
Abstract
Teleradiology can be used to provide health care to rural populations, especially where there is a scarcity of resources, including on-site radiologists. We have established a network link between a commercial teleradiology provider in Bangalore, south India and the Ramakrishna Mission Hospital (RKMH), located over 3000 km away in the north east of India. Image files were transferred to Bangalore via an ADSL connection using secure file transfer protocol. In the 12-month period beginning in August 2007, a total of 962 studies was sent to Bangalore from the RKMH. The average turnaround time for the report to reach the hospital once the images had been received in Bangalore was six hours for non-emergency cases. For emergency cases the turnaround time was consistently below 30 minutes. Because the RKMH was a charitable institution providing rural patients with free or low-cost treatment, no charge was made for the reporting. Our experience demonstrates that remote implementation of teleradiology is possible in rural India. The service has proved valuable for the remote hospital concerned.
Introduction
Much has been written about the value of teleradiology for rural populations, especially where there is a paucity of technical, IT and medical resources, including on-site radiologists. 1–3 The challenge is to incorporate effective and secure methods of image and radiology report transmission for rural populations.
Our experience at Teleradiology Solutions concerns the Ramakrishna Mission Hospital (RKMH) which is located in Arunachal Pradesh, over 3000 km away from our organization in Bangalore, south India. Arunachal Pradesh is a state in north-east India with an area of 84,000 km2. It is predominantly mountainous and relatively inaccessible, and has a mainly rural population of over one million. The RKMH is located in the state's capital and is a referral hospital for the entire state. The hospital has the only CT scanner in the whole of Arunachal Pradesh.
Although there was one full-time qualified radiologist and one part-time qualified radiologist at the RKMH, there were large numbers of cases, particularly computerised tomography (CT) cases and no other radiologists on-site to share the workload. To cope with the excess caseload, we set up a low-cost teleradiology system which allowed transfer of images and reports between the RKMH and Teleradiology Solutions. This paper reports the experience of the first 12 months.
Methods
To facilitate the transmission of data between the two sites, we were given access to a PC at the hospital. All settings were done remotely from Bangalore using remote access software (VNC). 4 Computer maintenance including anti-virus scanning, fine tuning and cache deletion, were all done from Bangalore.
At the request of the on-site radiologist, the radiographers at the RKMH could transmit DICOM CT images to Bangalore as soon as the scan was complete. Images were sent in the form of compressed ZIP files by secure-file transfer protocol (sFTP) using the FTP client in Internet Explorer. Data were transmitted via a 256 kbit/s ADSL (asymmetric digital subscriber line) connection. Patient information including clinical details was entered into the Radiology Information System (RIS) by the radiographers which enabled a case-list to be generated (Figure 1).

Screenshot of the RIS work-list
In Bangalore, we used the eFilm software (Merge Healthcare) for DICOM image viewing. After reporting in Bangalore, the reports (Figure 2) were sent back to the RKMH using the same RIS by the radiologists in Bangalore. The RIS system was configured to generate a final report from the details entered into the RIS (Figure 2).
Final report
Requests for preliminary reports for emergency cases or notifications of failed image transmission were communicated by telephone or by encrypted email.
Results
In the 12-month period beginning in August 2007, a total of 962 studies was sent to Bangalore from the RKMH (including repeat and follow-up studies). All of them were CT scans (see Table 1). All 962 patients had relevant clinical and demographic information loaded into the RIS successfully. However image transmission failed initially in 180 cases (19% of the total), although all were subsequently retransmitted successfully.
Type of CT study
The average turnaround time for the report to reach the hospital once the images had been received in Bangalore was six hours for non-emergency cases. This meant that patients could see their clinician at the latest by the next day with the report. For emergency cases the turnaround time was consistently below 30 minutes. Out of 962 cases, 32 cases were emergency cases where preliminary reports were available within 30 minutes. An example of an emergency case is shown in Figure 3.
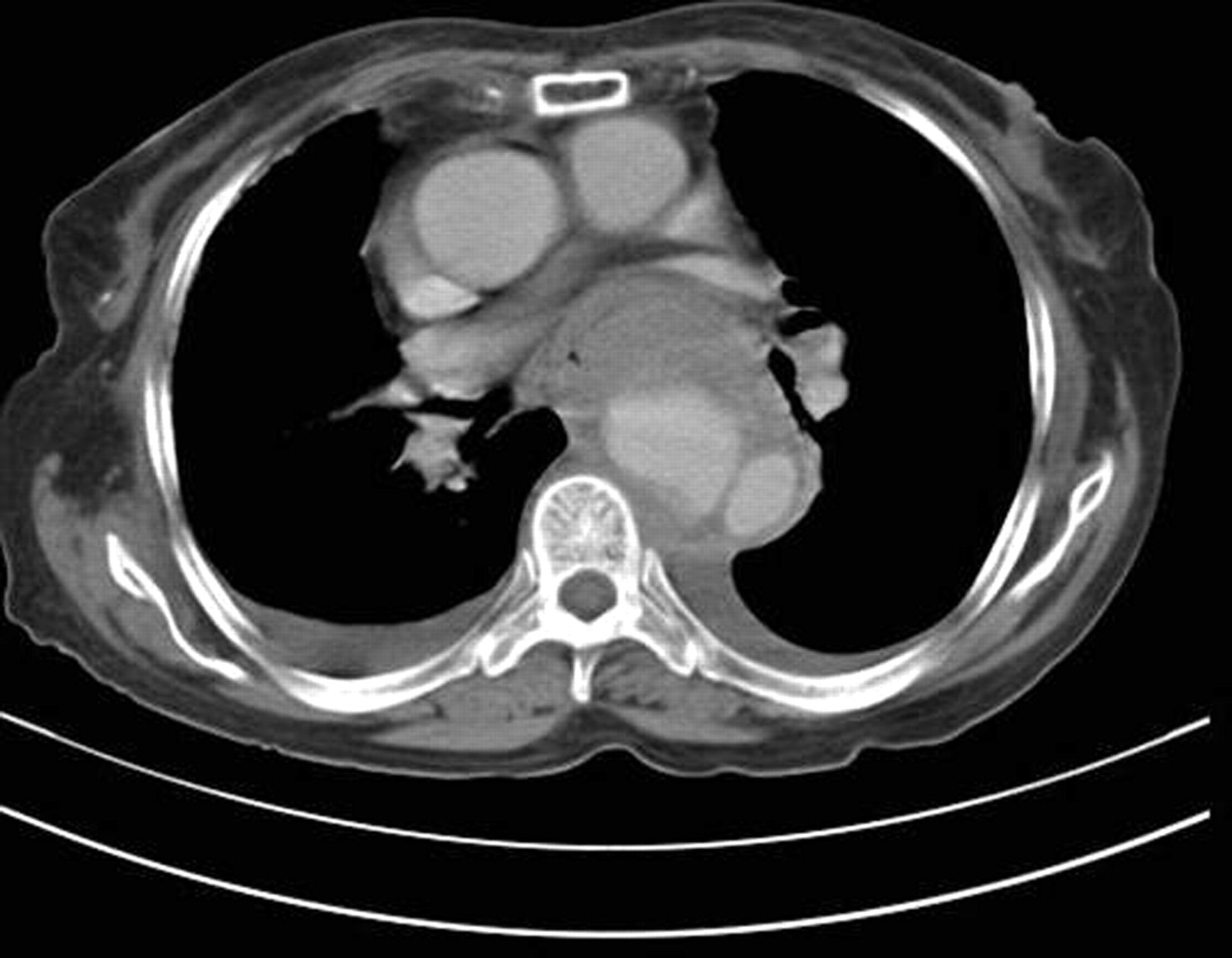
Emergency case. The axial CT section of the chest shows a dissecting aneurysm of the thoracic aorta
Discussion
In India, 80% of the population lives in rural areas, whereas 80% of the doctors live in the big cities. 5 Thus there is great potential for teleradiology to support health-care institutions in remote and far-flung locations, such as the RKMH.
It was initially proposed that the RKMH purchase a low-cost, picture archiving and communications system (PACS) that was web-accessible, such as the eRAD system. 6 However even the cheapest web-accessible image archiving system (costing approximately US$2500) was too expensive for the charitable institution. Although free PACS software such as K-PACS, Osirix or Conquest was available, it would not have been suitable for the erratic bandwidth (256 kbit/s DSL) available at the hospital. Also Osirix, although free, needs an Apple Macintosh computer, and these are relatively expensive. 7
The hospital also considered the use of satellite transmission, for example using VSAT (Very Small Aperture Terminal) equipment. This approach had the advantage that satellite bandwidth was provided free of charge by the government of India. However, there have been reports of VSAT transmission being unreliable in rural India. 8
We were able to transfer images and reports successfully using an ordinary broadband connection. Secure-file transfer protocol (sFTP) was employed. Staff at the RKMH were able to connect to our FTP server using the FTP client in Internet Explorer, which is free to use, 9 and then upload the images as compressed ZIP files. It has been shown that FTP or sFTP offers better transmission security than common email protocols (SMTP and POP), which are not as useful for transmitting complex images such as CT scans. 10 Although sFTP utilizes secure-shell encryption (SSH), there have been more recent developments in data encryption methods for images, and these deserve further investigation. 11
At the start of the project, both sites were in daily communication by email and telephone to clarify initial queries. Subsequently communication was usually limited to requests for reports on emergency cases. Communication is vital in the initial phase of telemedicine work and it has been shown in other studies that without such interaction, the overall performance of the system will be suboptimum and may lead to failure. 12
The two CT technicians at the RKMH were qualified radiographers with subspecialty CT training. They were trained to use the RIS via remote access to enable uploading of relevant patient and clinical details. The CT protocols were set by the on-site radiologists, who were general radiologists. Those cases not reported by the on-site radiologist were reported by the radiologists in Bangalore. Usually the latter were general radiologists, but neurological or musculoskeletal cases were reported by the relevant subspecialty radiologist. In keeping with the fact that the RKMH was a charitable institution providing rural patients with free or low-cost treatment, no charge was made for the reporting by Teleradiology Solutions or for the technical support provided.
Our experience demonstrates that remote implementation of teleradiology is possible in rural India. The service has proved valuable for the remote hospital concerned, as evidenced by the following comment: ‘I want to convey my heartfelt gratitude for the help extended by you. I have no words to convey my appreciation for your sincere efforts and will to help us. We can continue to render our service to the suffering humanity here only if we receive the kind of support that you are giving.’ (Swami Udaarnanda of the RKMH).
Footnotes
Acknowledgements
We thank Swami Udaarnanda (Ramakrishna Mission Hospital).