
Abstract
In 1999 we introduced a digital, mobile eye fundus camera for screening type 2 diabetes mellitus patients (adult onset diabetes) in the Finnish county of South-Ostrobothnia. Prior to this, eye fundus examinations were only available in the regional central hospital, and no systematic screening of type 2 (adult onset) diabetes patients was possible. The total number of screenings carried out with the mobile equipment from 1999 to 2006 was 17,471 cases. There were significant benefits, most important from improved coverage of type 2 diabetes patients. Because the mobile system made eye fundus examinations available to patients in their nearest health centre, approximately 85% of all patients with diabetes in the region are now screened. On average this means that each patient is screened once every 2.5 years, which is in line with national recommendations. As a result, more of the earlier stage retinopathy cases have been diagnosed. There have also been changes in the frequency and type of procedures at the eye department of the regional central hospital. The number of cases referred to the eye department for follow-up studies has decreased from 49 in 2000 to 19 in 2005. The screening system adopted in South-Ostrobothnia has had beneficial effects for both patients and health-care providers.
Introduction
Diabetic retinopathy is caused by lesions in the retina of individuals who have had diabetes mellitus for several years. 1 Diabetic retinopathy is the most common diabetic eye disease and a leading cause of blindness in adults in industrialized countries. 2
The less severe form of diabetic retinopathy, non-proliferative retinopathy, involves physical changes in the retina that often go unnoticed by the patient. At the earliest phase of non-proliferative retinopathy, microaneurysms in the retina occur. 1 If the disease progresses to the more severe form, proliferative retinopathy, the signals sent by the retina for nourishment trigger the growth of new blood vessels. These new blood vessels are abnormal and fragile. If they leak blood, severe vision loss and even blindness can result. 1
The prevalence of diabetes, and hence diabetic retinopathy, is increasing worldwide. In 1990, the World Health Organization (WHO) estimated that 135 million people worldwide had diabetes. By 2000 this figure had risen to 171 million, and by 2030 it is expected to be at least 366 million. 3
In Finland the prevalence of diabetes is approximately 9.5% of the population, which represents some 500,000 cases. 4 In the US, the number of new cases of diabetes diagnosed in people aged 20 years or older is 1.3 million per year; diabetic retinopathy causes 12,000 to 24,000 new cases of blindness yearly. 2 In Britain, it is estimated that the annual incidence of blindness among diabetics with retinopathy requiring treatment is 6–9%. 5
Retinal screening
Screening of diabetes patients is very important because it has been shown that blindness from diabetic retinopathy is largely preventable, provided routine screening examinations are carried out. 2,5,6 Screening can also improve the efficiency of ophthalmology services and reduce the number of patients referred to the eye clinic. 7
According to Finnish national recommendations, the eye fundus (retina) of every diabetic patient should be screened at least once every three years (Table 1). 8 However, practical limitations and lack of resources often make it impossible to adhere to these recommendations.
Recommended screening frequency in Finland of diabetic patients in case of normal findings 8
The development and use of portable digital equipment has enabled a profound change in the screening process. It has been transformed from a centralised, hospital-based system, to one involving secondary level care provider organisations.
We have introduced a digital, mobile eye fundus camera for screening type 2 diabetes mellitus patients (adult onset diabetes) in the Finnish county of South-Ostrobothnia. The present study was conducted in order to examine the effect of the screening system on both patients and care providers.
Retinal examinations prior to 1999
Prior to 1999, diabetic retinopathy suspicions in the Finnish county of South-Ostrobothnia were referred to the regional central hospital, the Seinäjoki Central Hospital (SCH), which is the only hospital in the county that provides secondary and specialised level care. The total population of the county is approximately 200,000.
Retinal examinations in the hospital were mainly based on traditional 35 mm film retinal photography. Although film-based retinal photography is an established and well-documented method, it has several limitations. It is labour and resource intensive, requires a skilled photographer, involves high cost of film developing and handling, and often involves delays in film processing. 9 Hence the hospital was unable to provide adequate screening services for all type 2 diabetes mellitus patients in the county. Only diabetic retinopathy suspicions referred to the hospital from secondary care or general practitioners were carried out, and no systematic screening of type 2 diabetes patients was possible.
Consequently, a project was commenced in 1999 to develop a screening system based on digital camera technology that would enable the extension of retinal screening to as large a proportion of the county's patients with type 2 diabetes as possible.
The hospital decided to replace the film-based retinal camera with two digital cameras, one of which would be transportable, so that screening studies could be carried out in the county's health-care centres. One fixed digital retinal camera would remain at the hospital for follow-up and routine hospital use.
At the time several digital fundus camera systems were commercially available, but they were not intended to be easily transportable. It was decided therefore to purchase and modify an existing system with the help of the system vendor and software designer.
Digital screening equipment installed in 1999
The equipment purchased consisted of two digital fundus cameras that were connected to a network server, where the digital images were stored. The mobile system consisted of a PC, imaging software (EyeCap, Haag-Streit Co, Harlow, UK) and a retinal camera. The camera (Canon CR 6–45 non-mydriatic retinal camera) was able to record JPEG/TIF images at a resolution of 1024 × 768 pixels.
Modifications to the original equipment involved changes to both hardware and software. The software changes enabled archiving of data from the mobile system, as well as the use of a CD station for data storage and back-up directly from the imaging software. Hardware changes included changing plugs, leads and electric connections to more robust components that could better withstand repeated connections/ disconnections and the construction of carrying cases for the system.
The portable equipment with its carrying cases is shown in Figure 1. Each carrying case was designed to be light enough to be handled by a single person. Figure 2 shows the hospital system in use.

Mobile digital fundus camera system with transport equipment. The fundus camera and computer are on the desk, and the transport cases for the equipment are underneath
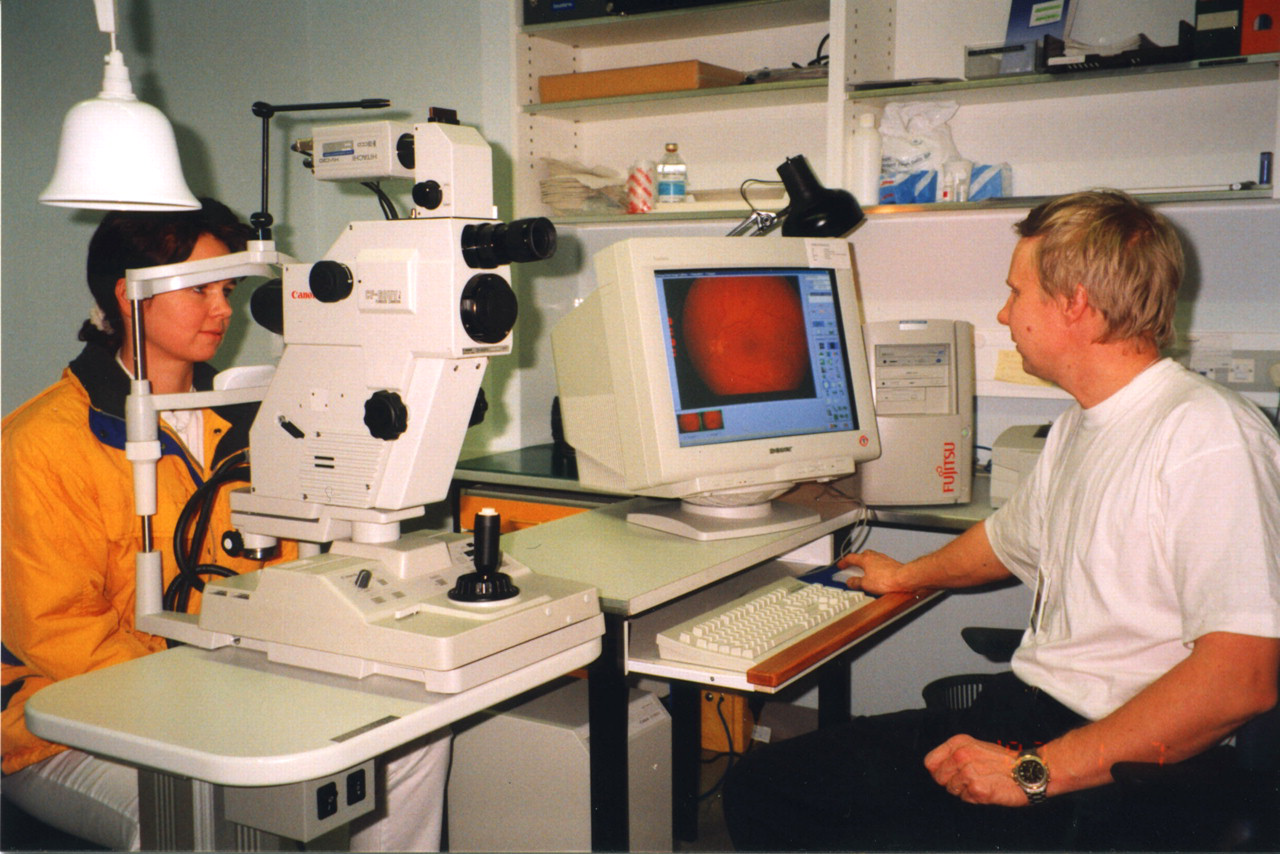
Fundus camera and computer used at Seinäjoki Central Hospital
Screening process
The resident physician at the local health centre is in charge of the care of diabetes patients living in the catchment area of the health centre and prioritises the screening of the diabetes patients. The diabetes nurse and office personnel of the health centre support the screening and make appointments. At the specialised care level the ophthalmologist of the SCH evaluates abnormal images and plans the care of the patient.
A nurse from the SCH is in charge of the mobile equipment and also of carrying out the actual screening study. The nurse transports the screening equipment to the health centre and captures the images. Before screening, the pupils of the patient are dilated with eye drops (tropicamide) because application of tropicamide 1% solution clearly improves the quality of images taken with a nonmydriatic camera. 10
After the images have been taken, they can be viewed immediately on the computer display with the viewing software Eyecap. The nurse will carry out the initial scoring of the image, as to whether the finding is normal or not. She is also responsible for the storage of the image files on the hospital's data bank. Final scoring is done by the ophthalmologist at the SCH. The screening process is summarised in Figure 3.
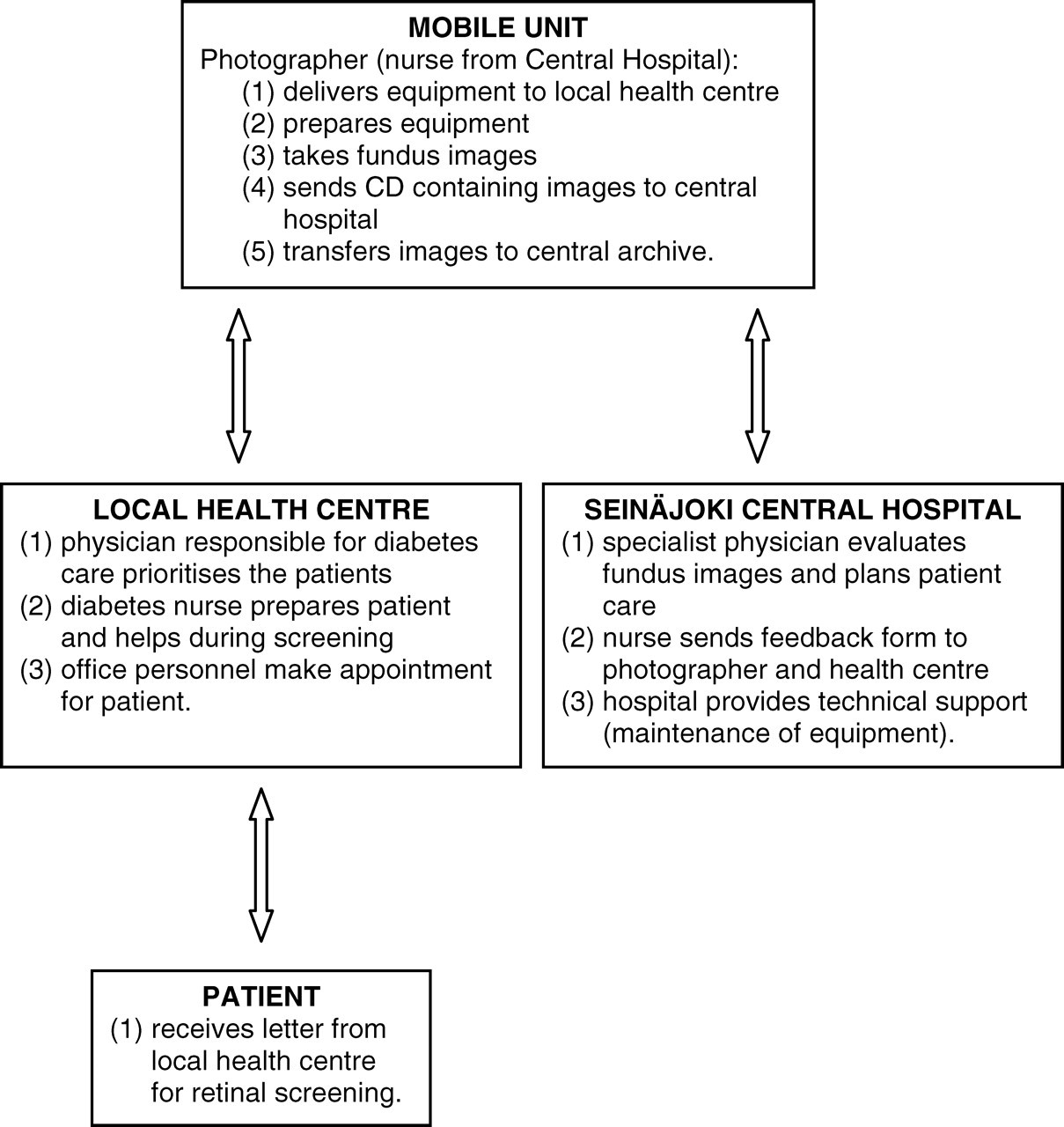
Flow chart of the mobile diabetic retinopathy screening system
Only the images with clear abnormalities are referred to the eye clinic of the SCH for further action. Those with normal findings and slight changes are diagnosed by the photographing nurse. The training of the nurse who takes the images is therefore a very important matter.
Patient questionnaire
During the initial stages of the screening service, the first 150 patients were asked to complete a questionnaire regarding the quality of the new screening service using a scale of 1 = poor to 5 = excellent. They were also asked to rate how important it was for them to have the screening service at their nearest health centre using a scale of 1 = not very important to 5 = very important.
Screening experience
The total number of screenings carried out with the mobile equipment from 1999 to 2006 was 17,471 cases. The number of patients screened per year (2004–2006) was approximately 3000. According to the statistics of the social insurance institution of Finland, there were 8292 cases in the region in 2006. On average this means that each patient is screened once every 2.5 years, which conforms with national recommendations (Table 1). The number of cases referred to the eye department for follow-up studies decreased from 49 in 2000 to 19 in 2005 (Table 2).
Number of screenings and diagnoses performed by mobile diabetic retinopathy system in South-Ostrobothnia during 2000–2006
A subsequent increase back to 53 patients in 2006 was due to changes in staff – the scoring of retinal images was performed by a trained ophthalmologist until 2005, when a more junior doctor with less experience took up the duties. This shows the effect of the process on staff learning and competence, and the reduction in patient load in the clinic achievable by a sufficiently trained physician. This training was made possible by the new system that allowed a sufficient number of studies, and hence encouraged the training process.
On the other hand, the annual number of glaucoma and cataract findings has increased from approximately 50 cases in 2000 to more than 120 cases in 2004, 2005 and 2006.
The incidence of diabetic proliferative and non-proliferative diabetic retinopathy and the total incidence of diabetic blindness in the population of South-Ostrobothnia were obtained from the Finnish Federation of the Visually Impaired, National Research and Development Centre for Welfare and Health (Table 3). Blindness was defined as patients suffering Category 3 to 5 stage visual impairment, as defined by the WHO 5-point scale for visual impairment. On this scale, Category 3 indicates visual acuity of less than 1/20 and Category 5 is defined as complete loss of all visual sensation. 3
Total number of patients with diabetic retinopathy and blindness in South-Ostrobothina 11
Patient feedback
In total 132 responses were obtained in the patient survey, i.e. a response rate of 88%. The average score for service quality was 4.8, indicating that the patients were overall very satisfied with the new screening method. The average score for the question dealing with the proximity of the service was 4.9, confirming that patients clearly preferred to have the screening available at their nearest health centre.
Discussion
A significant body of research exists on the evaluation of tele-screening methods or remote diagnostic methods of diabetic retinopathy 12–22 but less research is available on the extent of coverage or of the actual effects of diabetes screening. 2,23 The present study shows that the screening system adopted in South-Ostrobothnia has had beneficial effects on both patients and health-care providers.
The mobile system has made possible screenings that could not have been conducted at the central hospital. Before the establishment of the mobile system, only patients with type 1 diabetes were screened. As there was no systematic screening of those with type 2 diabetes prior to the system described here, the coverage of the diabetic screening in the South-Ostrobothnia improved dramatically. In addition, the patients are very satisfied with the mobile system because they prefer to be screened at the local health centre rather than at the central hospital. Similar findings have been reported elsewhere: according to the research conducted in Scotland, the majority of patients preferred to obtain diabetic care and reviews at their general practice rather than at the hospital. 12
Diagnosis of non-proliferative retinopathy has increased since the screening began. It can be presumed that patients may not be aware in the earlier stages of the disease of deteriorating retinal function, and hence they were only occasionally referred for diagnosis to the central hospital prior to 1999. As screening started, more of the earlier stage diabetic retinopathy cases were diagnosed. This can enhance patients' quality of life because symptoms can be detected at the earlier phase of the disease, thus reducing not only the severity of illness, but possibly making the treatment less invasive and thus easier for the patient.
The prevalence of blindness in the county has been reduced from 10 to 9 cases, but since the total numbers involved are small, this change cannot be considered significant. However, it can be argued that the effects of the screening process are notable in the earlier detection of retinopathy, as indicated by the increased clinical diagnosis of non-proliferative retinopathy, and that the incidence of blindness due to diabetic retinopathy in the population has not increased.
The effects of introducing the digital screening system were also evident in the changes in frequency and type of procedures at the eye department of the SCH. The increase in scoring expertise by the ophthalmologist was clearly shown by the reduction in the number of cases referred to follow-up studies at the department of ophthalmology until 2006. The workload of the department thus also decreased steadily until 2006. That is, as doctors saw more cases, they became more proficient at diagnosis based on retinal images. Hence the number of patients that had to be recalled to the hospital for more extensive studies decreased. The situation changed in 2006 when the responsibility for diagnosis based on retinal images was transferred to a more junior doctor with little previous experience of retinal diagnosis based on fundus images only. Hence more patients were recalled to the hospital in 2006 for additional examinations.
In the future, the efficiency and reliability of diabetic retinopathy screening may be improved with advanced computational systems, such as automated microaneurysm detection or other automatic decision support methods. Automatic image grading methods could improve the cost-efficiency of diabetic retinopathy screening. For example, the automated detection of microaneurysms performed with contrast normalization has been demonstrated to be effective. 24 It might also be possible to improve the cost-efficiency of screening with the implementation of teleretinal imaging methods. This kind of new national-level telemedicine framework using teleretinal imaging has been examined by the Veterans Health Administration in the US. 22 Inspection and grading of retinal images with tele-ophthalmology methods have also been found suitable for remote screening. 21
Conclusions
The development and use of mobile digital retinal imaging technology has enabled a profound change in the screening process of diabetes patients from a centralised, hospital-based system, to one involving secondary level care provider organisations. This has made possible comprehensive screening of a significant proportion of diabetes patients in a large, rural county. As a result, more of the earlier stage retinopathy cases have been diagnosed. The benefits of the system are also evident in the changes in frequency and type of procedures at the eye department of the regional central hospital.
Footnotes
Acknowledgements
We thank the South-Ostrobothnia Hospital District and Dr Eeva Orhanen for providing information for this paper. We also thank Kaarina Kosola and Jaana Hietala for their help in data collection.