
Abstract
We conducted a feasibility study of a system for non-invasive monitoring of subjects at home. Electrical activity was recorded from room lights and from electrical domestic appliances; this was translated into the probability of physical activity or a particular Activity of Daily Living (ADL). Thirteen volunteer subjects were monitored for a period of 6.4 months (range 3–8). The mean age of the subjects was 80 years and they all lived alone at home; one had moderate Alzheimer's disease. A one-week validation was carried out to ascertain whether the recorded activity actually occurred. The results showed that daily and nocturnal activity could be well differentiated. The probability of having eaten, taken a bath and going to the toilet could be calculated each day. Eating was the most accurately measured ADL; toileting and bathing results were less accurate. The system appears to be a promising component of home telecare.
Introduction
The importance of daily health monitoring at home in order to evaluate health status and quality of life has been proposed by Dittmar et al. 1 Some authors have developed the concept of continuous monitoring using different sensors in order to model human activity in their home. 2 A few clinical applications have been proposed in the field of home surveillance, mostly based on an identifiable routine of activity. Some publications have described the use of different types of sensors for recording movement or temperature or activity. Le Bellego et al. used a hospital suite simulating a person's home, equipped with a network of passive infrared (PIR) sensors in order to study activity, mobility, occupation and agitation. 3 The use of infrared sensors to detect an occupancy pattern in an experimental room has also been studied by other groups, but accuracy remains to be proved in different types of rooms, since the detector output depends on the velocity of movement and the distance. 4
Calculating energy expenditure for elderly people at home using these types of sensors has also been proposed by Kaushik and Celler. 5 This has been tested in an experimental set-up. Although the results were promising, the principal problem was that sensors could not differentiate the test subject when more than one person was present in the space being monitored.
Recognition of posture using a 3-D camera has also been tested, but the system was tested with a younger person. The results were promising: the system was capable of classifying position as standing, sitting or lying down. 6
Bonhomme et al. proposed extending their system which was based on a presence sensor to the environment of the home, but keeping wearable sensors to enhance sensitivity; this would probably not be suitable for persons with cognitive problems. 7 Nowadays the goal is to monitor people at home in order to keep them safe and in good conditions. Suzuki et al. 8 used a combination of sensors to follow a person living independently alone at home. They were able to identify a pattern of daily activities that allowed monitoring and detection of possible anomalies.
We have conducted a pilot study of a new method of surveillance at home based on recording the electricity used by light fittings and common electrical domestic appliances (EDAs). The aim of the present study was to test the acceptability of this method of non-invasive monitoring.
Methods
Subjects from the Rhône-Alpes Region of France were selected between May and August 2005. They were recruited by old peoples' associations or personal invitation by the investigators. The inclusion criteria were:
living alone at home; having an AGGIR score of more than 5; having a reference person (relative); being independent for instrumental activities of daily living (IADL); having a general practitioner; being able to give informed consent. having severe cognitive impairment (MMSE score <16); leaving their home too often (more than twice a day); likely to be non-compliant (i.e. people who travelled regularly); being seriously ill or likely to require hospitalization.
The exclusion criteria were:
Ethics
All subjects provided written informed consent explaining that they were free to abandon the protocol any time if desired. According to the French legislation on human medical studies, 9 this type of study did not need to be approved by a hospital ethics committee, but it was accepted by the national commission on rights on electronic data. Confidentiality was assured through data decryption and use of passwords to access information.
Installation of the equipment
On the day of installation, a questionnaire was completed regarding self-perception of health and physical activity, weekly schedules and whether a person or home care service came to the house.
For the technical part there were three steps:
installation of a sensor to detect the electricity used by the chosen EDAs and lights in the house; calibration of the chosen EDAs and lights; installation of an ADSL line for data transmission.
During the calibration step, each EDA or light had to be turned on and off at least 10 times to be detected and registered properly. Some appliances were classified as ‘simple’, such as the oven and coffee machine, and some were classified as ‘complex’, such the washing machine and dryer.
Data were transferred to an external server for analysis. Each subject was monitored for a week and asked to record their daily activities so that we could verify that the electrical activity detected corresponded to reality and whether the person had really used the appliances that were recorded.
Use of each EDA was assigned a weighting factor to be used in the calculation of an activity score. For example, using the coffee machine daily was assigned the maximum weight, an iron used twice a week was assigned medium weight, and the lamp over the stove was assigned the minimum (Table 1). At the central server, the data were displayed on a web page (Figure 1). To differentiate activity during a 24-hour period, the results were divided into the following time frames: 05:00–22:30, 22:30–23:59 and 00:00–04:59. For the final total daily and nocturnal activity score the timeframe was 05:00–22:59 and 23:00–04:59.
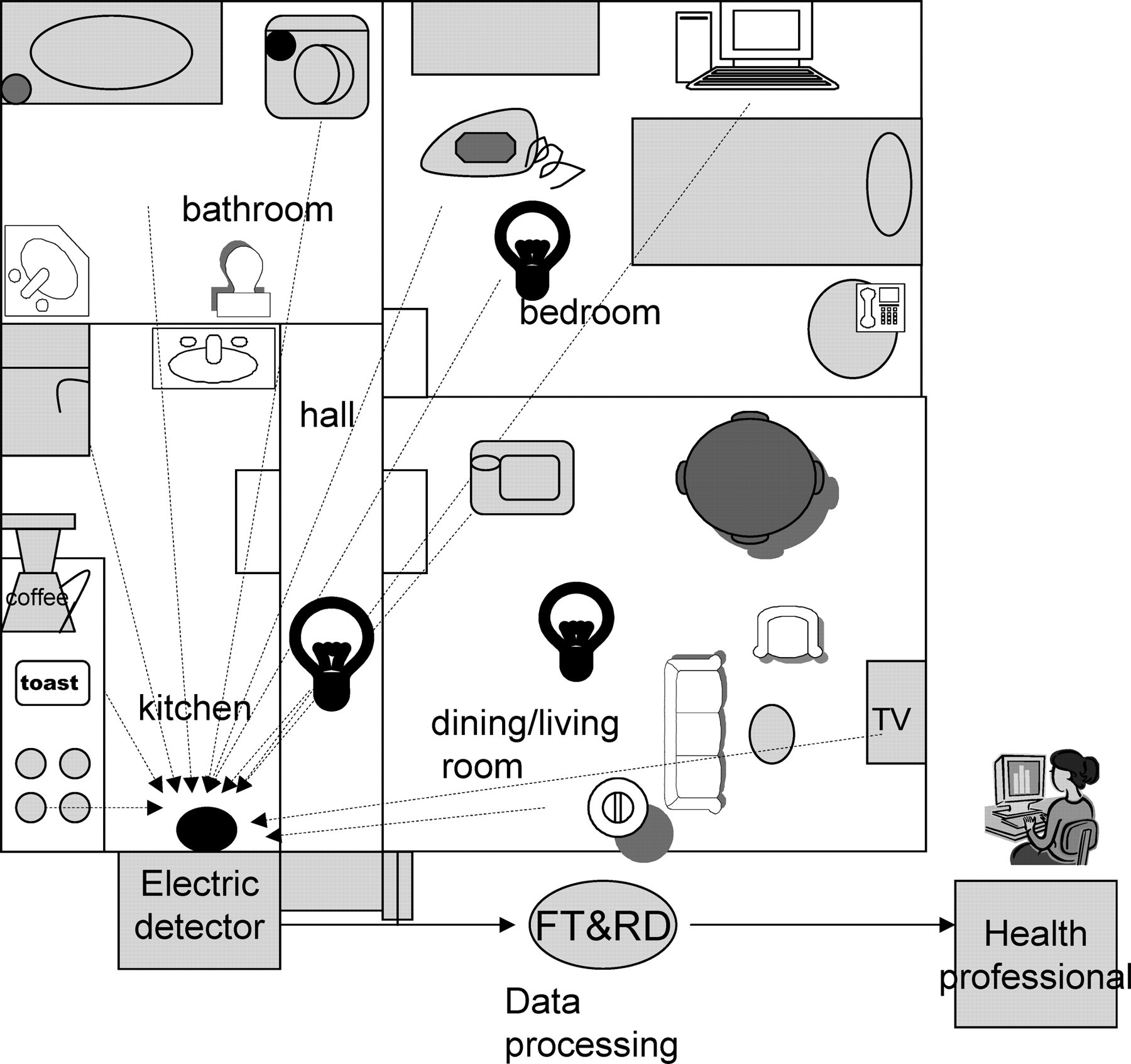
System architecture
Classification of electrical activity detected
Acceptability of the system
To evaluate the subject's opinions of the project, a questionnaire was designed with three main objectives:
the individual's judgement of his/her age, own perception of aging, independence and way of life; opinion about participating in the project; final impressions about the project, once it had ended.
There were 33 questions. The questions were based on a previous study of patients monitored in hospital.
10
In the present study, the persons were in good conditions at home, so that open questions were preferred. Questions were posed, such as ‘Were you conscious of being observed?’, ‘Did you feel more secure?’ and ‘Did you change your behaviour because of the system?’
Results
Data were collected for an average period of 6.4 months (range 3–8) from 13 subjects. There were 11 women and two men, whose average age was 83 years. Ten people were living in an apartment and three of them in a house. The level of activity did not change substantially between the summer and winter, but differences were detected between subjects as measured by rooms visited, with a mean of eight rooms visited daily for sedentary persons and 43 for very active subjects. Four of the subjects had a carer who helped with cleaning and three subjects received ‘meals on wheels’. Ten persons were in good health (physically and socially active), two were less fit due to co-morbidity and obesity, and one subject had moderate Alzheimer's disease.
The average number of EDAs monitored, including lamps, was 20 per home (11–28). The data also provided useful information, such as the type of room being occupied. This was identified by a colour scale, e.g. blue for bathroom, green for kitchen, grey for living room. When a person left their home, no activity was recorded so that empty intervals could be seen. The colour-coding enabled easier detection of patterns when visualizing the whole week (Figure 2, upper part).

One-day activity and ADLs of a subject
We were able to identify occasions on which two subjects had someone living with them because the mean rate of activity doubled.
Accuracy of the sensors
The main problem was that the sensors did not register electrical activity if the lamps in the light fittings were too weak (<40 watts). However, there were no false readings, since no electric activity was registered at all during periods when the subjects were absent and the activity readings increased significantly with the number of people present.
Another problem was that some people did not always turn the light on when going to the toilet. Hence, the results for the ‘bathing’ ADL were not accurate for five subjects and were biased in other cases.
The diaries from the subjects who recorded their daily activities were compared to the electrical activity detected and there was good agreement.
Translating activity into ADLs
To translate activity measurement into the probability of performing a specific ADL, two variables were analysed:
the presence of the individual in a room, as detected by a light being switched on; the use of an EDA corresponding to a certain activity.
Colour codes were used to facilitate the visualization of the results, e.g. eating was recorded as green, toilet-use as blue, nocturnal activity as black. Figure 3 shows the activities of a person with Alzheimer's disease who was very active during the night, with irregular eating patterns compared to a normal subject.
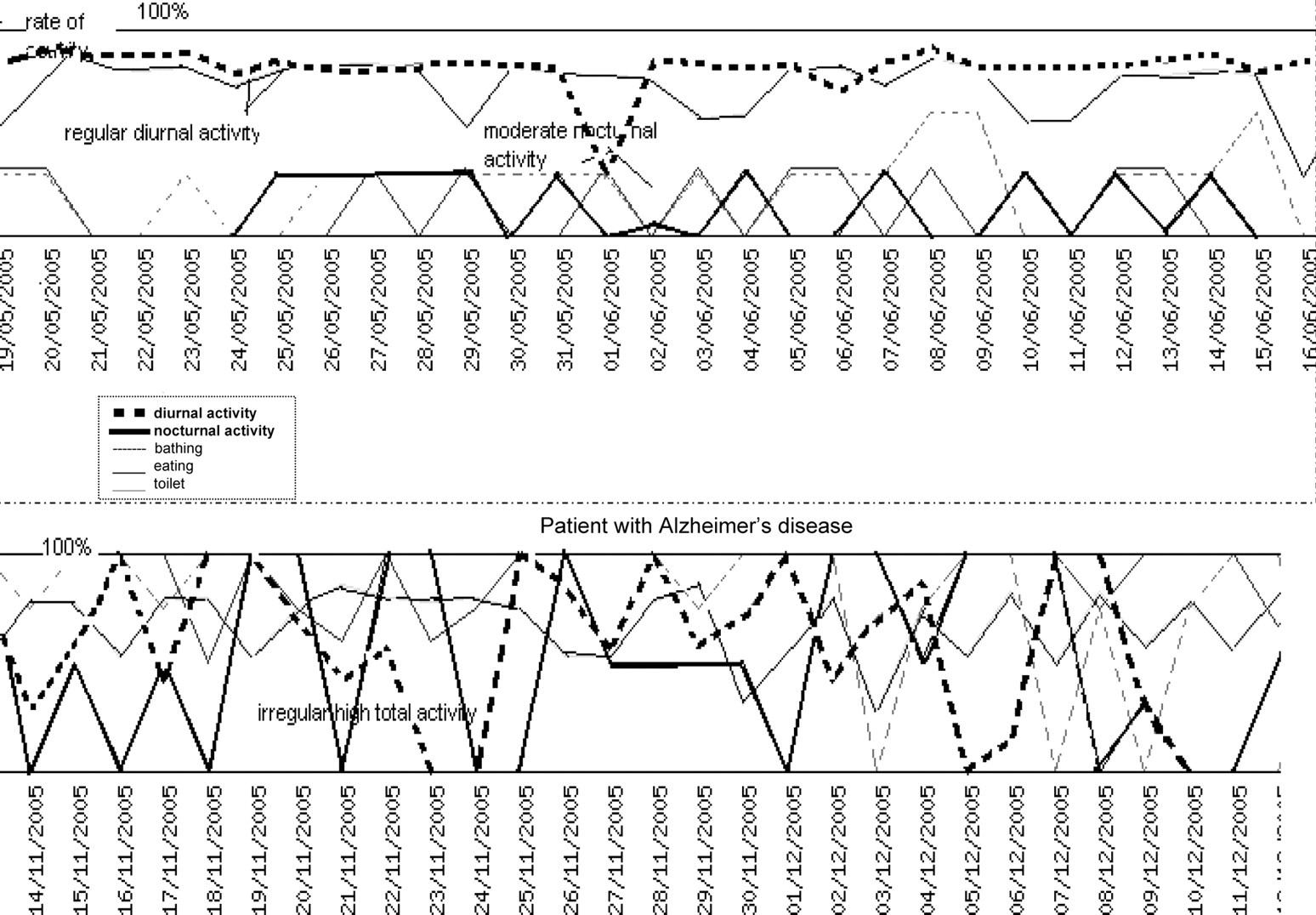
Total activity expressed in ADLs for a normal subject and a patient with Alzheimer's disease
Useful information could be obtained from these data, such as the patient with Alzheimer's disease who had not previously reported sleep problems. For example, Table 2 records the subject visiting the garage and the bathroom at night, hence signalling odd behaviour. We were able to identify other typical night-time scenarios, like watching the television or wandering about in the house.
Activity measurements in a patient with Alzheimer's disease during a disturbed night
Subjects' impressions
All 13 participants wanted to stay at home as long as possible. Seven participated in the study to help the person who recruited them and four to help further research. Eight subjects found the equipment installation period too long, 12 did not like being monitored and 10 forgot about the equipment once the cables were hidden. All were interested in having feedback on the results and eight wanted to be informed about their perceived level of independence. Twelve subjects believed that their physician was best suited to analyse these results. In general, negative impressions were due to the equipment installation period and having too many cables in some rooms.
Discussion
The present study was conducted to test the feasibility of the method of home surveillance. The system was able to identify a personal pattern of behaviour for each subject according to the probability of having performed an ADL and it could also differentiate between a person with Alzheimer's disease and the normal subjects.
The study showed that activity was regular and different between subjects and that patterns could be recognized. Even if all patients had a high total ADL score, individual activity patterns were very different, both quantitatively and qualitatively. This suggests that scoring ADLs by commonly used scales may not be sufficient. Such differences are probably related to morbidity, age or habits, but analysis of these variables was beyond the scope of the present study.
Like other authors, we reported the level of total day- or night-time activity. 11 This has proved to be useful when using different technologies, such as infrared sensors in doors, windows and the electricity signals. Most previous reports have been based on identifying a pattern of normality, usually defined by the mean ± 2 SD; when outliers are detected an alarm is given. 2,8,11–13 In our system this is also possible but the pattern of normality can be easily identified, either by the colour-coded activity patterns, or by the rate of activity calculated (Figure 2). The coloured pattern can be visualized on a single page for a whole week, showing the personal pattern corresponding to daily activities. For example, no activity was registered when the person left the home.
Elderly people tend to have stable lifestyles, enabling the detection of abnormalities in their rhythm of daily living. With our system, a table may be accessed showing the number of movements between rooms for a time period and it can be seen whether this rate increases or diminishes. Thus if a person spends too much time in a particular room this could suggest fatigue or illness. Elevated activity for persons who are wandering or agitated can also be recognized.
Suzuki et al. 12 followed the pattern of daily living of a 72-year-old woman at home using different types of sensors, mainly through movement recognized by infrared and photo-electric sensors, and electrical activity coming from the television. They were able to differentiate activities like sleeping, getting up, having breakfast, going out, having dinner and going to bed. Similarly these activities were detected from patients in a nursing home using the same principle. 13
Future applications
Information on using the toilet and bathing are crucial. In other publications, it has been reported that an increased frequency of toilet use can indicate a urinary infection or an episode of diarrhoea. It is well known that bathing disability is an independent risk factor for frailty and an important marker for loss of independence. 14 If the total amount of activity diminishes, or if people spend longer periods in their bedroom, for example, this may indicate sickness. However, the primary function of our system is to detect early loss of independence. Such loss of independence is often underestimated, especially if elderly people are keen to stay at home. Our system can help to identify whether it is a global level of independence or a specific task that is affected. Another advantage is that details of activity can be revealed, such as whether a person uses the vacuum cleaner, does the ironing or uses the oven.
Our system may also be useful for evaluating sleep versus night-time activity, as exemplified by the patient with Alzheimer's disease in the present study. Similar nights of insomnia with other types of activity were seen in other subjects. As demonstrated by previous studies, an infrared sensor close to the bed could also be installed to improve accuracy or provide more information about motor activity during the night. 15
Regarding the acceptability of the system, most individuals accepted the idea of a non-invasive tool, as long as there were no cameras. As Demiris et al. reported, elderly people show overall a positive attitude towards devices and sensors, once they understand their use. 16 In our study, only two people thought that there were too many cables. There was some concern about the home electricity bill increasing too much; however, the cost was only about €30 per month. We included some questions regarding the self-efficacy of the system and others concerning anxiety which have been proved to be important constructs in evaluating the acceptance of home telecare. 17
Suzuki et al. recently reported the use of infrared sensors at home, finding that a shorter sleep time and the number of outings were highly correlated with the detection of early dementia. 18 With our system, we too could identify that the patient with Alzheimer's disease living alone had an odd pattern of activity (Figure 3) with a persistent elevated night activity, wandering and with an irregular eating pattern. In fact this subject lost weight and had a fall with a hip fracture some weeks after the study and her physician did not notice this alteration in advance, because the patient referred to herself as being in good health. Hence, our system would probably be useful for evaluating the independence of patients with early to moderate dementia, living at home. 19
Footnotes
Acknowledgements
The system MAPA (Mesures de l'Activité des Personnes A domicile or Measuring Activity of People At home) and all technologies were developed by Orange France Telecom R&D in Grenoble, France. We are grateful to Nicole Giraud for support and to Miss Faith Dyer for assistance with the English writing.