
Abstract
We conducted a retrospective study of symptom assessment calls for adult patients at a US call centre, Ask Mayo Clinic. A total of 27,979 symptom assessment calls were received from July 2006 to June 2007. Calls concerning female patients predominated in all age groups and accounted for 71% of calls, but decreased significantly with increasing age. The average duration of an adult call was 10 min, and the duration increased with increasing age of the adult patient. The greatest frequency (8%) of calls were related to symptoms of abdominal pain, followed in frequency by skin problems (6%), pregnancy-related issues (6%), cold symptoms (4%), and chest pain or chest discomfort (4%). Surrogate calls accounted for 14% of adult calls but the proportion was significantly higher (40%) if the patient's age was 80 years or greater. Call centres should recognize the sex- and age-related trends in calls and adjust the training of their registered nurses accordingly.
Introduction
An increasing number of adults use telephone call centres to obtain health-related information, especially in the UK, Australia, Denmark and the Netherlands, where telephone advice is available for all citizens. 1 In England, the National Health Service (NHS) has NHS Direct, a 24-hour health information service accessed by telephone, the Internet and digital TV. In 2006, NHS Direct answered 6.8 million telephone calls, the majority of which were about adults. 2 In Australia, the HealthDirect call centre handles telephone triage calls throughout much of the country. 3,4 Similarly, Denmark and the Netherlands also offer telephone triage to a large segment of their population. 5 Finland is developing regional call centres. 6
The US does not have government-sponsored national telephone triage access. However, an increasing number of US adult patients use the telephone for advice and triage purposes. An estimated 100 million people have access to telephone triage in the US. 7 Although most of the published US experience with triage calls concerns calls related to children, some adult data from a large US call centre have been published recently. Conolly et al. 8 examined the calls from the Permanente Medical Group (PMG), a US call centre, that included all age groups and averaged one million calls per month. In their analysis, Conolly et al. described important characteristics of adult calls, including call demographics and the temporal distribution of the calls. Conolly et al. also ranked by frequency the clinical concerns of PMG callers and showed that these rankings varied with caller age. However, the PMG study did not analyze any age-related trends.
Despite the growth of adult telephone triage, little information has been published on how the characteristics of calls concerning adults vary with age. This knowledge is important for development of cost-effective triage systems. Information about age-related trends in calls may also be helpful in call centre staff development. Knowledge of trends in the types of adult calls may help to identify staff training needs, for example, in areas of geriatric health complaints.
The primary objective of the present study was to determine age-related trends among adults who use a triage call centre. Additional aims were to determine the frequency of caller medical concerns and the distribution of callers by sex and age.
Methods
All symptom assessment calls that were made from July 2006 through June 2007 to Ask Mayo Clinic, based in Rochester, Minnesota, were used in the analysis unless otherwise stated. The study was approved by the appropriate ethics committee.
Ask Mayo Clinic
Ask Mayo Clinic is a nurse-staffed telephone triage call centre that handles more than 80,000 calls per year. More than half of the calls are about symptom assessment. Most calls that are not about symptom assessment are requests for information about specific diseases. Access to Ask Mayo Clinic is by subscription only. Subscribers are generally medium- to large-sized corporations located in the US. These corporations purchase the triage service on behalf of their employees and their dependents. In addition, some US health insurance companies subscribe to the service. About two million people have access to Ask Mayo Clinic triage call centre advice.
The call centre has a staff of 41 registered nurses who each have, on average, 20 years of nursing experience. All nurses receive special training in both triage technique and use of triage software. Nurse supervisors also regularly review actual call audio recordings.
The call centre uses proprietary software (Expert RN) on an Expert-24 platform that has 41 symptom-based algorithms which are supplemented with an additional 79 computerized guidelines. 9 Of these 120 algorithms and guidelines, 105 are used for adults. Triage nurses use 38 distinct symptom- and concern-related algorithms and 67 distinct guidelines for decision support of the adult calls. The algorithms and guidelines are constructed and modified in-house. The software captures information about each call.
Data collection
Call durations were inclusive of all aspects of the call, including intake of caller and client information, time of triage, time of advice, time of any assistance with air or ground transport or other medical access help, and call wrap-up. The call documentation time was also included in the call duration data. We divided the telephone callers into either the self or the surrogate category, depending on whether they were calling about their own symptom or that of a dependent. For the purposes of the study, a patient was defined as the person who was the subject of the call. The time of call was collapsed into three 8-hour periods: daytime calls, from 08:00 to 16:00; evening calls, from 16:00 to midnight; and night calls, from midnight to 08:00.
Statistical analysis
Statistical analysis was performed using JMP 6.0 and SAS 9.1.3 (SAS Institute, Cary, North Carolina). The Cochran-Armitage test for trend (Z statistic) was used for categorical age-group trend analysis. 10 For calls that were not classified into one of the 105 software symptom or concern categories, we performed call record abstraction to discern the underlying reason for the call. We performed abstraction on 100 records (20 records randomly chosen from each of the 5 age-group categories).
Results
During the 12-month study, Ask Mayo Clinic received 42,757 symptom-related calls. Of these calls, 27,979 (65%) concerned symptoms of adults (aged 18 years and older). Further data in this paper refer only to the 27,979 adult calls.
English was the language spoken in 97% of adult calls. The calls for patients aged 18–34 years accounted for 47% of all adult calls, followed in frequency by calls for the age-groups of 35–49 years (24%), of 50–64 years (17%), of 65–79 years (8%), and of 80 years and older (3%). There was a significant downward trend in call volume as age increased (P < 0.001). Calls concerning women predominated in all adult age-groups (Figure 1) and accounted for 71% (19,782) of calls. The proportion of calls related to women was highest (77%) in the age-group of 18–34 years; it was lowest (58%) in the age-group of 65–79 years. There was a significant downward trend in calls about female patients as age increased (P < 0.001).
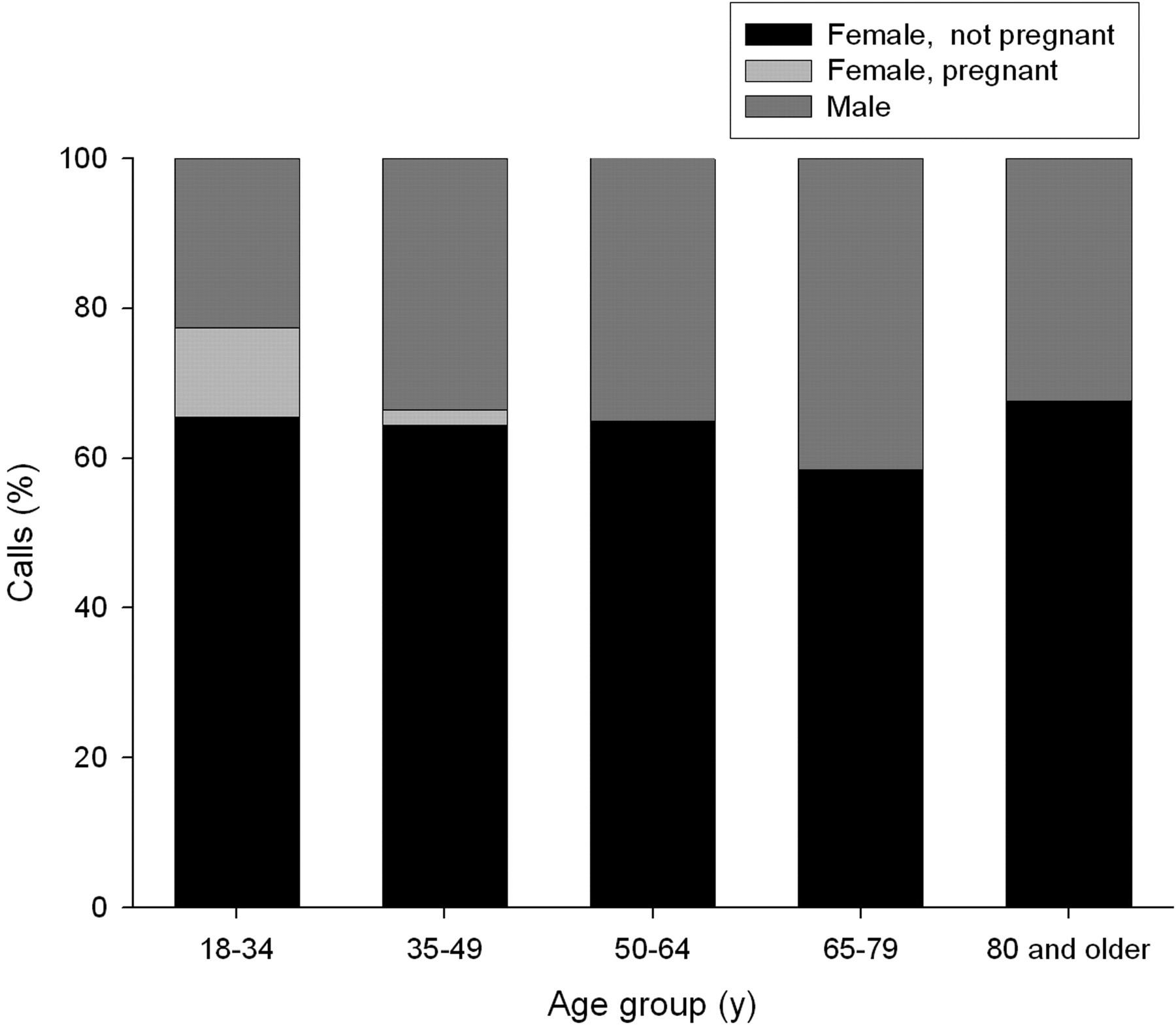
Percentage of calls according to sex and age-group
Surrogate calls accounted for 14% (3812) of adult calls. They comprised 11% of calls about adults aged 18–64 years, increasing to 40% in the age-group of 80 years and older. Unlike the female predominance of self-calls, surrogate calls were about men 59% of the time, for patients aged 35–79 years.
Call volumes relative to time of day showed strong trends by increasing age. There was a significant trend for calls related to older patients to occur during the daytime (P < 0.001) (Figure 2). Older patients also called more frequently at weekends than younger patients did (P < 0.001).

Time of day when calls occurred according to age-group
The mean call duration was 10 min (SD 6). The call duration distribution was skewed, with 220 calls (0.8%) longer than 30 min. Call duration showed a significant linear relationship with increasing age. There was a 1.4-min increase in call duration from the youngest adult age-group (18–34 years) to the oldest (80 years and older) (Figure 3).

Duration of calls (and 95% CI) according to age-group
The highest frequency of calls (8%, or 2195 calls) were related to symptoms of abdominal pain, followed in frequency by skin problems (6%), pregnancy-related issues (6%), cold symptoms (4%), and chest pain or chest discomfort (4%) (Table 1). A significant downward trend in calls about women occurred with increasing age, even when pregnancy-related calls were excluded (P < 0.001).
Frequency and rank of call concern by age-group
ai.e. the concern did not fit into an algorithm or guideline
Fifteen caller concerns positively correlated with increasing age (Table 2). Caller concerns with the highest odds ratios (ORs) in the age-group of 80 years and older were those related to high blood pressure (OR, 52.7), confusion (OR, 17.4), asymptomatic blood glucose concerns (OR, 12.4), pedal oedema (OR, 9.2) and constipation (OR, 6.8).
Caller concerns that were positively correlated (P < 0.001) with increasing age
aAsterisk indicates odds ratio greater than 1.0 at the 95% confidence level
Of the adult calls, 4% or 1091 calls did not fit into an algorithm or a guideline and were placed in an ‘other’ category. Post-hospitalization and post-procedural concerns accounted for 16% of ‘other’ calls. Additional reasons for the ‘other’ calls included questions about medications, which were questions specifically about dosage concerns related to accidental medication overdose or to missing a dose (27%), vague symptoms not further classified (20%) or those misclassified (16%), chemical exposure (11%) and chills without fever (10%).
Discussion
In the present study, calls about women dominated in all adult age-groups but decreased significantly with increasing age; the highest frequency of female calls was in the age-group of 18–34 years. Although pregnancy-related calls accounted for a large proportion of calls about women in the younger adult ages, a significant downward trend in calls about women persisted even when pregnancy-related calls were excluded. This predominance of female calls was similar to that observed in other studies. 8,11 The age-related sex trend was also similar to that in office visits in the US, where women account for 61% of visits. 12 Call centres should recognize this sex predominance in calls and adjust the training of their registered nurses accordingly.
Of the top 20 call reasons, 70% showed significant trends with aging. Many of these trends were expected because of the natural history of the underlying causes for the symptoms. Positive correlations of call concerns with increasing age were primarily seen in calls about high blood pressure, confusion, asymptomatic blood glucose concerns, pedal oedema and constipation. Other high-ranking call concerns, such as those about skin, cold symptoms and painful urination, showed no trend with age. Two of the strongest positive correlations with age were associated with home-use measuring devices (blood pressure and glucose). These findings suggest the value of a call centre in chronic-disease management support. Our results were congruent with telephone and computer-assisted management of chronic disease in New Zealand and Australia. 13
A UK call centre found that specialist nurses (registered paediatric nurses) using computerized guidelines had shorter paediatric call durations than non-specialist registered nurses using the same program. 14 Based on this finding, it is possible that increased training in geriatrics for nurses might reduce some of the increased call durations that we found in calls made about the older patients.
We found that, as in other call centres, the call volume of Ask Mayo Clinic varied significantly with time of day and day of week. 8,15 The greatest proportion of calls occurred during evening hours and at weekends. Calls between 08:00 and midnight showed strong trends according to age. Adults younger than 50 years were more likely to call during the evening (16:00 to midnight) than during the day (08:00 to 16:00). People aged 50 years and older were more likely to call during the day. A probable explanation for these trends is that younger adults prefer to call after work.
The mean call duration of our adult-related calls was 10 min, a length similar to that at other centres using computerized algorithms. NHS Direct, which uses such algorithms, averages 11 min per call. 16 Call duration increased with increasing age of the patient. Because call centre costs are partly dependent on call duration, this finding is relevant to the financial planning of call centres. 17
Although we found a significant increase in call duration with increasing age of the patient, age explained only a small fraction of the call duration variability (R2 = 0.0055). Other factors appear to be more important contributors to differences in call length. For example, a major US paediatric call centre with more than 30 million subscribers, 500 nurse employees and a physician-designed clinical guideline system had an average call length of 14.5 min, but paediatricians in the same study taking similar calls were on the telephone for only 4.8 min. 18 This difference in call length between two different systems of triage (9.7 min) is much greater than the 1.4 min difference we found between patient age groups. More study is needed to explain call length differences between triage systems as well as within the same system.
When comparing call durations from different call centres, it is also important to know whether the reported call durations include all aspects of call-related work or simply time on the telephone. The published literature is not always clear on what is included in the call duration. O'Cathain et al. 19 have pointed out that both the call wrap-up and the collection of intake information contribute to call duration. Our call durations included all aspects of the calls from start to finish, including documentation after the conclusion of the call. Some of our callers were assisted with timely access to medical facilities after their symptoms were assessed. This assistance with ground or air transport was an additional service component of the call. Nurses kept the line open while arranging for emergency transport, sometimes calling other countries to make these arrangements. Ong et al. 20 pointed out the contribution of telephone advice to the call duration. It is important that call centre studies state exactly what is included in their call duration data.
The Ask Mayo Clinic data for adult caller concerns showed significant differences compared with the published data from another US call centre, PMG in California. PMG consistently ranks abdominal and chest pain in the bottom 5 of its top 10 reasons for adult calls. 8 Among Mayo callers, abdominal pain and chest pain consistently rank in the top five reasons for adult calls. Part of this difference may be explained by differences in service offered by the two call centres. For example, medication refills were the most common reason for calls to the PMG centre, while prescription refills were not available via the Ask Mayo Clinic service line.
Beyond this service difference, we believe that a more fundamental reason underlies the difference in caller concerns between Ask Mayo Clinic and PMG. The appointment and advice call centre at PMG served as the ‘front office’ for primary care services in Northern California. In contrast, Ask Mayo Clinic does not directly take appointments. Instead, it assesses symptoms and gives recommendations to patients who may have varied levels of access to medical care across the US. We know that Ask Mayo Clinic callers had a high sense of urgency because a large number of calls were about their acute symptoms. Of adult callers, 16% intended to seek emergency care if they did not have access to Ask Mayo Clinic (of 27,770 callers, 4469 intended to go to an emergency department or call an ambulance). From this perspective, the Ask Mayo Clinic caller concerns may be more similar to those of emergency department visits than to office calls or even to another call centre. National data tends to support this hypothesis. Abdominal pain and chest pain were the number 1 and number 2 reasons for adult emergency department visits in the US in 2005, similar to the ranking with Ask Mayo Clinic calls. 21
The proportion of calls from surrogates increased significantly for patients older than 65 years. Surrogate calls accounted for about 40% of the total calls for adults aged 80 years and older. Because frailty and cognitive problems occur more often in older patients than in younger patients, this finding was expected in this age-group. However, it is interesting to note that surrogate calls still accounted for a significant proportion of calls in younger adults (11%) and showed no significant trend between ages 18 years and 65 years. Little research has been done to examine these surrogate calls in detail. Our research suggests that surrogate calls for persons aged 65 and older are associated with more urgent conditions and receive a higher frequency of emergency triage recommendations than calls made by patients themselves. 22
It may not be possible to generalize the results of the present study to other call centres because of demographic and call centre service differences. Ask Mayo Clinic is accessible only to callers who are associated with a paid subscriber having access to the call centre telephone triage line. Most callers were employees (and their dependents) of companies that subscribed to the service.
Access to call centres is increasing worldwide. Call centres are experiencing an increasing demand for advice about adults. Knowledge of age-related trends can help call centres plan software development, staffing and training to meet the increasing demand for telephone advice.
Footnotes
Acknowledgments
We thank Barbara L Kreinbring, LeTesha D Montgomery, Robert J Stroebel and Sidna M Tulledge-Scheitel for their support, and Christopher Kaspar for help with data preparation.