
Abstract
We conducted a multicentre study in five Italian hospitals to assess the feasibility of a remote monitoring service for the follow-up of implanted cardiac devices. The system was designed to monitor device performance as well as physiological aspects of the patient's condition. Sixty-seven patients (mean age 64 years) affected by chronic heart failure and with a biventricular implantable cardioverter defibrillator for cardiac re-synchronization therapy (CRT-D) were enrolled for a three-month observation period. A total of 267 device recordings were transmitted through the ordinary telephone network, with a success rate of 99%. The telemonitoring service was more efficient than conventional face-to-face follow-up in terms of the time savings: both for physicians (4.7 minutes versus 15 minutes for remote and conventional monitoring) and for patients (6.6 minutes versus 116.3 minutes). In addition, a total of 23 clinical events occurred during the study, but only two cases required a clinic visit, thus reducing inappropriate hospital admissions. Finally, the service was well accepted by all the users.
Introduction
An implantable cardioverter defibrillator (ICD) is a battery-powered, fully implantable device, which can monitor the heart rhythm and deliver an electric shock to restore normal sinus rhythm when a potentially life-threatening arrhythmia is detected. 1 All devices have four functions: arrhythmia detection, arrhythmia treatment, bradycardia pacing and episode-data storage. 2 ICD, associated with cardiac re-synchronization therapy (CRT), has been shown to be effective for primary or secondary prevention of sudden cardiac death in patients with chronic heart failure. 3–6 Thus there has been a rise in new implantations 4 and a consequent increase in the number of follow-up visits in hospitals. 7 Follow-up visits are usually scheduled at three-month or six-month intervals. 8 The main disadvantage of intermittent follow-up is that any device problem which occurs will not be identified quickly. 9 Additional unscheduled visits are often required to investigate symptoms that may or may not be related to the cardiac disease or device. 10
Remote monitoring of cardioverter defibrillators is an alternative to frequent visits. The physician can decide whether the patient needs a visit to the outpatient clinic for device re-programming, 11,12 an emergency admission, a change in therapy or nothing. This reduces the need for follow-up and enables the individualization of correct routine follow-up intervals 13 avoiding unnecessary visits. In addition, remote monitoring allows the early detection of changes in the rhythm state of the patient 14 and the review of information from the device such as battery voltage and lead impedance.
Remote monitoring service
The Medtronic CareLink Network is an Internet-based remote monitoring service designed to assist physicians in the management of chronic cardiovascular diseases treated with an implantable device (ICD or pacemaker). There are two main components:
a small device, the Medtronic CareLink Monitor, with an attached aerial for wireless data transfer. The monitor is powered by batteries and can be plugged into a standard telephone connection; a website, where clinicians can monitor the condition of patients who use the device.
The service allows patients to interrogate their implanted device by pushing a button to turn on the Monitor and placing the aerial over the device. Then the Monitor automatically transmits device-related and physiological data to the Medtronic CareLink Network via the telephone connection. In addition to the review of the transmissions, the user interface has an event notification which displays alerts, for example when a shock has been delivered or in case of certain out-of-range values. Implantable device data available on the website are equivalent to data available from an in-clinic interrogation-only device evaluation.
11
Limited bidirectional communication is possible (e.g. setting of alarms), but ICD re-programming can only be done during a clinic visit.
The Medtronic CareLink Network has been adopted by several clinics in the US and preliminary results have been published elsewhere. 15 The aim of the present study was to assess the Medtronic CareLink Network in a European clinical practice setting.
Methods
A multicentre observational study was performed involving five Italian hospitals. The hospitals were experienced in monitoring implanted patients. They all had suitable staff, managerial skills, structures and knowledge about heart failure and ICD for the routine control of their patients.
Patients affected by heart failure and implanted with a biventricular defibrillator for cardiac re-synchronization therapy (CRT-D) were selected for the study. Biventricular defibrillators use a coronary sinus lead for left-ventricular pacing, in addition to the leads placed at the right ventricular apex and in the right atrium. These devices are capable of continuous assessment of several diagnostic variables such as patient activity, heart-rate variability and the intra-thoracic impedance (a surrogate measure of fluid overload) and can generate an audible alarm in case of persistent decreases of measured impedance.
Inclusion and exclusion criteria
Baseline data (n = 67)
NYHA = New York Heart Association classification
There were five scheduled patient visits in the evaluation. Two clinic visits were performed at baseline and at the end of the observation period, three months later. In addition, three remote visits were performed through the remote monitoring system at 2 weeks, 1 month and 2 months after baseline, and the transmitted data were reviewed by clinicians. Patients received training about the remote transmission technique and clinicians conducted the standard routine ICD check with a full ICD interrogation.
If the patients experienced any difficulty in using the device, they were asked to contact the hospital. Unscheduled visits could occur when patients were symptomatic or received a shock from their biventricular ICD. In these circumstances, the clinician assessed the patient using the remote monitoring system. If the clinician felt that the patient needed further medical attention, a clinic visit or an emergency admission were requested.
Assessment
Technical feasibility was measured as the rate of successful transmissions, accomplished without requiring a troubleshooting call. Efficiency was measured as the time used by clinicians and patients for the remote transmission and the subsequent review of data. Patient time was measured for each of the three scheduled remote visits (2 weeks, 1 month and 2 months after baseline) as the average time required by the patients to complete the remote transmissions. These times were compared to the average time usually spent for an ordinary follow-up visit, measured during the baseline clinic visit as the sum of the time required for the round trip home–hospital, the waiting time before the visit and the time for the ICD control. The time required by the physician for the remote review of transmitted data was compared to the duration of the traditional clinic follow-up visit.
Clinical utility was assessed by the number of unscheduled contacts that occurred. In particular, patients were asked to contact the clinic by telephone in case of symptomatic events, ICD shocks or acoustic alarms. After the patient contacted the clinic, the physician assessed the patient by telephone and then, if necessary, requested the transmission of the implanted device data using the remote monitoring system. If the physician felt that the patient needed immediate medical attention, a visit to the clinic or the local emergency department was suggested.
User satisfaction was measured by questionnaires submitted both to patients and to clinicians about the use of the telemedicine system compared to traditional in-clinic follow-up.
Results
Technical feasibility
At the end of the study, only three troubleshooting calls had been recorded for technical problems. Consequently, the success rate, computed as the ratio between the number of successful transmissions (264) and the total number of successful and unsuccessful transmissions (267), was 99%. In all the three cases the problems were solved after contact with Medtronic.
Efficiency
The average time spent by patients for the three remote scheduled transmissions was 8.1 min (SD 5.5), 7.8 min (SD 5.8) and 6.6 min (SD 3.5), respectively. This was lower than the time usually spent for a traditional clinic visit (116.3 min [SD 89.5] (Figure 1). This time saving mainly resulted from the avoidance of the round trip home–hospital (85% of the total time) and the waiting time before the visit (2% of the total time) by performing a remote monitoring control instead of a clinic visit.

The time used by patients for clinic visits and remote data transmission
In all the hospitals, standard device follow-up was carried out by an electrophysiologist assisted by a nurse and the observed time for this visit was 15 minutes. In contrast, the average time required for a remote review of a transmission was 4.7 minutes (SD 2.0) (Figure 2). The telemonitoring allowed a saving of two-thirds of the physician time normally spent for the standard follow-up visits.
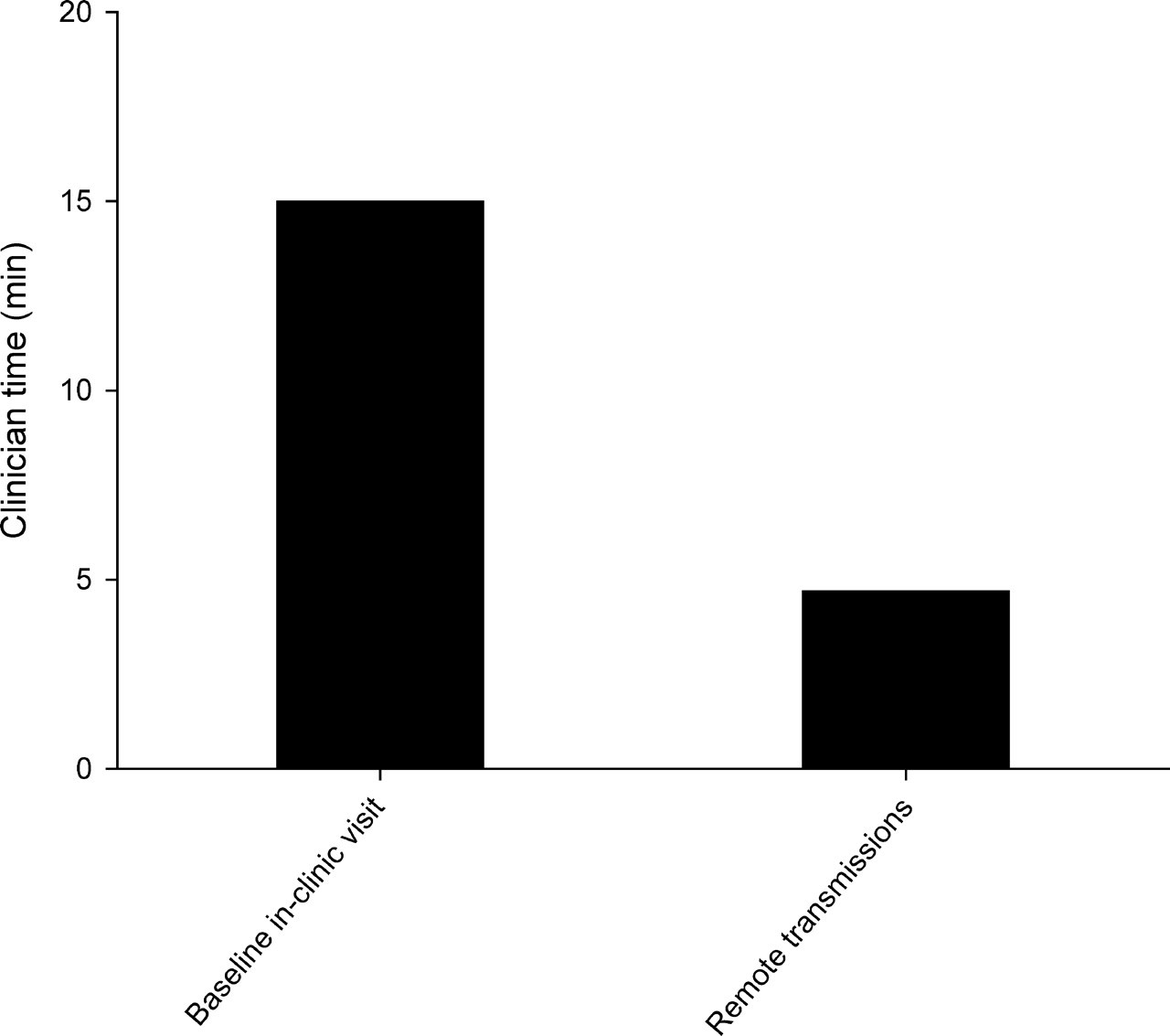
The time used by clinicians for clinic visits and review of remotely transmitted data
Clinical utility
Review of unscheduled contacts and transmissions
User satisfaction
Patient satisfaction (n = 65)
Physician satisfaction
Discussion
ICD remote monitoring systems have been shown to be an effective alternative to frequent clinic visits, reducing follow-up and enabling the individualization of routine follow-up intervals. 11–13 In addition, these systems help physicians to diagnose disease or device related adverse events, thus reducing re-hospitalizations, length of hospital stay, mortality rates 14,16,17 and inappropriate therapies. 9,18,19 Remote monitoring therefore represents an efficient method of health-care delivery that may contribute to reduced costs. 20
A previous study of the use of CareLink was conducted in 59 patients in the US, 15 demonstrating that patients were capable of interrogating their ICD. The review of transmitted data revealed several clinically significant findings and allowed rapid clinical decisions, often avoiding hospital admissions. The present study represents the first European experience with the Medtronic CareLink Network, a system for the remote monitoring of patients implanted with cardiac devices. We conducted a multicentre observational trial. First, the remote monitoring system appeared to be technically feasible in a European clinical practice setting. In fact technical feasibility, calculated as the rate of successful transmissions which did not require a troubleshooting call to Medtronic personnel, reflected a success rate of 99%. This can be compared to the results obtained with other automatic systems. For example, Brugada 13 showed that 12% of patients did not manage to establish satisfactory automatic messaging.
Second, there were time savings both for patients and for physicians. In the literature, there is only one study of time and cost savings achieved through ICD home monitoring compared to the conventional follow-up. 21 The authors demonstrated that home monitoring may avoid up to two visits per year and reduce the overall costs of ICD follow-up by savings on transportation, particularly when the distance between home and medical facility is higher than 100 km. In our study, patients spent on average less than 10 minutes for a remote transmission instead of 116 minutes for standard in-clinic follow-up. Physicians also saved time through remote monitoring.
Third, good clinical utility was observed in the management of both scheduled controls and unscheduled events. The remote monitoring system allowed the physician to continuously check the patient's clinical condition and to review ICD data remotely rather than conducting in-clinic control, with benefits in terms of time and scheduling (remote review can be conducted in batches). In a population of 67 patients, 23 unscheduled events occurred during the observation period, and a clinic visit was required in only two cases.
Finally, the user satisfaction questionnaires demonstrated the acceptance of remote monitoring. Ease of use was reported by the majority of patients (96%). Seventy-eight percent of the population claimed to prefer remote monitoring to the traditional in-clinic visit and 83% reported a positive effect on calmness and anxiety. Patient acceptance of ICD remote monitoring has also been investigated by Res et al., 12 who showed that the service functioned seamlessly in 23 out of 24 patients (97%) during a one-year observation period, with benefits in terms of reassurance for those who experienced a shock. In another study, 22 93–99% of patients indicated complete or high satisfaction with remote interrogation through five measures of acceptance.
In the present study, the physicians indicated positive results in terms of management of scheduled and unscheduled device follow-up and clinical management of patients. In fact, all of the physicians stated that the transmitted data were exactly the same as those obtained through direct device interrogation, confirming the findings of other studies. 19 None of the telecardiology systems currently available commercially (CareLink by Medtronic, 23 Home Monitoring by Biotronik, 24 Housecall Plus by St Jude Medical, 25 Latitude Patient Management system by Boston Scientific 26 ) allows the remote re-programming of ICD settings, 13 but limited bidirectional communication is possible. 11
In conclusion, the present multicentre observational study demonstrated the feasibility of the Medtronic CareLink Network in a European clinical practice setting. Positive findings were related to time saving, clinical utility and acceptance. A multicentre randomized controlled trial is planned. It will trial a new device using wireless transmission within the patient home. 27
Footnotes
Acknowledgements
We thank the following physicians who were involved in the study: M Santini, M Lunati, M Landolina, GB Perego, M Marzegalli, RP Ricci, M Schirru, C Belvito, R Brambilla, G Guenzati and L Tavazzi.