
Abstract
We studied a web-based triage system which was accessible to the general public in the Netherlands. In a retrospective analysis we investigated the type of complaints that were submitted and the kind of advice provided. Over a period of 15 months, 13,133 different people began using the web-based triage system and 3812 patients went right through the triage process to the end. The most frequent complaints were common cold symptoms, such as cough and a sore throat (22%), itch problems (13%), urinary complaints (12%), diarrhoea (10%), headache (8%) and lower back pain (8%). Most commonly, the system generated the advice to contact a doctor (85%) and in 15% of the cases the system provided fully automated, problem-tailored, self-care advice. A total of 192 patients participated in a prospective study and completed an online survey immediately after the delivery of advice. A follow-up questionnaire on actual compliance was completed by 35 patients. Among these, 20 (57%) had actually complied with the advice provided by the system. A regression analysis revealed that intention to comply was strongly related to actual compliance. In turn, intention to comply was strongly related to attitude towards the advice (P < 0.001). Web-based triage can contribute to a more efficient primary care system, because it facilitates the gatekeeper function.
Introduction
Conventionally, triage is applied to urgent conditions, 1 but it is also used in primary care to reduce after-hours referrals, usually by telephone. 2 However, telephone triage depends on the ability to make consistent and accurate decisions based on the responses from patients. The advice given by caregivers during telephone triage is often inconsistent and inadequate. 2
Web-based triage may provide advice about the necessity of visiting a general practitioner (GP) in case of minor ailments like a sore throat, which in practice usually leads to self-care advice. 3 To our knowledge, there is little published information about the effect of web-based triage on the care delivery process. Studies of the use of web-based triage in a college health setting indicate good accuracy. 4 There are also indications that web-based triage can reduce utilization costs (e.g. hospital emergency room visits) by directing people to the most appropriate place for care. 5 However, there is a lack of knowledge about the potential of web-based triage to reduce unnecessary doctors' visits by the general public.
The aim of the present study was to investigate the use of a web-based triage system in primary care, and compliance with the medical advice delivered by it. In a retrospective analysis we investigated the type of complaints that were submitted and the kind of advice provided by a Dutch web-based triage system in primary care. In a prospective study, we investigated the users' compliance with the advice provided and the factors that promoted compliance.
Web-based triage system
We evaluated a web-based triage system (
Methods
We analyzed the use of the triage system over a period of 15 months. During this period, 13,133 different people began using the web-based triage system and 3812 patients went right through the triage process to the end. We examined the frequencies of the submitted complaints and the types of advice generated by the system. In the retrospective study, we used an existing database where ‘clicks’ per user were stored, while negotiating the web-based consultation process.
To determine which factors were related to compliance with the advice delivered by web-based triage, we carried out a prospective online survey with two waves (wave 1: n = 192; wave 2: n = 35). Immediately after the delivery of web-based triage advice, patients completed the first wave questionnaire. Using Likert scales (range -2 to +2), we assessed the usability of the web-based triage system, satisfaction with the generated advice, attitude towards the advice (Cronbach's α = 0.91), perceived social norm to comply with the advice (α = 0.79), perceived self-efficacy to comply with the advice (α = 0.89), perceived severity of the complaint (α = 0.84), response cost and response effectiveness. Users also indicated their intention (yes/no) to follow up the advice. After three months, the patients received a follow-up questionnaire which assessed their actual compliance with the advice. Using data from two completed questionnaires we carried out a regression analysis to assess the factors that were most strongly related to compliance with the provided advice.
Results
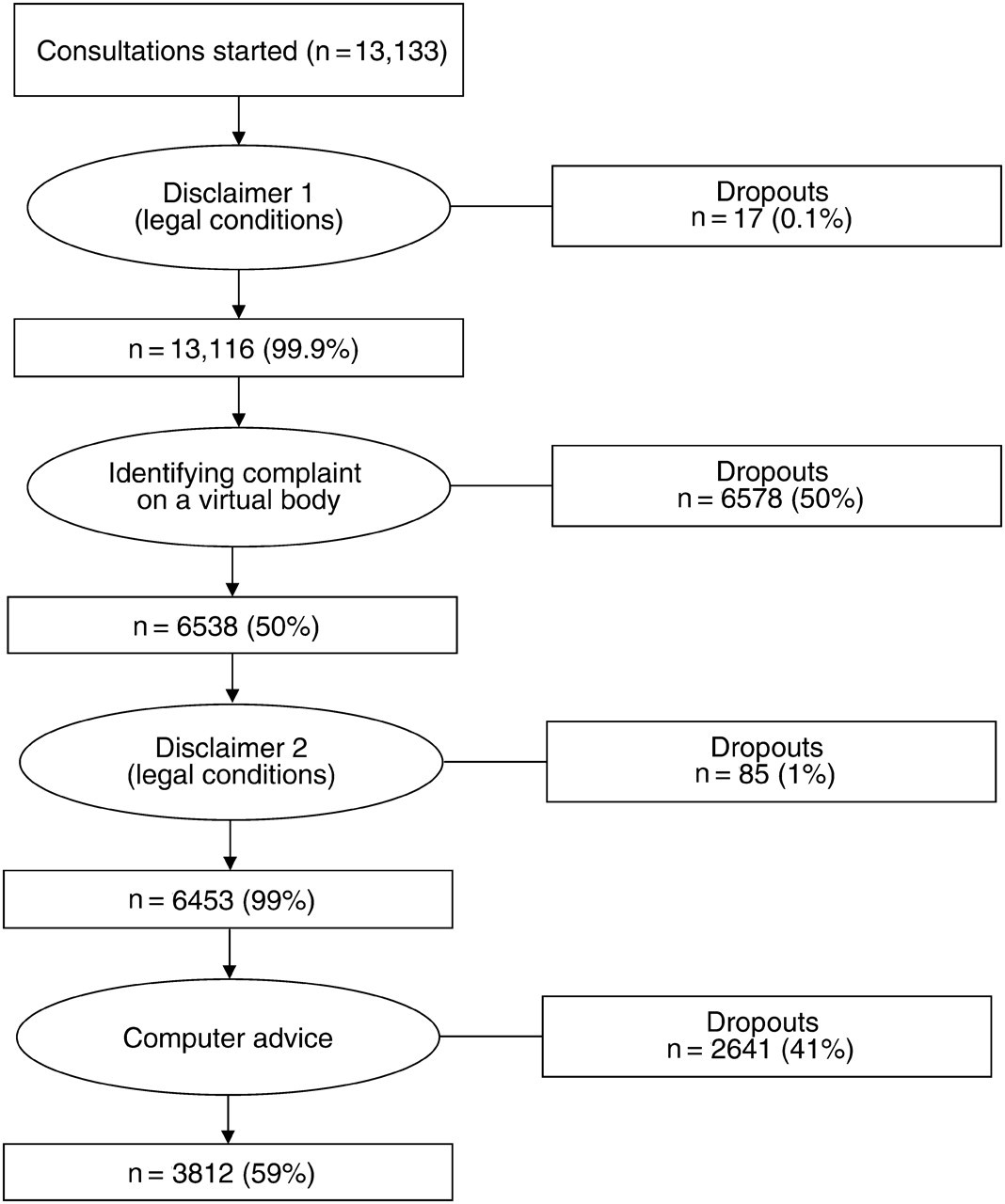
On average, the web-based triage system was used for 29 consultations per day. The numbers of people who started a consultation, submitted a complaint and received advice are summarised in Figure 1.
The consultation process
Out of 13,133 patients, who started a consultation, 6538 entered a complaint and 3812 completed the triage process and received medical advice (29% of all those started). There were two critical points regarding drop-out during the triage process. Half the users left the system at the point where they had to identify their complaints. The second critical point was just before receiving the advice.
The most frequently submitted complaints (Table 1) were common cold symptoms, such as cough and a sore throat (22%), itch problems (13%), urinary complaints (12%), diarrhoea (10%), headache (8%) and lower back pain (8%). Together, these complaints covered more than 70% of all submitted complaints. The frequency of complaints was similar to the complaints for which GPs are most frequently contacted in the Netherlands. 6 In general, self-care advice could be given more often for these complaints. 7
Overview of complaints
The advice generated is summarised in Table 2. Most commonly, the system generated the advice to contact a doctor (85%) and in 15% of the cases the system provided fully automated, problem-tailored, self-care advice.
Overview of generated advice
The relation between the submitted health complaints and the delivered advice is shown in Table 3. In general the system most frequently delivered the advice to visit a doctor in the short-term (within 24 hours or a couple of days with persistent complaints). The frequency of tailored self-care advice was limited, even for complaints that could be treated via self-care. 7 In the case of high frequency complaints, such as common cold, the system generated the advice to visit a doctor, while in the case of lower frequency complaints like itch the system generated tailored self-care advice. For headache and urinary complaints, self-care seemed not to be appropriate.
Overview of submitted health complaints (n = 2930) and advice given
*Urgent: call the emergency number 112/911
**Short-term: contact a doctor within 24 hours/within a couple of days with persistent complaints
Compliance with the medical advice
A total of 192 patients participated in a prospective study and completed an online survey immediately after the delivered advice. Most were females (n = 127,66%) with a middle (n = 101,53%) to high level of education (n = 55, 29%) and most were 16–35 years old (n = 107, 56%). Patients knew about the web-based triage system by surfing on the Internet (n = 73, 38%) and by advertisements of a health insurer (n = 62, 32%). At the time of completing the questionnaire, most patients (n = 104, 54%) had visited the web-based triage system for the first time. The triage system was used to gather information about a health complaint (n = 72, 38%) and to decide whether it was necessary to contact a GP (n = 38, 20%). Prior to triage, 73 patients (38%) intended to visit a GP for their complaint.
The evaluation of the web-based triage system is summarised in Table 4. All scores were neutral to slightly positive, which indicates that patients did not have a clear mental representation of what to expect from a triage consultation. This can be explained as a lack of experience, as only a minority had used the web-based triage system more than once.
Evaluation of web-base triage of complaints
*Social influence was computed from the product of two variables: ‘do you think your family finds it important’ (−2 to +2) and ‘to what extent the opinion of your family is important for you’ (1 to 5)
A follow-up questionnaire on actual compliance was completed by 35 patients. Among these, 20 (57%) had actually complied with the advice provided by the system. A regression analysis (Table 5) revealed that intention to comply was strongly related to actual compliance. In turn, intention to comply was strongly related to attitude towards the advice (P < 0.001). Attitude towards the advice was primarily shaped by the perceived effectiveness of the delivered advice (r = 0.71, P < 0.01) and trust in the web-based triage (r = 0.52, P < 0.01).
Predictors of intention to comply with medical advice delivered by the system
**P < 0.01
***P < 0.001
Discussion
The present study suggests that a web-based triage system has the potential to reduce costs and to promote self-care. However, there are two main problems: the high dropout rates and invariability of the generated advice. The dropout rates were high, especially before entering a complaint (50%) and just before the system delivered advice (40%). Based on the retrospective study we were only able to investigate the moments when users left the system, not their motives in dropping out or the perceived barriers in continuing with the system. In the future, in-depth interviews will be necessary to understand these matters.
A second problem was the invariability of the generated advice. In most cases the system generated the advice to visit a doctor (85%). In the case of high frequency complaints such as the common cold, the system generated the advice to visit a doctor, while in the case of lower frequency complaints like itch the system generated tailored self-care advice. This indicates that the system was more medically-driven than user-centred. In only 15% of the cases was self-care advice given, which may not reduce GP visits very much. A clear policy and new legislation about practising online consultation will be needed to maximize the accessibility and effectiveness of web-based triage and to clarify responsibility for online consulting.
Our findings are consistent with the findings of other studies about similar web-based triage systems. A web-based triage system, operated in the USA, was mainly used by women for high frequency, non-urgent complaints. 4
A second aim of our study was to investigate the factors that were related to compliance with the generated advice. A prospective survey revealed that attitude to the advice was strongly related to intention to comply with the advice, while intention to comply was strongly related to actual compliance with the advice. This means that web-based triage can promote self-management of minor ailments, especially among patients with a positive attitude towards the computer-generated advice. This positive attitude leads to intentions to follow up the advice and to actual follow-up.
A limitation of the study was the limited response to the online surveys and the incompleteness of the responses. Patients did not respond to all questions. The explanations could be the period of examination, summer time and the lack of experience with online triage. On the other hand, the results were similar to findings in other studies about web-based triage. 4,5
Although there were start-up problems, we foresee opportunities for web-based triage. Online patient interviewing via web-based triage can be used for diagnosis and early detection of risks, for instance for preoperative screening and handling taboo complaints, see for example
From prior research we know that reduction of uncertainty was the main factor in using web-based triage. 10 To support self-care and decision-making, it is important to match the expectations of users and the technology. Patients experienced a high percentage of referrals to a doctor, which was higher than they expected. So there was an imbalance between the central idea of web-based triage and the intended use of it. As self management is the focus of electronic care, an in-depth evaluation of patients' needs for autonomy and their readiness to make decisions about their health care is important. Especially in the case of chronically ill patients, who are overrepresented among emergency department visitors, web-based triage systems could reduce uncertainty by delivering alternative access to care, could reduce costs 11 and could facilitate more adequate communication for self-management. 12
In conclusion, web-based triage can contribute to a more efficient primary care system, because it facilitates the gatekeeper function. This implies that empowering patients by means of web-based triage requires interventions to instruct and motivate users; which is not common in the implementation of health care technologies.
Examples of self-care advice
Although your complaints can be (very) irritating, there are no reasons to worry;
You have a common disease, you do not need to visit your GP;
Your complaints indicate an upper airway disease, caused by a virus or a bacterium;
This is a non-severe disease, which recovers spontaneously in 1 to 2 weeks;
What a doctor can do, what you can do.
Footnotes
Acknowledgements
We thank Stef Verlinden of Vivici BV, The Netherlands, for his cooperation.