
Abstract
We surveyed health service providers in Namibia to find out how they used information and communication technologies (ICTs) to deliver health services to their patients. A structured questionnaire was administered to 21 health service providers in two regions of the country (one urban, one rural). There was overwhelming consensus among the health service providers that ICTs were very important, especially for medical services (100%). Ninety-one percent of health service providers viewed ICT as helping them to interact with other providers in other health institutions. The most commonly used ICT was the telephone, which was used in the admission areas of most health institutions (36%); the next most commonly used ICT was the PC (23%). The most commonly used channels for communication with patients were the telephone followed by TV. Some of the problems common to all health institutions in Namibia were poor budgetary resources and lack of basic infrastructure such as electricity or telephone lines. There is a need to promote ICT use for health service delivery and also to stimulate patients to use ICT to access health services and relevant information.
Introduction
The delivery and management of health services to deprived communities and regions in less developed countries is a complex task.
1
The use of information and communication technologies (ICTs) in the health sector can assist in disease surveillance and information provision, and improve planning and policy formulation. In Namibia, it is not clear to what extent health service providers use ICTs for health service delivery. We have therefore investigated this. The objectives were to:
examine how health service providers in Namibia use ICTs to deliver health services to their patients; describe the ICT channels that health service providers use for their internal and external communication with other parties; suggest measures to promote ICT use for health service delivery and also stimulate patients' ICT uptake to enhance access to health services and relevant information.
Methods
Health service providers who were surveyed
A structured questionnaire was administered to the health service providers. The questionnaires aimed to investigate: (1) different kinds of ICTs that were being used to deliver health services to patients; (2) health service provider perceptions about the importance of ICT for health service delivery; (3) ICT applications for internal and external communication with other parties; and (4) constraints on the delivery of ICT-based health services in Namibia, particularly in the Khomas and Oshana regions. The questionnaire included both closed and open-ended questions. The information was collected during face-to-face interviews that lasted for about an hour each.
Secondary data
Secondary data on ICT use in Namibia was acquired from different publications such as journals, white papers and policies related to health service delivery. Namibia's policy on ICT use in different economic sectors was also investigated. In cases where key documents were not easily accessible, government officials from the policy and planning directorate were interviewed. Semi-structured interviews were conducted with the policy directorate of the Ministry of Health and Social Services (MOHSS) to enquire about the policy documents on ICT and to also find out if there were existing government policies affecting health service delivery in Namibia. Secondary data sources from literature review, policy documents and interviews provided supplementary information to that generated from the primary data collection.
Results
ICT use for health service delivery
There was overwhelming consensus among the health service providers that ICTs were very important, especially for medical services (100%) (Figure 1). Both clinical support (91%) and nursing services (91%) ranked second in the services that they perceived as very important for ICT application. However, in general, most (86%) health service providers expressed the view that it was very important to use ICT for health service delivery.
Health service provider perceptions about ICT for health service delivery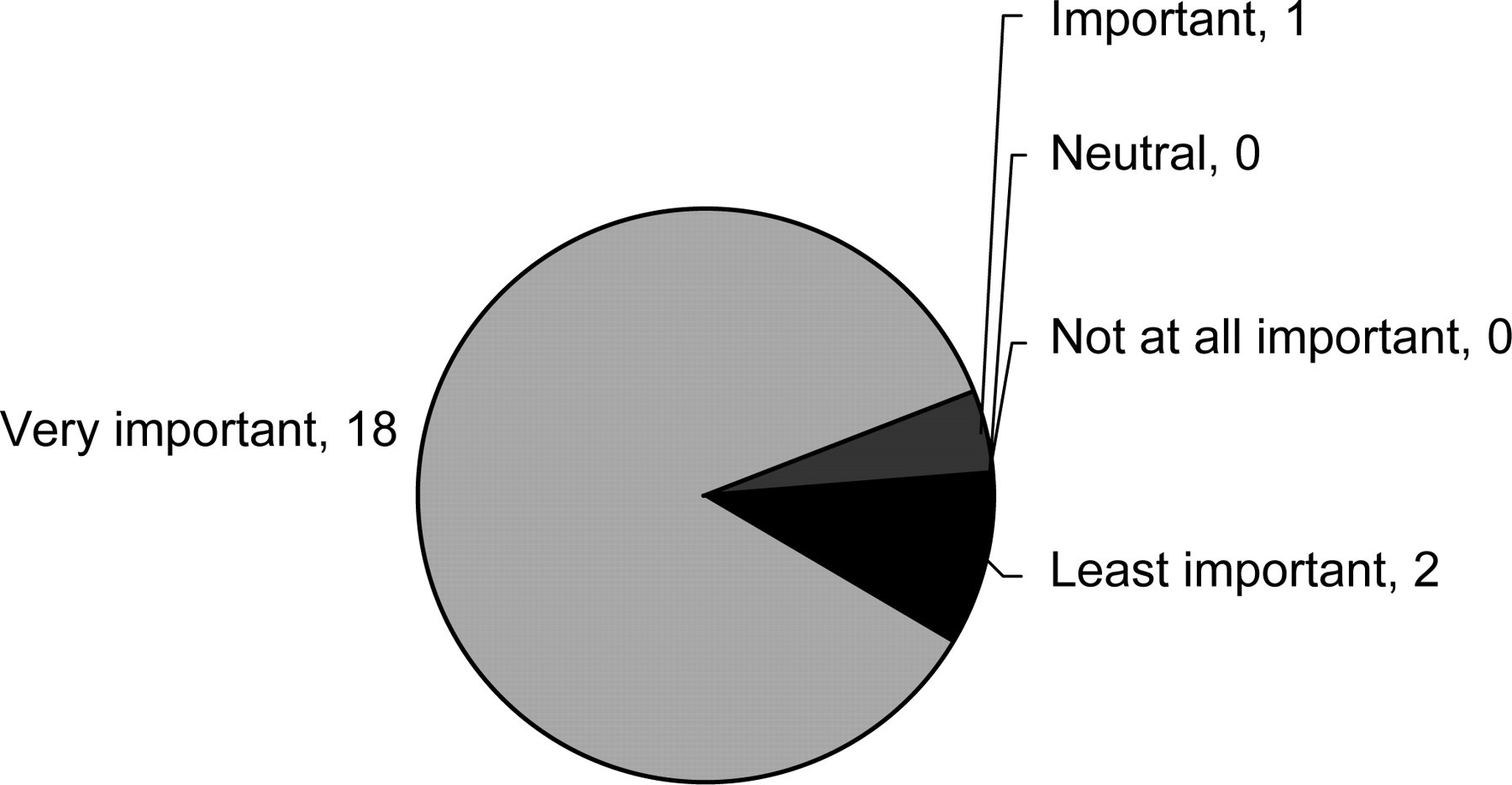
Health service providers had different views about how ICT interventions could make the delivery of health services effective and efficient. Most of them thought that staff needed to be educated first about how to use computers and other technology to enable effective use of ICT tools and to deliver better services to the patients. All health service providers thought that free computer lessons would enhance ICT use, since well trained health workers and personnel would use ICT tools more effectively and efficiently.
Some of the problems common to all health institutions in Namibia were poor budgetary resources and lack of basic infrastructure such as electricity or telephone lines. Most respondents reported that insufficient funds were allocated to provide the necessary investment levels in ICT and in particular to assist in the process of service provision to patients. Additional constraints that were mentioned were lack of technical support, unreliable power supplies, low computer to employee ratios and low priorities for ICT investment. Some of the health institutions in the Oshana region lacked even basic infrastructure such as electricity, and were instead using solar energy at the time of the study.
Health service providers had different opinions about how existing ICT in their institutions had helped them to provide services to patients. There was complete consensus among health service providers that ICT helped them to access new health information. It was observed that the use of computers helped to improve the efficiency and effectiveness of health management information. This mostly applied to departments such as admissions where patient data needed to be captured and stored effectively.
Ninety-one percent of health service providers viewed ICT as helping them to interact with other providers in other health institutions. Eighty-one percent of health service providers strongly agreed that ICT did provide ways to improve health services, even though there were costs involved in the introduction, maintenance and utilization of ICT. More training of staff on ICT use was required to achieve greater effectiveness. Ninety-five percent of health service providers strongly agreed that the government needed to play a more prominent role in the provision of ICT for health service delivery, as they felt that the public sector was lagging behind in ICT use as compared to the private sector. The providers felt that the public sector should learn from the private sector about how ICT could be used in health service delivery to patients.
Areas for ICT use in health service delivery
There was considerable variation in ICT applications across the different functional areas of the health institutions. The most commonly used ICT was the telephone. The telephone was reported as the major ICT used in the admission areas of most health institutions (36%) followed by the PC (23%). For clinical support services, the telephone (86%) and email (23%) were the key ICT channels used for health service provision. In the maternity department, the telephone (36%) and TV (9%) were the most commonly used forms of ICT. Health service providers also mentioned that they used the telephone (27%) and TV (9%) in the family planning departments. The telephone (91%) was also the leading ICT channel used for emergency services and referral services (73%). Fax-based health services were also used in admission and family planning units. Thus the telephone and television were the leading forms of ICT being used across all the functional areas of health institutions surveyed.
Main purposes of ICT use in health institutions
Communication strategies: internal versus external
Health service providers used different communication strategies to interact with patients, other employees, institutions and the higher levels of management. Meetings (32%) were the most commonly used method of communication between health service provider and patients. This specifically referred to health education meetings held between patients and various health facilities. Health education in this context refers to the health service provider conducting one-to-one sessions with either individual patients or a group of patients to present health-related information. The second communication strategy used by health service providers with patients was TV (23%). In this case, patients were shown videos of health-related information on diseases such as HIV/AIDS or TB. The telephone (20%) was also used for communication with the patients in consultation sessions, when setting appointments and during follow-ups by health service providers. It was surprising that health service providers made little use of radio (8%) because it was one of the main communication channels for health information provision as reported by respondents during the patient survey (data reported elsewhere). The reason for this disparity could be that most health programmes and health information services broadcast on the radio are not necessarily initiatives of the MOHSS, but of other non-governmental organizations.
Meetings (43%) were widely used as a communication strategy in major institutions (e.g. reporting of information from low levels to the health institution management). Most institutions mentioned that they held daily, weekly and monthly meetings where matters concerning their health institutions were addressed. The telephone (24%) was used for internal communication with other medical personnel especially in larger health institutions. Health service providers from some smaller health institutions, particularly clinics and health centres in both the Khomas and Oshana regions, noted that it was not necessary to use ICT such as the telephone constantly for internal communication in their health institution. The argument was that some of these institutions were small and would rather use verbal communication by way of holding meetings for employees working in the same health facility.
The most commonly used ICT by health service providers for external communication with other institutions was the telephone (52%) followed by postal services (20%). Ten percent of health service providers used email to communicate with other institutions. Only 7% used courier services. Another 7% used fax machines. Other more sophisticated ICTs used were virtual meetings (i.e. videoconferencing) specifically for the Oshakati hospital. The virtual meetings were used to communicate with other health institutions in different geographical regions.
Communication between institutions and administrative offices at the district level was mostly by telephone (62%). The postal service (57%) was also used as a way of sending reports to the MOHSS head office. In addition to meetings and couriers, another method of communication that did not directly involve the ICT-related communication tools but was commonly used by almost all the public health institutions involved sending reports with people going from one health institution to another (43%). The reports were normally sent with the ambulance driver or with the district drivers.
Both districts had a schedule for reports to be collected from all the public health facilities using district vehicles. Reports were then sent to higher levels (regional and national headquarters) via email or computer diskettes. Some institutions mentioned that videoconferencing was also used to report to administrative offices and this mainly occurred in major hospitals. Email (19%) was used more than courier services (14%) as a communication strategy between health service providers and higher levels in the health service delivery hierarchy. Figure 2 shows communication between health service providers and higher levels in health service.
Health service provider communication strategies with higher levels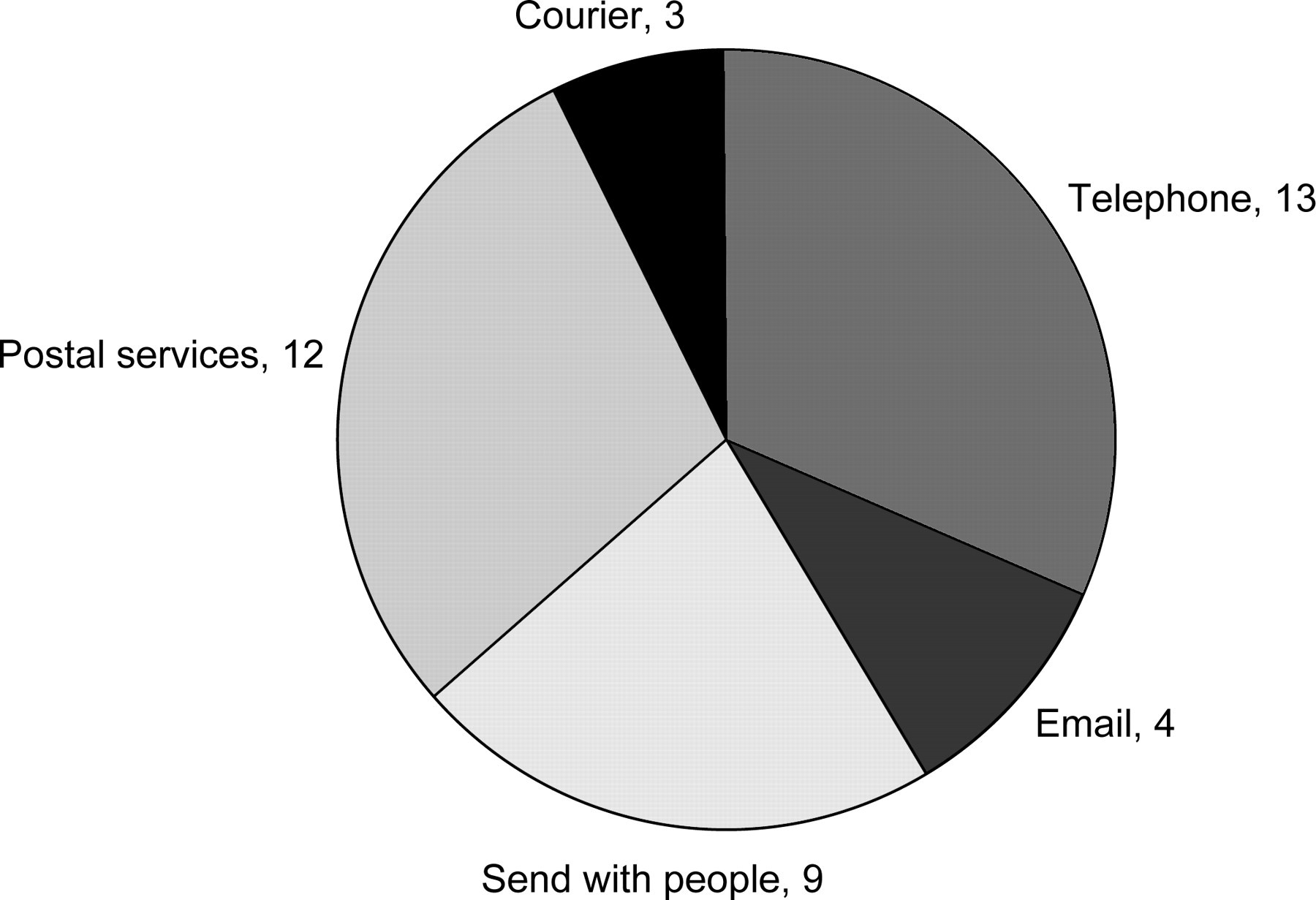
Discussion
The health service provider survey revealed the need to increase awareness of ICT before its widespread use would be feasible. High awareness of ICT was observed in both regions. Most respondents in both regions were aware of ICT even though not all had access to them. This was more common in the Oshana region, where health service providers or medical personnel were aware of computers and the Internet, although some had never used them.
The most commonly used channels for communication were the telephone followed by TV. Health service providers reported that they were not using radio as a main communication channel for health information provision, as stated by patients, which implies that most of the health programmes and health services broadcast on the radio were not initiated by the MOHSS. Mobile phones played a significant role in admissions and emergency services, suggesting that they could be used as effective tools to aid or promote rapid response to medical emergencies in Namibia.
The use of ICTs for service delivery played an important role in the health sector. There is need to provide more training and align the ICT needs of patients with those of health service providers in Namibia to ensure effective use. In other words, health service providers must promote the use of ICTs that are commonly available to their patients, such as radio, TV and mobile phones. The use of newer techniques such as podcasts and Skype is still very limited in most developing countries. However, with increased budgets for ICT infrastructure development and training, the use of these modern tools will expand and can be expected to improve the overall access to health services in Namibia.
From the study results, it was observed that key constraints in delivering health services were:
budgetary constraints. The allocated funds were insufficient to buy all the necessary ICT for service provision to patients;
lack of basic infrastructure to support health service delivery. Some health facilities, especially those in the rural areas, lacked basic infrastructure such as electricity, and this was a major constraint in using ICT, such as personal computers and emails.
To enhance the use of ICT in health service delivery in Namibia the following steps should be considered:
draft a comprehensive ICT-based health service delivery policy; provide adequate budgets for personal computers, especially at operational level, since capturing and processing the data at district level is prone to errors; establish sustainable funding for training sessions for health service providers to facilitate the use of ICT in health institutions; integrate the use of mobile phones which are widely used in Namibia to enhance efficiencies in the admission and emergency service units.
The application of ICT in health service delivery of Namibia is expected to generate two main benefits: improved quality of health care and increased patient outreach. The anticipated benefits from ICT use such as improved quality of services, relatively easier access to health information and faster diagnosis are widely acknowledged worldwide.
Footnotes
Acknowledgements
We are grateful to the Cape Peninsula University of Technology for financial support.