
Abstract
A total of 50 patients (affected by traumatic brain injury, stroke or multiple sclerosis) were treated for one month using a rehabilitation protocol. Rehabilitation could be monitored using a Portable Unit (PU) which could be installed in a patient's home allowing the measurement of kinetic and kinematic variables during exercise. In a preliminary analysis, the variables related to four rehabilitation exercises were examined for two patients at baseline and at the end of the one-month treatment. The exercises involved movement of checkers, a pencil, a jar and a key. The results suggest that, even if the overall duration of exercise execution is an important aspect of the rehabilitation process, other variables acquired by the PU might deliver useful information for assessing the patient's status. In order to integrate such variables into the assessment process, further studies are needed to investigate their eventual correlation with traditional rehabilitation scales and variables.
Introduction
The primary objective of the European Project HELLODOC 1 was to investigate a home-based upper-limb tele-rehabilitation service. The main aim of the service was to provide rehabilitation treatment in the patient's home for people affected by traumatic brain injury (TBI), stroke or multiple sclerosis (MS).
The core of the service was the Portable Unit (PU), which was installed in patients' homes. The PU had a desktop with sensors in, two shelf-like modules and a set of tools allowing the execution of daily tasks and the measurement of various kinetic and kinematic quantities. 2
In a feasibility study, the exercise performance of patients with TBI, MS and stroke was measured remotely. The present paper reports a preliminary analysis of some physical quantities remotely acquired from the sensors in the PU.
Methods
The core of the project was to demonstrate the clinical efficacy of the tele-rehabilitation service. A total of 50 patients were treated for one month by using a rehabilitation protocol based on physical exercises executed with the PU. 2
The standard outcome measures – the ARA test, WMFT Test, Barthel Index, Abilhand questionnaire, NHPT Test and the SF-36 questionnaire – demonstrated that the proposed treatment was as effective as the traditional one. 3 The average time per exercise per day, which was the only PU variable included in the above investigation, confirmed this.
The PU allowed patients to execute the following rehabilitation exercises: Pencil: the patient was asked to follow a path on the screen or to perform
writing activities on the screen; Jar: the patient was asked to move a jar to and from the shelves; Book: the patient was asked to move a book to and from the shelves; Key: the patient was asked to insert a key, rotating it to a specified angular
position; Light bulb: the patient was asked to screw and unscrew a device which resembled
a light bulb, and to turn on and off two different switches; Keyboard: the patient was asked to press the keys according to a specified
sequence; Checkers: the patient was asked to move a checker-like device on the screen
along an established path. The requested sequence to be performed is shown in
Figure 1.
The PU was designed to acquire a wide set of variables through kinematic and
dynamic sensors embedded in the system (Figure 2). The screen area was equipped with sensors so that position and pressure
exerted could be measured. Each shelf was equipped with 32 position sensors in order to
detect the correct position of the PU tools: the book and the jar. The keys of the
keyboard were equipped with sensors to record them being pushed. The switches and the
tool for the light bulb were equipped with sensors in order to capture the corresponding
event. The module for key insertion had angular potentiometers to measure the rotation
of the key, and triggers to detect the insertion event. Two webcams were mounted on the
PU to monitor the patient while performing the exercises.
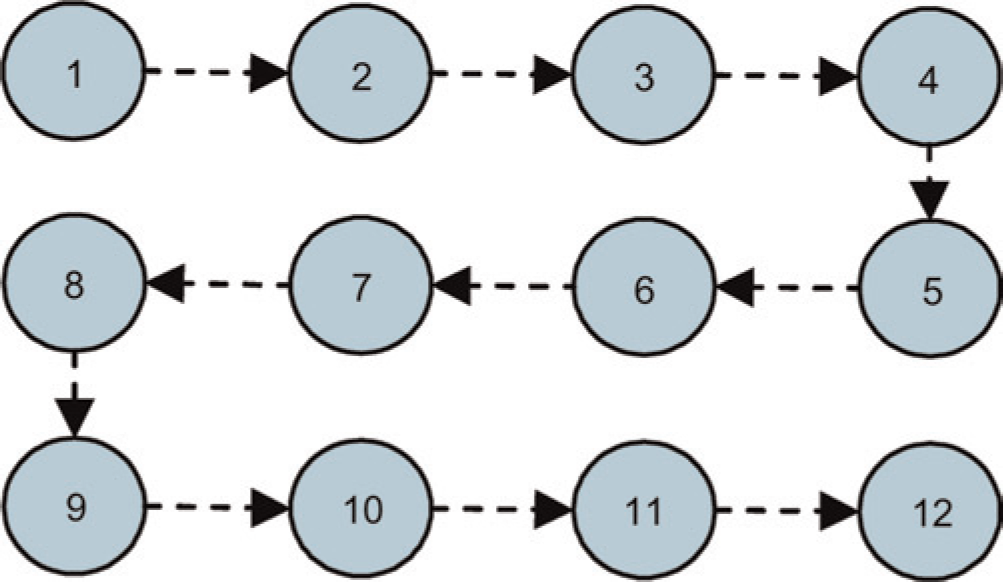
Sequence of checker positions

PU with sensors and main variables acquired
All the physical variables acquired by the PU during each exercise execution were extracted and analysed, together with the video related to each exercise execution 4,5 which allowed the patient's activity to be checked remotely.
Results
The variables related to four rehabilitation exercises are reported below for two patients (A and B, respectively) at baseline and at the end of the one-month treatment. Work is still in progress.
Checkers exercise
For patient A, the mean transition time from one position to the next was 3.0 s (SD 1.1) at the start of treatment and 2.7 s (SD 0.8) at the end. The mean resting time at each of the requested positions was 3.1 s (SD 2.4) at the start of treatment and 8.0 s (SD 2.5) at the end. Even though the total time for the exercise as a whole was longer at the end of the month, the total transition time was shorter. Pressure during checker landing seemed to be less variable at the end of treatment except for the final requested position.
For Patient B the times were longer at the end of the month, even with respect to transition time. However, transition times were already short at the beginning of treatment, while execution time remained almost unchanged. The mean pressure significantly increased at the end of the month (P = 0.024).
Clinical interpretation of these results needs further investigation.
Pencil exercise
For patient A greater pressure modulation was evident during the exercise at the end of the treatment (Figure 3). There was also greater improvement at the end of treatment in matching the established path.

Patient A. Pencil exercise: (a) trajectory and (b) pressure exerted
For patient B, pressure modulation was more evident at the end of treatment, even though path matching seemed to be very good.
Jar exercise
The analysis was conducted by comparing the time intervals needed to reach each position, both on shelves and on the screen, and estimating the mean velocity. The transition times for the right and left shelf are shown in Table 1 for Patient A. At the end of the month of treatment, the time intervals between jar landings on the right shelf were a little shorter, and more repositioning actions had been performed with respect to the left shelf.
Transition time (s) between two successive positions of the jar
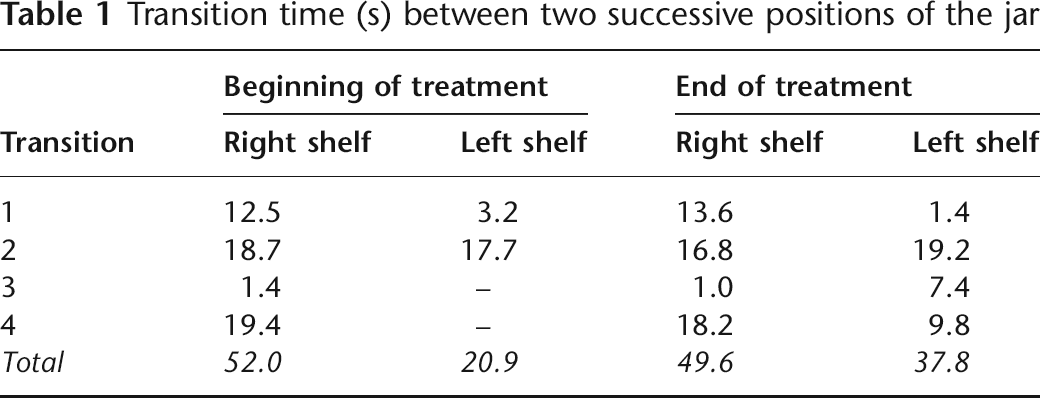
The results for Patient B were very similar to those for Patient A.
Key exercise
For Patient A, the different peak values (180° and 360°) were in correspondence with the same command (Figure 4). The key rotation at the end of treatment was clearly faster than before. Further investigation is needed.

Patient A. Key exercise: angular pattern
For Patient B, the shapes before and after treatment were similar. The only difference was the greater resting time in the extreme angular positions at the beginning of treatment. At the end of treatment, the time intervals were shorter and less variable than at the beginning: 1.9 s (SD 0.1) vs 3.2 s (SD 0.6) calculated over the first 4 cycles.
Discussion
The examples reported in this paper show that, even if the overall duration of exercise execution is an important aspect of the rehabilitation process, some other variables acquired by means of the PU might deliver useful information for assessing the patient's status. In order to integrate such variables into the assessment process, further studies are needed to investigate their eventual correlation with traditional rehabilitation scales and variables. The main aim should be to better modulate the rehabilitation protocol and adapt it to the individual patient's requirements. The tele-rehabilitation service which has been developed is a method of controlling the relevant variables from a distance.