
Abstract
A mobile telemedicine system, capable of transmitting video and audio simultaneously, was designed for consulting acute stroke patients remotely. It could use a wireless local area network (e.g. inside the hospital) or a mobile phone network (e.g. outside the hospital). When initiating a call, the sending unit chose a suitable encoding profile based on the measured data throughput, in order to allocate appropriate bit rates for video and audio transmission. The system was tested using a portable digital assistant (PDA) type phone and smart phone as receiving units. Video and audio recordings were made from five patients (two normal and three stroke patients) and then transmitted at different rates. Subjectively, both video and audio qualities improved as the data throughput increased. The physical findings, including facial droop, arm drift and abnormal speech, were observed remotely by four specialists according to the Cincinnati Pre-hospital Stroke Scale guideline. A comparison between the face-to-face method and the mobile telemedicine method showed that there were no discrepancies at bit rates of more than 400 kbit/s. We conclude that specialists could generally conduct remote consultations for stroke patients either using a public mobile network or a wireless LAN.
Introduction
The proper and timely management of acute stroke is important to minimize brain injury and maximize patient recovery. It is recommended that the emergency department (ED) personnel should attend to a patient with a suspected stroke within ten minutes of arrival at the ED. Furthermore, fibrinolytic treatment must be provided within a few hours of the onset of symptoms. 1 Acute stroke care in the ED should aim to minimize the delay in making a definite diagnosis and providing therapy. However, treatment can sometimes not be performed appropriately by ED staff, as patients often deny their symptoms and fail to recognize the signs of a stroke. Moreover, the signs and symptoms of a stroke may be subtle and difficult to identify. 1
In the care of patients with acute stroke, health-care professionals experienced in managing stroke can improve patient survival, functional outcomes and quality of life. 2 Moreover, they can play a critical role in determining which patients will be treated with fibrinolytic therapy and when to transfer patients to another hospital with a dedicated stroke unit. However, they often are not in the ED, and sometimes are even out of the hospital. Hence, a portable telemedicine unit with a wireless network interface may be an efficient means of linkage between patients in the ED and remote healthcare professionals, without the limitations normally associated with the movement of experienced healthcare professionals within or outside hospital.
The identification of a stroke patient normally requires both visual and auditory cues. Signs and symptoms include sudden weakness or numbness of the face, arm, or on one side of the body, sudden confusion, and trouble speaking or understanding. Typical physical findings include facial droop, arm drift and abnormal speech. 2 Hence, both video and audio information are necessary for remote patient observation. We have developed a portable telemedicine system, capable of transmitting video and audio simultaneously, which was designed for consulting acute stroke patients remotely. The present work describes a feasibility study of its use.
Portable telemedicine system
The system was designed to operate over both the in-hospital wireless LAN and the public mobile phone network. The design requirements were:
Simultaneous transmission of video and audio through secure communication; Ability to use a wireless LAN (inside the hospital) and a mobile phone network (outside the hospital); Capable of operating on a range of portable devices, including a portable digital assistant (PDA)-phone and a smart phone; Flexible compression of video and audio depending on the available network throughput.
A sending unit located at the ED compressed the patient's video and audio in order to transmit the compressed streaming data to a remote receiving unit for the health-care professional (see Figure 1). Windows Media Video 9 (Microsoft Co.) and Windows Media Audio 9 (Microsoft Co.) were used to compress video and audio, respectively.
3
Windows Media Player (WMP) 9 (Microsoft Co.)
4
was employed as a device-independent presentation platform for receiving units. WMP 9 presents video and audio simultaneously, and is operable on both desktop type computer systems and diverse mobile devices. Because of the popularity of WMP 9, any receiving unit supporting WMP 9 could be used for assessment of an acute stroke patient remotely, which eliminated the need to develop dedicated decoding software for video and audio presentation.
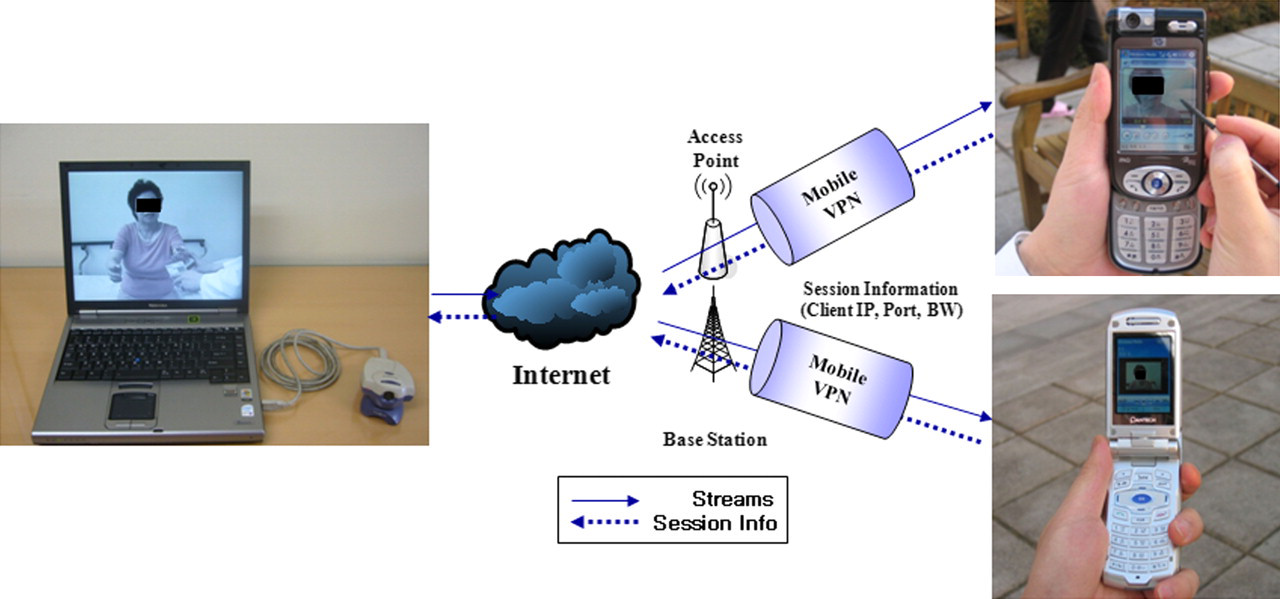
System architecture. The sending unit was a laptop near the patient in the emergency department. A portable device with wireless LAN and mobile phone network interfaces was used by a health-care professional as a receiving unit
A laptop computer was used at the ED as a sending unit to capture the video and audio of stroke patients.
Two types of handheld phones were employed as receiving units to provide the healthcare professional with mobility both inside and outside the hospital. They were a PDA-type phone (iPAQ rw6100, HP, USA) and a smart phone (PH-S 8000T, Pantech & Curitel, Korea). The display resolution of both devices was 240 x 320 pixels. The PDA-type phone employed the Pocket PC 2003 operating system with a stylus pen input interface, while the smart phone employed the Windows Mobile 2003 Smart Phone operating system with an input button interface. 5 Secure communication over a wireless network was performed by using a mobile virtual private network (VPN). Mobile VPN protects Internet protocol (IP) packets through an IP security protocol and tunnelling. 6
When the receiving unit attempted to connect to the sending unit, it first checked for the availability of a wireless LAN connection. If a wireless LAN connection was not available, it then connected to a mobile phone network. Connections through a wireless LAN are likely to provide more data throughput than those through a mobile phone network. While the connection was initiating, the receiving unit measured information about the session, including the available bandwidth, by transmitting dummy packets to the sending unit. After session setup, the sending unit obtained the measured throughput. The sending unit then selected a suitable encoding profile (see Table 1) based on the measured data throughput, in order to allocate appropriate bit rates for video and audio transmission.
Encoding profiles for video and audio compression
Methods
The sending unit was used in the Severance Hospital's emergency centre located in the central area of Seoul. There were 170 access points at the hospital, based on the 802.11 b protocol. The mobile network test was performed over a 2.5 generation network at a residential area, 20 km away from Severance Hospital. The network used Code Division Multiple Access 1x Evolution Data Only transmission. The measurements of the connection rates between the sending unit and mobile telemedicine system were made at 1 hour intervals from 09:00 to 21:00.
Encoding profiles
Nineteen different encoding profiles were designed by considering the data throughput in a typical mobile phone network (less than 1 Mbit/s) and a typical wireless LAN (less than 10 Mbit/s). This throughput range was divided uniformly, as shown in Table 1.
Clinical tests
Five patients (two normal and three stroke patients) were recruited to evaluate both the subjective quality and clinical efficacy of the proposed system. They provided written informed consent for the pilot study; ethics permission was not required. Three abnormal patients all had ischaemic lesions on brain MRI (a right anterior cerebral artery infarction, a right pontime infarction and a left striatocapsular infarction), but each patient had different levels of facial droop, arm drift and speech abnormalities as shown in Table 2.
CPSS screening results for the face-to-face method and the mobile telemedicine method for profile 4 and greater
The physical findings, including facial droop, arm drift, and abnormal speech, were observed remotely according to the CPSS (Cincinnati Pre-hospital Stroke Scale) guideline 2,7 for the assessment of acute stroke patients, as shown in Figure 2. Patients were asked to show teeth while smiling to evaluate facial droop; to extend their arms to 90 degrees (palms up) and hold them up with their eyes closed for 10 s to evaluate arm drift, and to repeat a given sentence twice to detect abnormal speech (‘Oh Neoul Eun Nal Shi Ga Cham Jo Sum Ni Da’; ‘It's lovely weather today’ in Korean).

The physical signs in the assessment of acute stroke patients included (a) facial droop, (b) arm drift and (c) abnormal speech
Clinical tests were performed by four specialists (two neurologists and two emergency physicians). First, original video and audio for abnormal patients were recorded and then compressed for subjective quality assessment. The decompressed quality of the video and audio for different encoding profiles (i.e. using different compression ratios according to the different bitrates of the networks) was evaluated using a 5-point Mean Opinion Scores [MOS] scale (1 = worst to 5 = best). Second, clinical tests for all five patients were performed to demonstrate the clinical efficacy of the proposed mobile telemedicine method in comparison with the face-to-face (patient-to-specialist) method according to the CPSS guideline. Four specialists compared the screening results between two methods, C (correspondence between two methods) and D (discrepancy between two methods), as shown in Tables 2 and 3.
Agreement between the face-to-face method and the mobile telemedicine method for profiles 1 to 4. C = Correspondence observed between the two methods, D = Discrepancy observed between the two methods. The patient identification number is shown in parentheses
Results
The system was tested using a PDA-type phone and smart phone, as shown in Figure 3. Both receiving units were able to present satisfactory video for the observation of facial droop and arm movement, and provide satisfactory audio for the detection of abnormal speech.

The system was tested using a PDA-type phone and smart phone: (a) normal and (b) full screen views on a PDA phone; (c) normal and (d) full screen views on a smart phone
Quality evaluations
Both video and audio qualities improved as the data throughput increased (i.e. as the encoding profile number increased) (see Table 4). The audio quality scores were more than 4 for all encoding profiles, except profile 1. The lowest audio bitrates of 32 kbit/s for profiles 1, 2 and 3 provided understandable speech. In contrast, the video bitrates in profiles 1, 2 and 3 were not high enough to allow the specialists to assess the stroke patients without difficulty. Profiles 4, 5, 6 and 7 were satisfactory, even though slight differences between the original video and the decompressed video were observed. Profile 8 and greater provided satisfactory video quality of the stroke patients without discernible quality differences. That is, profile 4 and greater (more than 400 kbit/s) would be preferred for remote access to a stroke patient.
Mean (n = 15) video and audio scores (1 = worst to 5 = best)
Clinical evaluations
The comparison between the face-to-face method and the mobile telemedicine method showed that there were no discrepancies for profile 4 and greater (corresponding to bitrates of more than 400 kbit/s), as shown in Table 2. In other words, if the available bandwidth of a mobile phone network was more than 400 kbit/s, the proposed method could be used to screen stroke patients regardless of their level of abnormality.
In order to compare the CPSS screening performance between the two methods when the available bitrates of the mobile phone network was low, clinical tests were conducted for profiles from 1 to 4, as shown in Table 3. Some discrepancies were found between the two methods, especially for profiles 1 and 2 (available bitrates of less than 200 kbit/s). That is, for patients 3 and 4 showing minor levels of abnormality in facial droop, the mobile telemedicine method could not screen the stroke correctly using encoding profiles 1 and 2, as the differences between mild symptoms (a flattened nasolabial fold and asymmetry on smiling) and the normal state (a symmetrical movement) were difficult to identify at low bitrates due to the poor quality of the received video with frequent frame dropping and a blurring effect. However, in the case of a severe level of abnormality in facial droop (patient 5), there was no difference between the two methods using profile 1 and 2, because the distinct pattern of facial droop could be recognized in spite of the poor quality of the patient video. Similarly, no discrepancies were observed for normal cases of facial droop (patients 1 and 2).
As for arm drift and abnormal speech, no discrepancies were observed irrespective of the level of abnormalities (including the normal, the minor and the severe). The distinct pattern of arm drift (the distinction between minor drift of the motor arm and some efforts against gravity for the motor arm) could be easily recognized even at low video quality. In addition, allocated audio bitrates of 32 kbit/s for profiles 1, 2 and 3 (refer to Table 1) did not disrupt the screening of abnormal speech, including mild-to-moderate dysarthria and severe dysarthria.
Connection tests
The number of connection tests conducted over the mobile phone network are shown in Table 5. The measured connection rates from profile 3 to profile 7 (more than 300 kbit/s) were present for 92% of the total measurement duration. However, connection rates for profiles 1 and 2 (corresponding to clinically unacceptable qualities) were less than 8%. That is, acceptable video and audio qualities could be maintained except at low bandwidth. From these observations, we conclude that specialists could generally conduct remote consultation over a public mobile network. Regarding the wireless LAN connection, all measured throughput rates were more than 500 kbit/s. Thus, the system could provide acceptable video and audio quality using the wireless LAN in the hospital.
The number of times each profile was tested using the mobile phone network (profiles 11–19 were used for wireless LAN operation, i.e. inside the hospital)
Discussion
Simultaneous transmission of both video and audio data is essential to remote specialists in evaluating acute stroke. A patient's difficulty in speaking and understanding cannot be judged by video information alone; numbness of the face and arm cannot be judged by sound information alone. Simultaneous video and audio transmission can be accomplished using multimedia technology. However, most multimedia telemedicine systems use desktop or laptop computers, 8-10 which are not appropriate during movement. Therefore, a handheld type telemedicine device, capable of transmitting video and audio simultaneously over a wireless network, is likely to be useful for diagnosing patients remotely, particularly stroke patients. It could reduce the time to treatment and speed up clinical decisions. However, such portable, mobile telemedicine devices are not commonly available for stroke assessment.
When expert consultation is required, healthcare professionals are often not available in the ED. They are sometimes in other areas within the hospital and sometimes outside of the hospital. Hence, the support of both a wireless LAN (within the hospital) and a mobile network (outside the hospital) is essential to permit healthcare specialists to move anywhere. Operability via various mobile phone networks should also be considered. It is now common for people to carry sophisticated mobile phones, including PDAs and smart phones. Finally, the tolerance of throughput variability of the wireless network is important. The system we have designed can cope with network heterogeneity to some extent by means of the multi-profile bit assignment scheme.
In conclusion, a mobile telemedicine system, capable of transmitting video and audio simultaneously, was designed for consulting acute stroke patients remotely. By employing a wireless LAN or a mobile phone network, the telemedicine system could be operated anywhere inside or outside the hospital. The combination of popular media streaming technology with a multi-profile bit assignment scheme coped successfully with the heterogeneous throughput of the mobile phone network. The system could therefore be used with a range of handheld devices, including PDAs and smart phones.
Footnotes
Acknowledgements
This study was supported by a grant of the Korea Health 21 R & D Project, Ministry of Health and Welfare, Republic of Korea (A020608), and this research was financially supported by the Ministry of Knowledge Economy (MKE) and Korea Industrial Technology Foundation (KOTEF) through the Human Resource Training Project for Strategic Technology.