
Abstract
We evaluated the efficacy of two telehealth applications, delivered by telephone and videophone, for improving outcomes of patients following hospital discharge for an acute exacerbation of heart failure. The outcomes measured were patient self-efficacy, satisfaction with care and knowledge of and compliance with prescribed medications. At hospital discharge, patients were randomly assigned to either control (usual care), telephone or videophone groups. Study nurses contacted the intervention patients each week for 90 days after discharge. A total of 148 patients were enrolled: 49 were randomized to usual care, 52 to the videophone intervention and 47 to the telephone intervention. At 90 days, 126 patients (85%) had completed follow-up; at 180 days, 109 patients (74%) had completed follow-up. There were no significant differences between the groups in medication compliance, self-efficacy or satisfaction with care. The intervention group patients were more likely to have had their medications adjusted during the 90-day intervention period. Knowledge scores improved in the intervention group patients, although these scores were lower at enrolment compared to the control group. It is possible that routine monitoring of symptoms by the study nurses led to medication adjustments and accounted for the intervention patients' significantly delayed time to readmission relative to the control patients.
Introduction
Heart failure (HF) is a chronic progressive disease characterized by declining function punctuated by acute exacerbations and frequent hospital admissions. Optimum care depends on health-care providers delivering appropriate medical care and patients complying with recommendations. 1–3 The goal of therapy is to help patients achieve clinical stability, including freedom from congestion, stable fluid balance and vital signs, and ability to engage in moderate activity. Failure to achieve clinical stability may be caused by a patient's lack of knowledge or failure to recognise warning signs of decompensation, by noncompliance with therapeutic recommendations, or by inadequate social support or financial resources. 1
Patients with chronic illnesses such as HF face a number of daily self-management tasks, including recognizing and managing symptoms, using medications, managing acute episodes, as well as dealing with nutrition, exercise, stress-reduction, communication and appropriate use of resources. 4 Patient knowledge and confidence to manage chronic illness can improve when health-care professionals offer surveillance, advice and continuity of care. 4 Early detection of potential problems increases through intensive outpatient monitoring. This provides access to health information, feedback on reported symptoms and strategies to enhance compliance. When a patient's self-management improves, so do outcomes, including quality of life, health status and satisfaction; at the same time, resource use decreases. 1
Care facilitated by telehealth has the potential to enable earlier detection of key clinical symptoms indicative of HF-related decompensation. It can also trigger earlier implementation of medication, dietary and lifestyle adjustments. Only one previous randomized trial 5 of HF follow-up care has compared telephone and videophone approaches with usual care. However, the study was relatively small (n = 37), and investigators encountered a high rate of technical problems with the videophone, i.e. 76% of encounters were limited by technical problems, primarily poor video resolution.
The present study reports data from a randomized clinical trial that evaluated the efficacy of two telehealth applications, delivered by telephone and videophone, for patients following hospital discharge for an acute exacerbation of HF. The primary endpoint was hospital readmission. 6
Methods
The study was a randomized controlled trial; details have been reported elsewhere. 6 The study was conducted at the Iowa City Veterans Affairs Medical Center (ICVAMC), a 107-bed tertiary hospital. The study was approved by the appropriate ethics committee.
Patients were screened within 24 hours of admission to identify potential participants admitted for heart failure exacerbation. After providing informed consent, patients were randomly assigned to one of the three study groups: usual care, telephone intervention or videophone intervention. The intervention, modelled on previous work, 7 was consistent with American Heart Association guidelines. 8 Two registered nurses conducted all intervention contacts, which included a maximum of 14 contacts over 90 days. Because patients often fail to recall important elements of medical advice, the study nurses reviewed the discharge plan of care with patients during the first intervention contact and reinforced it during subsequent contacts. During all intervention contacts, the study nurses assessed patients using a standardized symptom review checklist. When patients reported symptoms, such as weight gain, the nurses reviewed patients' reported data, reinforced the plan of care, and made referrals (e.g. to a dietician) or contacted the patient's physician for care plan adjustments. During the contacts, the study nurses had full access to patients' medical records.
Home telecare equipment
Patients assigned to the telephone group participated in all intervention contacts using the telephone in their home. Patients in the videophone group initially used a commercial videophone (EHC 200 Sentinel Patient Station, CyberCare Technologies). The system provided videoconferencing at 10-15 frames per second with a resolution of 176 x 144 pixels. The unit connected through an ordinary telephone line at a data rate of 33.6 kbit/s. During the enrolment period, CyberCare Technologies went out of business, and a different videophone was installed instead (TeleVyou 500SP videophones, Windcurrents Technology). This device had a built-in speaker phone, a 5-inch colour video screen with a resolution of 176 x 144 pixels, and transmitted video at 15 frames per second. A research assistant installed the videophones, trained patients in their use, and removed them at the end of the intervention.
Measures
Self-efficacy can be enhanced through performance accomplishments (engaging in a particular behaviour), vicarious modelling (observing another similar individual engaging in a particular behaviour), verbal persuasion (the influence of credible individuals) and physiological cues. Enhanced self-efficacy leads to changed behaviour, motivation, thinking patterns and emotional well being. 10 Two scales were used to assess self-efficacy: Self-efficacy to Manage Disease in General and Self-efficacy to Manage Symptoms. 11 The Stanford Patient Education Research Center developed the scales for use in patients with chronic illnesses. Each scale contained five items using a Likert scale (0 = not at all confident to 10 = totally confident). The scales were tested on a large sample of clinic patients (n = 1130). All item-scale correlations (internal consistency reliability) exceeded 0.50.
Satisfaction with care was measured using two instruments. First, all patients responded to two items from the VA outpatient satisfaction instrument to assess all participants' satisfaction with care initially and over time. The first item was, ‘Overall, how would you rate the quality of care you received during the past two months?’ This was rated on a five-point scale (1 = poor to 5 = excellent). The second item was, ‘VA medical care is as good as that provided anywhere.’ This was also rated on a five-point scale (1 = never or almost never to 5 = always or almost always).
Because the VA outpatient satisfaction instrument does not address telehealth, intervention patients completed a second survey specific to telehealth. The survey was a 17-item instrument. Items for the videophone group included, ‘I am able to explain my medical problems well enough over the television’ and ‘I can be as satisfied talking to the nurse over the television as talking in person.’ 12 Each item was rated on a five-point scale (1 = strongly disagree to 5 = strongly agree). For the telephone group, items referred to telephones rather than televisions. In a preliminary test on 32 patients, a 20-item form of the instrument had acceptable reliability (Cronbach's alpha = 0.8), but three items were found to be redundant. When tested on 10 patients, the revised 17-item instrument had high test-retest reliability (r = 0.98).
At hospital discharge, the study nurses asked the patients whether there had been any changes in their prescribed medications. Recent changes (i.e. changes made during the hospital stay) were coded as ‘yes/no’. Knowledge was assessed by asking the patients whether they understood the purpose of each medication and its side effects. Knowledge scores represent the proportion of medications for which a correct response was given, based on the patient's medical problems.
Compliance was assessed by asking the patients whether they had taken their medications as prescribed. Compliance scores represent the proportion of medications for which the participant's responses agreed with the directions for use. This approach has worked well in prior studies and has been found to be similar to examining the timeliness of medication refills. 9
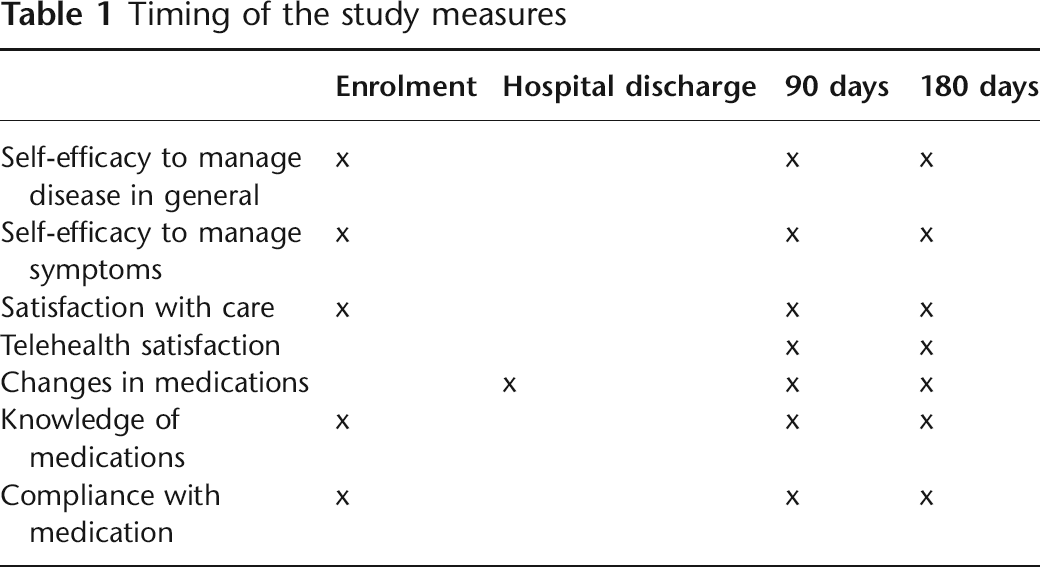
The timing of the study measures is summarised in Table 1.
Timing of the study measures
Data analysis
Continuous data for the three groups were compared using a one-way analysis of variance (ANOVA) and categorical data were analyzed using chi-square statistics. Student's t-test was used for two-group comparisons (i.e. the telehealth satisfaction questionnaire).
Results
Over 39 months, 853 admissions (648 patients) were screened. Of these, 370 patients did not meet the inclusion criteria and 130 patients refused participation. Thus, 43% (n = 148) of the eligible patients enrolled. Of those, 49 were randomized to usual care, 52 to videophone intervention and 47 to telephone intervention. At 90 days, 85% (n = 126) had completed follow-up; at 180 days, 74% (n = 109) had completed follow-up. Among patients who completed the full intervention period (i.e. did not die or drop out), telephone group patients completed 94% of scheduled intervention contacts and videophone group patients completed 96%. Intervention contacts lasted for 34–37 min. Due to technical problems, telephone contacts were used to replace videophone contacts for an average of 2.6 times (out of 14 possible intervention contacts). The intervention resulted in significantly longer time to readmission but had no effect on readmission rates or mortality. 6
The mean age of the patients was 69 years (SD 10); this was consistent with the population of patients treated at the medical centre. Of the patients, 94% were Caucasian and 99% were men.
There were no significant differences among the three groups or across time for either of the self-efficacy measures (Table 2). Intervention group patients had small but non-significant increases in both self-efficacy scores (symptoms and confidence to manage disease) from enrolment to the end of the 90-day intervention. These scores decreased at the 180-day follow-up.
Mean scores (SD) for self-efficacy overall*

*Scoring: 1 = not at all confident; 10 = totally confident
There were no significant differences in the perceptions of care among the groups or over time (Table 3). Satisfaction with telehealth was measured at the end of the intervention period and again at 180 days in the intervention groups only (the control group had no experience with the telehealth intervention). There were no significant differences between the telephone and videophone groups at either 90 or 180 days (Table 4).
Mean scores (SD) for satisfaction with care by group

1The quality of care received during the past two months was: 1 = Poor 2 = Fair 3 = Good 4 = Very good 5 = Excellent
2VA medical care is as good as that provided anywhere: 1 = Never or almost never 2 = Rarely 3 = Sometimes 4 = Often 5 = Always or almost always
Mean scores (SD) for perceptions of telehealth care*
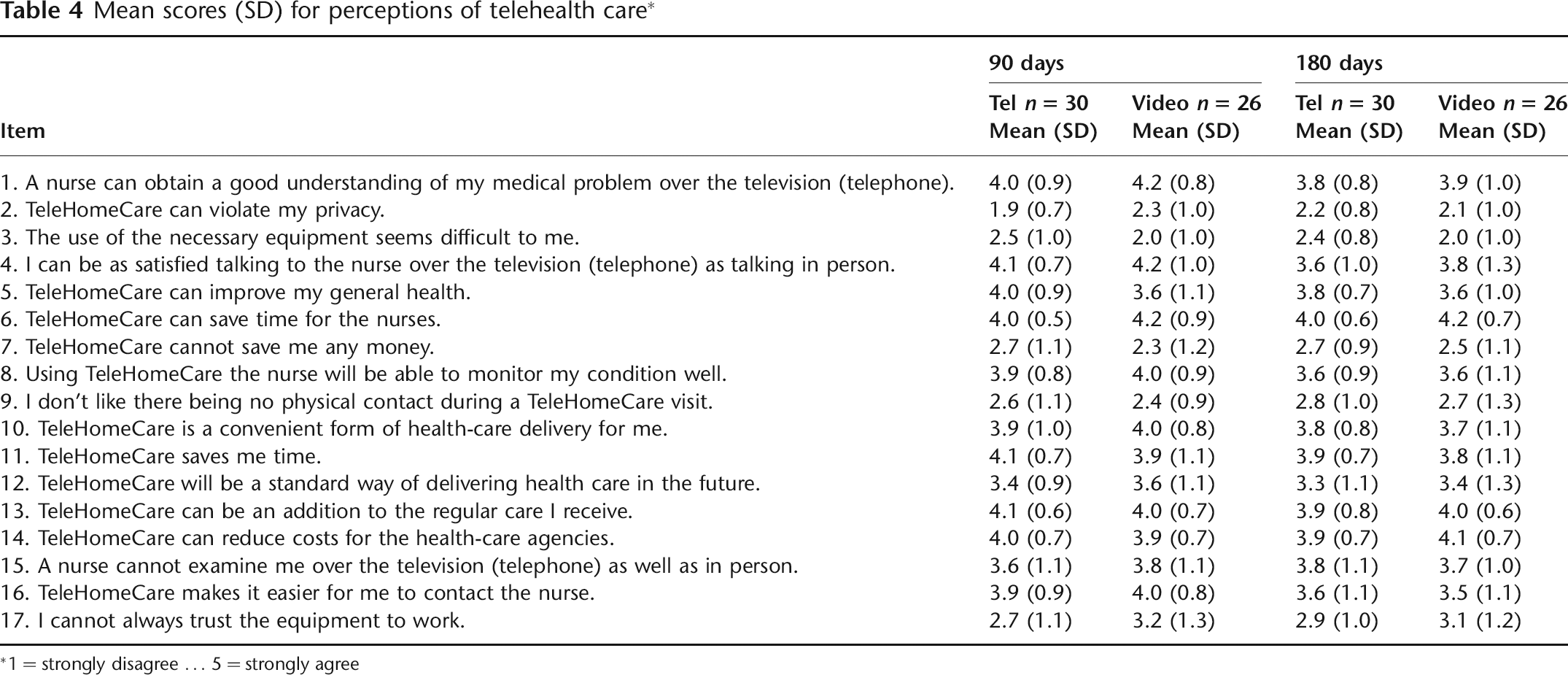
*1 = strongly disagree … 5 = strongly agree
In response to the first question, ‘Have any of your medications changed?’ intervention group patients reported significantly more recent changes in medications (see Table 5). At enrolment, the responses were: control 38%; telephone 52%; and videophone 83% (P = 0.001). At the end of the 90-day intervention, the responses were: control 29%; telephone 48%; and videophone 59% (P = 0.04). No significant differences in changes in medications appeared at the 180-day follow-up.
Medication changes and patient knowledge

1 P = 0.001
2 P = 0.04
3 P = 0.01
*Response ‘yes’ or ‘no’ to question: Have any of your medications changed? (% yes responses shown)
†Proportion of medications for which the responses agreed with the directions for use, in response to question: Do you understand what your medications are for, and their side effects?
Control group patients were significantly more likely to correctly state the purpose and/or side effects of their current medications at enrolment. The responses were: control 97%; telephone 69%; and videophone 69% (P = 0.01). However, there were no significant differences between the three groups at 90 or 180 days. Intervention patients improved from 69% at enrolment to 94–96% at the end of the 90-day intervention period (Table 5).
The compliance question asked, ‘Are you taking your medications as prescribed?’ (data not shown in Table). At enrolment, 97% of controls and 95% of intervention patients answered correctly. At 90 days, the responses were: control 91%; intervention 88%. At 180 days, the responses were: control 91%; intervention 86%. None of these differences was significant.
Discussion
Patients in the intervention group were more likely to report changes in medications at enrolment and at the end of the 90-day intervention period. Their understanding of their medications improved from 69% at enrolment to 94% and 96% at the end of the intervention. This group had small but non-significant increases in self-efficacy scores (confidence to manage disease and symptoms) from enrolment to the end of the intervention. These scores decreased at the 180-day follow-up. No significant differences appeared across the groups in satisfaction with care.
Despite randomization, more intervention group patients than controls reported changes in medications on discharge from hospital. This may have been an artefact of the relatively small group sizes. At enrolment, the intervention patients reported significantly lower understanding of current medications than control patients. Because intervention patients reported more medication changes, they may not have had enough time to learn about new or changed medications. Fortunately, at the 90-day follow up, the percentage of intervention patients correctly reporting medications improved substantially. It is likely that the study nurses' weekly reviews of medications with patients helped them to better understand the purposes and side effects of medications. However, at 180 days, all groups showed slight decreases in medication understanding. The reason for this is unclear. Even so, self-reported compliance was high for all three groups over the course of the study.
Self-efficacy did not improve significantly during the study, even though the study nurses employed self-efficacy enhancement strategies during the intervention contacts (e.g. encouraging the use of community support groups and verbal encouragement and feedback). It is possible that a stronger intervention is required to enhance self-efficacy. Other investigators have documented a relationship between self-efficacy and salt restriction and exercise adherence in veterans with heart failure. 13 Thus, interventions focused on enhancing self-efficacy warrant further attention.
The present study had some limitations. First, we did not assess the appropriateness of the medication profile, i.e. whether patients were on guideline-concordant medications. Thus, differences in outcomes may reflect prescribing patterns. We think this is unlikely because the VA monitors this, and the ICVAMC consistently performs well on these measures. During the first few study contacts, the study nurses attempted to reconcile medications, i.e. discover whether the patient-reported medication list agreed with the electronic record's medication profile. Unfortunately, at the time of the study, the electronic record's medication profile only included medications provided to the patient by the VA. The records did not include over-the-counter medications or medications ordered by non-VA providers. Medication reconciliation is particularly important in this population because patients are cared for by hospital staff while hospitalized, but are followed as outpatients by a different VA primary care provider, and may also see non-VA physicians. Problems with medication discrepancies during the transition from inpatient to outpatient care are well-documented and can be particularly severe for patients on several medications and those with heart failure. 14 Although we did not systematically collect data on medication reconciliation, study nurses anecdotally reported spending a great deal of time during early study contacts clarifying the medication profile with intervention patients. Finally, knowledge and compliance were assessed only for medications, in order to minimize respondent burden. Other areas, such as adherence to diet and fluid and sodium intake, were not measured but are critical self management behaviours in heart failure.
In conclusion, although intervention group patients did not improve in self-efficacy, they were more likely to have medication adjustments over the 90-day intervention period. This group also increased their knowledge about medications. It is possible that routine monitoring of symptoms by the study nurses led to these adjustments and accounted for intervention patients' significantly delayed time to readmission relative to controls. However, this should be validated in a larger sample of patients.
Footnotes
Acknowledgements
The research was supported by the Department of Veterans Affairs, a Veterans Health Administration Health Services Research and Development (VA HSR&D) grant (NRI 99-345), a VA HSR&D Career Development Award to Dr Wakefield, the VA HSR&D Center for Research in the Implementation of Innovative Strategies in Practice, and by the Harry S Truman Memorial Veterans Hospital, Columbia, Missouri.