing the physical 9–25 and/or cognitive 26–31 condition of a patient. They employed videoconference, 10–13,26–31 audio-visual 14–17 and telehealth communication units 18–25 for virtual visits. During these virtual visits the patient was supported, educated on topics related to their status and consulted for the better management of their disease. In some cases, these activities were combined with traditional home health caring strategies. 30,31 Teleconsultations between the nurse specialists located at a veterans clinic and a multidisciplinary wound care team were also reported. 9
The second large category dealt with telemonitoring. 32–47 The information transmitted was physiological data such as vital signs, ECGs and symptoms. This was sent to a central repository via the Internet or a conventional telephone line. 35–41 The patient's position (indoors and outdoors) was monitored using various technologies such as positioning devices with Radio Frequency Identification (RFID) tags, 42 remote video cameras, 43 e-textiles 44 or sensors. 45,46 One study described a complex renal support system. 47
A number of evaluation studies were published on topics such as the technical quality of the home telecare equipment, 48,49 user satisfaction and acceptance, 50–54 the ethical issues and psychosocial outcomes 55 and the cost of the services. 56 The remaining publications reviewed smart homes 57,58 and other telemedicine technologies 59 for elderly people with disabilities. Two recent papers described telesurveillance 60 and a robotic personal aid. 61
Ní Scanaill et al. 45 reviewed systems for elderly telemonitoring. These technologies were used in many studies as shown in Table 2.
Findings
Each paper presented findings that could be classified into three thematic categories: (1) patients and health-care professionals; (2) effects on chronic diseases; and (3) cost aspects.
Patients and health-care professionals
The main problem in monitoring patients at home was their ability to use the equipment provided. Usually, they failed to respond to the establishment of a videoconference session after it was initiated from the centre 32 or transmit their data successfully. 30 In particular, home telecare was not always found to be user-friendly for people who had middle-stage Alzheimer's disease because they had difficulties in learning a new task, or how to use the telemedicine device. 14 On the other hand, veterans in another study who were suffering from non-cognitive diseases (hypertension, heart failure, emphysema, coronary artery disease and diabetes) reported that the technology was easy to use and helpful in managing their chronic conditions. 51 In a third study, patients with COPD or chronic heart failure felt comfortable with the videoconference and the other peripheral devices they used. 35
Patient satisfaction varied between studies and was related to the result of their treatment. Wilkins et al. 9 indicated that 98% of patients were satisfied when using a web-based teleconsultation system for the care of their chronic wounds. In another study the patients felt more secure and had a perception of efficiency and effectiveness from their daily assessment. They also expressed great satisfaction when they received better information on their health status. 36 In addition, the patients reacted positively when they were asked to suggest potential health-care applications or questioned about the participation of robots in their health care. 52 In the earliest study that was reviewed, 17 mobility-impaired elderly patients were connected via a broadband video communication system to a telecare centre from 1991 until 1997 and received a variety of services. The total number of calls was approximately 14,000, indicating the patients' satisfaction. 10
The study by Wilkins et al. demonstrated that not only patients but also referring providers reported a high degree of satisfaction with the system. 9 It also seems that more trustworthy relationships were developed among nurses and doctors who cooperated through a teleconsultation system. 36 In many cases the nurses' knowledge of specific topics was increased as shown in a study by Gardner et al. on wound assessment and treatment using videoconferencing. 18 However, it should be noted that patients and nurses foresee the need for real nurse home visits along with telemedicine ones. 15
Finally, there was a paper describing relatives' positive opinions of IT support in dementia care. 53
Effects on chronic diseases
According to the review by Bowles et al., the addition of home telecare appeared to improve outcomes among patients with chronic diseases, such as heart failure, diabetes and chronic wounds. 62 There was also evidence that home telecare coordination strategies improved functional independence in veterans with chronic diseases. 33
Elderly patients with diabetes had reduced HbA1c values, 19 blood pressure and LDL cholesterol 37 when monitored and educated via telecommunication devices. They also required fewer clinic visits when they were monitored daily via home telehealth, which increased their quality of life. 20 When they were similarly educated regarding diet, symptoms, management of hypoglycaemia, foot care and exercise, they had a better understanding of their status. 11,12 This led to better self-care and lower health risk as shown in the IDEATel study. 55
Shore et al. showed that dementia assessment by videoconferencing did not differ significantly from face-to-face assessment in American Indian veterans; 26 Loh et al. claimed the same in their studies. 27,28 In another study the results were less encouraging. 30 Only one qualitative study found positive results, although the sample was extremely small. 54 In contrast, it seemed that the results were better when a patient was hosted at a nursing home and the nurses used a telemedicine system for teleconsultation. 31 Finally, the use of technologies for locating elderly people with dementia appears promising. 42
Exercise training of elderly people with chronic heart failure in a telemedicine-supervised programme improved their oxygen consumption and their quality of life. 38 There was also a significant improvement in blood pressure, weight and shortness of breath, but also in the average daily doses of medication. 21 An earlier study in the same disease suggested that a disease management programme through a telehealth device could be as effective as traditional methods. 22
Another chronic disease in the elderly that gained benefit from home telecare was chronic wounds, e.g. pressure, foot or venous stasis ulcers. Kim et al. 48 suggested that a relatively inexpensive store-and-forward telemedicine system for monitoring the status of chronic wounds had the potential to improve access to specialty care for patients who were not receiving routine monitoring by specialized nurses or doctors.
Cost
Users felt that on many occasions home telecare led to a reduction in costs due to time savings and avoidance of travelling. 13 A care coordination/home-telehealth programme for veterans with diabetes produced a significant reduction in the proportion of patients who were hospitalized (50% reduction). 16 The reduction in hospitalizations has also been shown in other studies as well 16,19–21,23,24,39,40,51 and is the motivation for developing new systems. 34 For example, the costly incidents of decompensation in heart failure that led to hospitalization could be avoided, or at least lessened in severity with shorter inpatient times when hospitalization is unavoidable, through the use of a telemonitoring service. 25
Discussion
The present review focused on published studies for elderly people with chronic diseases. Home telecare is a relatively new field and the first paper was published in 1997. However the field seems to have developed rapidly after 2001 (Figure 2). It was also clear that certain chronic diseases are not suitable for home telecare, e.g. those requiring the permanent presence of health-care personnel or life critical monitoring equipment.
A basic limitation in many studies was the small sample size and the short follow-up period. There were studies that involved only ten patients or even fewer. 13,17,46,49,52 This represents a significant problem, especially for those studies that produced interesting results. 27–29,41,43,56
Even though dementia and Alzheimer's disease were investigated, the review showed that there were no significant benefits of home telecare compared to traditional methods. A possible explanation is the difficulty of cognitively-impaired elderly patients learning how to use the necessary equipment. This requires further investigation. According to the review findings, the benefits in other diseases (diabetes, heart failure, chronic wounds) are substantial.
Elderly patients are not entirely familiar with technology, but it seems reasonable to believe that they will be in the near future.
63
In addition, staff members are not always comfortable about using computer-based applications and some can easily be deterred when new technological issues arise.
64
In any case, people have to be trained to use a system taking into account their level of expertise (if any) and the type of disease, especially in the case of cognitive diseases. Generally, home telecare systems should fulfil the following requirements:
be simple to use; operate without interruptions; provide computer security and data confidentiality.
The evidence showed that elderly patients were accepting of technology and enjoyed self-monitoring.
35,51
The frequent assessment through home telecare increased their confidence and sense of security.
22
However, they did not want to lose face-to-face contact immediately and considered the combination of home telecare and in-home visits as the best choice.
15
A variety of technologies were used for home telecare of the elderly (Table 2). Many of the technologies have been used previously for other telemedicine applications. The evaluation showed that there are significant benefits in following validated strategies. But the important question is whether these applications meet the needs of elderly people suffering from chronic diseases adequately. New studies are necessary to investigate their value and limitations, and to evaluate the technological complexity which is necessary. For example, personal aids utilizing robotic systems appear promising, but require further study.
The present review did not identify major ethical or legal concerns. Generally, it was stated that as long as data confidentiality and security were ensured there was no major legal problem. However, an important question is whether there should be a special legal framework for health care administered at a distance. Apparently, the characteristics, limitations and permissions in home telecare should be stated clearly. Also, it is important to have an active and open relationship with the possible ethical problems that such systems imply. As mentioned above, in many studies the patients stated that they did not want to lose completely the ‘warm hands’ of the health-care professionals.
In many studies there were cost reductions in terms of time saving, elimination of travelling expenses and fewer hospitalizations. These reductions balanced the substantial cost of some home telecare devices. Unfortunately, very few countries have consistent reimbursement policies for home telecare services. This is an area that should be further explored, otherwise it will not be possible to implement home telecare applications successfully.
The aforementioned areas (technology, ethical and legal issues, costs) could be defined better through a set of guidelines and standards. The Home Telehealth and Remote Monitoring special interest group of the American Telemedicine Association has focused on this but the target is home telehealth with no distinctions. 65 However, the development of specific guidelines for the delivery of these services to the elderly suffering from chronic diseases is necessary and should be a direction for future research.
Organizational and societal changes, such as cost reduction policies and aging populations, are the main driving forces for the development of home telecare for the elderly suffering from chronic diseases. The findings of the present review indicate that there could be significant benefits from the implementation of such systems. It is suggested that more research be conducted on home telecare and its effects on elderly people suffering from chronic diseases, in order to obtain the evidence required to utilize the techniques in routine health care.
Footnotes
Acknowledgment
This work was carried out during TB's tenure of an ERCIM ‘Alain Bensoussan’ Fellowship.