
Abstract
When visiting patients with serious mental illness at their homes, case managers carried a portable videophone. This was used to access the hospital clinical team via the home telephone line, when an acute clinical need arose in addressing questions related to medication management and treatment planning; travel was therefore avoided. In an acceptability study lasting 12 months, 24 patients received the supplemental videophone mental health service and 19 of them completed a satisfaction survey. Only one patient was not satisfied with the videophone treatment, while 74% of them were very satisfied. Specific areas of satisfaction concerned the savings of time and travel, assistance with medication questions and increased involvement in treatment. No patient reported any difficulty in using the equipment. Staff members were enthusiastic about the decrease in travel time and there were no complaints about the videophone process or encounters. During the study, 135 h of the case manager's time was saved by using the videophone for urgent access visits, equivalent to a saving of $4000 in salary costs. In addition, the patients saved 135 h in travel time. We believe that there are other potential uses of videophones for seriously mentally ill patients, including discharge planning, intensive post-discharge monitoring and transition to community life.
Introduction
The majority of clinical services in telemental health which have been reported in the literature occur through videoconferencing and require patients to travel from their homes to a suitably-equipped location. 1,2 In contrast, home telehealth applications bring care to the patient's place of residence. Home telehealth is used in many clinical areas, but there have been few mental health applications. 3 The latter have been restricted to non-image applications such as in-home messaging and monitoring devices, 4,5 interactive voice response, 6,7 electronic mail 8 or telephones. 9,10 While these modalities can provide real time exchange of educational or clinical material, the lack of images restricts their clinical applications, as an image is important in establishing a presence. 11
Videophones allow an interactive exchange with the patient, albeit at restricted image quality in comparison with conventional videoconferencing equipment. The limited reports in the literature suggest that videophones offer a cost-effective method of providing mental health services to patients at home. 12–19 Menon, 12 Fortney, 13 May 14 and their colleagues demonstrated that low cost videophones could be used in the treatment of depression, anxiety and cognitive disorders. Others have demonstrated use with differing treatment approaches: psychotherapy in terminally ill patients, 15 dignity therapy in advanced disease, 16 biofeedback, 17 neuropsychological assessment 18 and brief psycho-education sessions with the severely ill. 19
While successful use of videophones has been described in the treatment of mental illness, the Hampton Veterans Administration Medical Center (VAMC) appears to be the first organization to use them for intensive case management of persons with severe mental illness. Outpatient intensive case management for severely ill psychiatric patients is an established treatment modality 20,21 that coordinates treatment and promotes access across multiple service lines, diagnoses or cultures. 22,23 In the Hampton VAMC intensive outpatient case management programme, four case managers provide care through home visits for 53 seriously mentally ill (SMI) patients. They provide on-site services at the patient's residence that includes assessment, treatment adherence monitoring, advocacy and social support.
Our catchment area of 50,000 km2 on the shores of the Chesapeake Bay is crisscrossed with barriers such as rivers, creeks, tunnels and bridges that are frequently subject to severe traffic congestion. Case managers spend considerable time facilitating patients' visits as they travel to patients' homes and then back to the hospital to bring the veterans to their clinic appointments. They then repeat this process to return the patient to their home after each appointment. Thus a case manager may spend up to 4 hours in transit for a single patient visit. In addition, most of our SMI patients have multiple co-morbidities that limit their daily functioning, have negative effects on their general health and make travel uncomfortable. Patients sometimes refuse to travel altogether, increasing the deterioration of their physical and mental health.
To improve access to care, we employed videophones in our SMI intensive case management programme beginning in 2006. The present study assessed the acceptability of videophone usage to patients, and the strengths and weaknesses of this treatment approach.
Methods
Patients enrolled in our mental health intensive case management clinic were characterized by severe and persistent mental illness, social/occupational functional impairment and high utilization of mental health inpatient services. Videophone services were provided as part of the routine clinical treatment programme for all patients who had access to an independent telephone line and who gave consent to treatment using videophones for visits by their mental health clinicians.
Following at least one year of videophone participation, patients were asked to voluntarily participate in an acceptability survey designed to assess their experience. Administration of the survey was approved by the appropriate ethics committee and patients gave informed consent for their participation in the survey.
Patients
Of the 53 patients in our intensive case management programme, 24 of them received supplemental videophone mental health services as part of their clinical treatment plan. The other 29 patients did not receive videophone services because they did not have independent telephone line access at their own home, they lived in adult homes with no independent telephone line access, or they used only mobile phones. Of the 24 patients who received the supplemental videophone mental health services, five were not eligible to participate in the study survey (3 left the programme, 1 moved away and 1 was not considered competent to consent). All 19 who were eligible to participate in the survey acceptability study agreed to do so.
Procedure
Case managers used videophones when visiting the patients at their homes to connect with clinicians at the main Hampton VA Medical Center. Each case manager carried a videophone (Wind Currents Diva i300) while making home visits. The videophones were about the size of a laptop computer and weighed less than 1 kg (Figure 1).

Videophone
The videophones were used to access the clinical team from home when an acute clinical need arose in addressing questions related to medication management and treatment planning. These videophone encounters occurred instead of the case manager transporting the patient directly to the medical centre for these urgent access visits.
Medication dosing adjustments and treatment response evaluations were made through videophones by the team psychiatrist. Potential medication side effects or interactions were also discussed via videophones, and medication refill authorization and formulary questions were addressed by the team pharmacist. 24
Family and/or caretaker access to the team psychiatrist for treatment planning questions and functional evaluations was also available. Likewise, remote consultative services like vocational and substance abuse rehabilitation could be discussed and incorporated into the treatment plan. Videophones were not used for behavioural emergencies, or to evaluate lethal ideation.
After an average of one year of videophone use, patients were offered the opportunity to participate in a brief anonymous acceptability survey about the experience. The survey was approved by the appropriate ethics committee and all patients gave informed consent for the survey separate from the previous consent for the treatment with videophones. Patients received the survey to complete at their leisure in their homes in the absence of their clinicians. They were given an addressed envelope to mail the completed survey to the medical centre.
Survey
The survey consisted of seven items. The first question asked the patient to rate their global assessment of satisfaction with the videophone visits, taking into consideration all aspects of the visit compared with travelling to the facility for a face-to-face visit instead; a 5-item Likert scale was used (1 = very satisfied to 5 = very unsatisfied). The next six questions were designed to identify facilitators or barriers to videophone usage.
The veterans identified which of the following statements described their satisfaction or lack of satisfaction with videophone utilization: I am very satisfied with videophone use, I am satisfied with videophone use, I am neither satisfied nor dissatisfied with videophone use, I am dissatisfied with videophone use or I am very dissatisfied with videophone use.
They were then asked to select all of the following statements which applied to their videophone use:
Use of the videophones has saved me time and travel to see my doctor; Use of videophones has helped when I have questions to ask my doctor about my medications; Videophones have not made a difference in my treatment; Videophones often do not work and are hard to use; Videophones have helped my family see my doctor if they have questions about my condition; Videophones have helped me be more involved in my treatment.
Results
Of the 19 patients, 14 were male and 5 were female. Their mean age was 59 years (range 30–82). Fourteen were diagnosed with schizophrenia and five with bipolar disorder.
During an average 12-month period of videophone use, the 24 patients received a total of 77 urgent access videophone visits with their psychiatrist (i.e. an average of 3.2 videophone visits per patient). The visits lasted for 15–30 min. During the same period, the patients were seen by their psychiatrist for a total of 237 face-to-face visits, i.e. 9.9 per patient. Thus the videophone visits comprised 25% of the total contacts with the psychiatrist.
Outcomes
Time/cost: The average travel time for case managers to transport patients from their home to their psychiatrist and back was 105 min. The 77 urgent access visits that were completed by videophone resulted in the following savings during the 12-month study period:
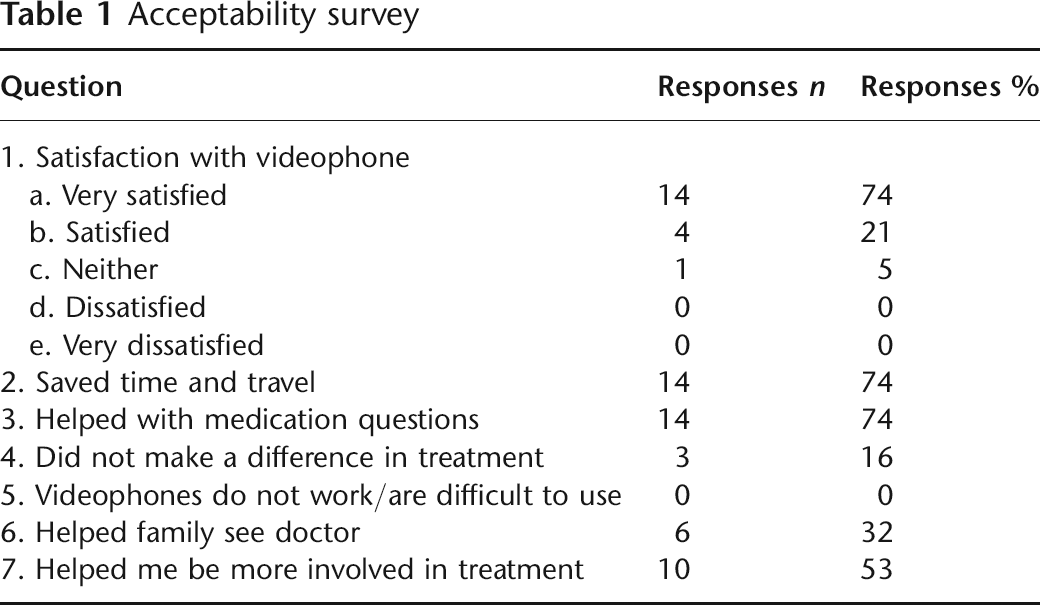
Case manager time = 135 hours, equivalent to approximately $4000 in salary cost; Patient travel time = 135 hours. Patient satisfaction: Of the 19 patients who completed the survey, 14 answered the global satisfaction question with ‘very satisfied’ and 4 were ‘satisfied’ with their experience with videophones. One patient was neutral about the experience, while none reported being dissatisfied (see Table 1). Staff satisfaction: Staff members were enthusiastic about the decrease in travel time and there were no complaints about the videophone process or encounters. Anecdotal staff comments highlighted the usefulness of videophones in patients who had an incentive to remain at home (e.g. patients with difficult family responsibilities, patients who were reluctant to leave pets, or patients with a place of employment near home). Staff also commented that the value of videophones decreased in situations where the patient's need for remote services diminished (e.g. patients who moved closer to the VA, patients who began having weekly appointments at the VA centre for group therapy or for medical reasons).
The psychiatrist time required was the same, whichever modality was used.
Acceptability survey
Discussion
In our study the videophone was not placed at the home of the patient but was carried by the case worker on a home visit. This allowed the patient access to the psychiatrist, pharmacist and other clinicians during the home visit. Over a twelve-month period, more than three weeks of clinician case manager time was saved by using the videophones for urgent access visits instead of needing the case manager to transport the seriously mentally ill patients to the facility. The estimated savings in nurse time amounted to $4000. In addition, the cumulative patient travel time saved was over 130 hours.
The acceptability study demonstrated that the majority of patients were satisfied with the videophones; none of them were dissatisfied. Specific areas of satisfaction were the savings in time and travel and the help with medication questions. More than half thought that videophones helped them to become more involved in their own treatment. Our satisfaction results mirror those of Cluver et al. 15 and Passik et al. 16 who found strong positive perceptions and acceptance of videophone use in the delivery of remote psychotherapy for the terminally ill.
One positive yet unintended result was the veteran's perception of improvement in carer involvement in their care due to use of videophones. The videophones were not specifically used for family interactions, as many of the patients did not have family on-site at their place of residence. Nonetheless, 6 of the 19 patients indicated that videophones improved family and caretaker involvement. This has potential implications for treatment planning, clinical follow up and compliance with treatment as a caretaker may best be able to report early symptoms of relapse.
There were no technical difficulties in the implementation of videophone treatment. There were no problems in initiating or sustaining connections. This absence of technical difficulties may have occurred because the case worker was present to install and adjust the videophone equipment at each visit where it was used, because the connections were mostly in urban rather than rural areas, or because long distance carriers were seldom involved in the transmission. Our findings contrast with those of Cady et al. 25 and Day et al. 26 who reported videophone connection difficulties especially in rural areas where low bandwidth restricted the use.
While mobile videophones have been used successfully in medical applications, 27,28 there appear to have been no previous studies of mobile videophones used with psychiatric patients. Mobile videophones, carried to the home by experienced clinicians, do not rely on the ability of a psychiatric patient to install and adjust the equipment on their own. Mobile videophones are also attractive because a single unit can be used to service many patients, although obviously the units are not available to each patient when the case worker is not present.
It is notable that 29 of the 53 intensive case management patients lacked an ordinary telephone line necessary to receive videophone treatment. Thus, the increasingly popular use of mobile phones for personal communications represents a barrier to the application of videophones. No readily available mobile phone service would be practicable for 15–30 min-long videoconferences. Even if available, current patient privacy and security regulations would prohibit the use of such mobile phones for telemedicine. However, while current videophones cannot operate with mobile phone networks, the technology of mobile phones is evolving rapidly and video transmission is already being studied. 29 In addition, Internet-based phones are likely to provide alternatives to fixed telephone lines. 30
The present study was based on a small number of patients with serious mental illness. Further studies are required to clarify the role of videophones in psychiatry. Although our results are preliminary, they suggest time and cost savings for clinicians and patients, along with a high degree of acceptability in the setting of intensive case management with the seriously mentally ill. We believe that there are other potential uses of videophones in this patient population, including discharge planning, intensive post-discharge monitoring and transition to community life. The equipment is affordable, portable and well received by the patients.