
Abstract
We explored the benefit of video communication in home rehabilitation after shoulder joint replacement and compared it to referral for physiotherapy in the conventional way. A total of 22 patients were included in the study. The intervention group (n = 10) had training at home under the supervision of a physiotherapist at the hospital using videoconferencing. The control group (n = 12) had physiotherapy training in a conventional way in their home town. All patients had the same postoperative, three-phase-programme for two months. The outcome measures were a Visual Analogue Scale (VAS) for pain, range of motion (ROM), shoulder function ability (Constant score and SRQ-S) and health-related quality of life (SF-36). Questions about areas of priority for improvement and general satisfaction with the shoulder were also included. The telemedicine group received a greater number of treatments compared to the control group. After the intervention, there were significant improvements in VAS-pain, Constant score and SRQ-S for both groups. The telemedicine group improved significantly more in all three measurements than the control group (P < 0.001 for all). When changes from baseline to follow-up were compared, the telemedicine group improved significantly more in terms of decrease in pain (P = 0.004) and vitality (P = 0.001) than the control group. Despite some limitations, there seem to be clear benefits from physiotherapy at a distance with a telemedicine technique that allows patients to obtain access to physiotherapy at home.
Introduction
Early therapeutic movement exercises are important after a shoulder joint operation. 1–3 The usual procedure after shoulder joint replacement includes physiotherapy at the hospital, followed by exercises at home. The individually tailored physiotherapy programme is supervised by a physiotherapist who is based at the local treatment centre. 4 Rehabilitation in remote areas can be difficult due to long distances between home and the therapist, a problem which can lead to permanent disabilities due to lack of appropriate rehabilitation and resources. 4–8
Delivery of telemedicine has often been described either between health-care professionals at each telemedicine site or between health-care professionals and a patient at a remote site. 9–11 The experiences with telemedicine have shown positive response. 12–16
Physiotherapy is a highly manual process. Not being able to conduct manual therapy, or to palpate, may be a major disadvantage in telerehabilitation. 17 Nonetheless, telemedicine systems have been developed for home use in cardiac, 18 neurology 19–22 and orthopaedic rehabilitation. 23–28 Physiotherapy at home via telemedicine might improve rehabilitation through continuing exercise sessions under the supervision of an experienced physiotherapist at the hospital, and this may increase patient satisfaction. 29
As far as we are aware, no studies have been done regarding postoperative physiotherapy at a distance after shoulder joint replacement in comparison with conventional physiotherapy. The aim of the present study was to explore the benefit of video communication in home rehabilitation, compared to conventional physiotherapy.
Methods
Twenty-five patients were selected from the waiting list for a shoulder replacement at an orthopaedic clinic at a hospital in Norrbotten, Sweden. To be included they needed to be Swedish speaking adults with either primary osteoarthrosis or rheumatoid arthritis. The exclusion criteria were humeral fracture, cuff arthropathy, the presence of medical conditions that precluded safe participation in exercises (e.g. recent myocardial infarction, stroke or severe pulmonary disease), psychiatric or neurological diagnosis, serious impaired hearing or vision, or dementia.
The study was conducted from January 2003 until February 2007. A total of 94 shoulder hemiarthroplasty replacements were performed during this period, of which 42 were comminuted proximal humerus fractures not included in the study. Of the remaining 52 patients, 27 were excluded for reasons such as lack of equipment. The remaining 19 women and six men were divided into two groups: one group received physiotherapy via telemedicine and a second group was referred to conventional physiotherapy.
The telemedicine group was enlisted according to the availability of telemedicine equipment at the time of surgery. The control group was selected prospectively from the remaining patients on the waiting list in order to match the telemedicine group in respect of age, sex and diagnosis. All patients underwent the same shoulder joint replacement with hemiarthroplasty by the same orthopaedic surgeon, using the same surgical technique.
There were three drop-outs: two patients in the telemedicine group and one in the control group. Thus 22 patients actually participated in the study: 10 in the telemedicine group and 12 in the control group. Their baseline characteristics were obtained from their medical records (Table 1).
Baseline characteristics of the 22 subjects
Intervention
All patients received, as a usual routine, a three-phase programme of exercise at the hospital and were instructed by the physiotherapist to combine the physiotherapy sessions with a progressive home-exercise programme of their own (Figure 1).

Study design
After the operation, the telemedicine patients had eight weeks of supervised physiotherapy including solitary exercise (Figure 1). After being discharged, the telemedicine patients exercised at home and were supervised at a distance by a physiotherapist at the hospital, who had long experience of treating shoulder patients. The patient was connected by a videoconference system which permitted the physiotherapist to perform the exercise programme with the patient.
The control patients were, as a usual routine, referred to continue the exercise programme during supervision by the physiotherapist at the local treatment centre. After discharge the physiotherapy aimed at 2–3 training sessions a week, gradually reducing to once every week or every second week.
All patients provided written consent to participate. The study was approved by the appropriate ethics committee.
Videoconferencing
Standard commercial videoconferencing units were used in the patient's home and the clinic (e.g. Tandberg 800, Sony PCS-50, Polycom VSX 3000). In the home, the equipment was connected via the patient's broadband service. Initially the connection in the clinic was via ISDN lines, and then later, a secure IP connection was used instead. The connection bandwidth varied from 256 to 768 kbit/s.
Measures
Assessments were done at baseline, during the week before the operation and at the end of the intervention (week 8) (see Figure 1). Demographic data, the length of stay at the hospital and the number of physiotherapy sessions during the rehabilitation period were derived from the medical records. All clinical assessments were made by the same physical therapist.
Self-rated shoulder pain was assessed as perceived pain on a Visual Analogue Scale (VAS) with the endpoints from none to extreme pain. 30
Maximum active pain-free shoulder range of motion (ROM) was assessed using a manual goniometer with the patient in a sitting position; external rotation around the long axis of the humerus was recorded with the arm hanging by the side of the body and the elbow flexed 90° and body segment references were the trunk, the humerus and the ulnae. Forward flexion was recorded with the humerus in the sagittal plane. 31–33
Shoulder function was assessed by using the Constant score, combining self-rated and objectively measured functional assessment by items covering pain, ability to perform normal activities of daily living (ADL) and active ROM. The basis of the score is a 100-point scale. Muscle strength was not measured due to the short time period after the operation. That excluded 25 points from the score. Consequently the maximum score was 75 points. The higher the score rating, the less severely affected was the shoulder. 34–36
The condition of the shoulder was self-rated by the Swedish version of the standardized Shoulder Rating Questionnaire (SRQ-S), covering health related to the shoulder on a VAS 0-10 cm scale and pain, activity of daily living, recreational and athletic activities and work on a five-point scale. The higher the score (17-100 points) the better was the condition of the shoulder. The score had two additional questions pertaining to shoulder satisfaction and areas for improvement (not used to calculate the overall SRQ-S score). 37–38
The Health-Related Quality of Life questionnaire SF-36 was used, covering the eight domains of physical functioning, role limitation due to physical problems, role limitation due to emotional problems, social functioning, mental health, pain, energy/fatigue and general health perceptions. The score ranged from 0 to 100, with a higher score representing better health. 39
Data analysis
The power calculation was based on a Mann-Whitney test and from the results of the first six patient results concerning the Constant score. Based on the differences between baseline and follow-up, the calculations showed that for 90% statistical power of detecting a significant difference (P < 0.05) nine persons in each group were needed. For within-group comparisons, the Wilcoxon Signed Ranks Test was used and for between-group comparisons the Mann-Whitney U test. Due to the disparity of initial values at baseline, the differences between the values at baseline and the values after follow-up were calculated and used for the analysis of the effect of the treatment. Standard software (SPSS version 15.0) was used for the analysis.
Results
The median age of the study group was 71 years. There was no significant difference in the number of subjects with osteoarthrosis and rheumatoid arthritis between the groups (P = 0.41) (Table 1). There was no significant difference in the length of stay at the hospital after the operation: 8.2 days and 7.7 for the telemedicine and control groups, respectively.
The telemedicine group received physiotherapy sessions initially lasting 60 min and then later for 10 min in duration. The sessions for the control group were estimated to last for 30 min each. The telemedicine group received a greater number of treatments compared to the control group (Figure 2).

The number of physiotherapy sessions during two months after discharge from hospital
There were lower pre-operative measures in the telemedicine group in pain (VAS), function (SRQ-S), mobility (ROM) and physical function, pain and vitality domains in health-related quality of life (SF-36) compared to the control group. After the intervention, there were significant improvements in VAS-pain, Constant score and SRQ-S for both groups. The telemedicine group improved significantly more in all three measurements than the control group (P < 0.001 for all). Both groups improved in ROM after the intervention and the telemedicine group improved significantly more than the control group in external rotation (Table 2).
Within-group comparisons between the baseline and follow-up and between-group comparisons in improvement between the baseline and follow-up
None of the patients were dissatisfied with the shoulder and there was no significant difference (P = 0.11) between the two groups after the intervention according to the self ratings in SRQ-S (Table 3).
The number of satisfied patients according to the SRQ-S questionnaire. The results of the telemedicine group and the control group before and after the intervention are shown
The majority of the patients when asked before the operation said that their first priority was to achieve less pain. After intervention the majority gave priority to achieving a better function in ADL. One patient did not rate any second priority (Table 4).
The domains that the patients gave priority to according to the SRQ-S additional question: ‘Please give priority to the two areas in which you would most like to see improvement (select 1 for the most important and 2 for the second most important between pain, ADL, sport and work)’
According to the SF-36 there were significant improvements in vitality (telemedicine group P = 0.004, control group P = 0.001) after the intervention and in physical function for the telemedicine group (P = 0.021) and close to significant for the control group (P = 0.052).
The telemedicine group also improved significantly in all domains, apart from the social (P = 0.44) and role-emotional function (P = 0.38) (physical functioning P = 0.021, role-physical P = 0.031, pain P = 0.002, general health P = 0.012 and mental health P = 0.004).
When changes from baseline to follow-up were compared, the telemedicine group improved significantly more in terms of decrease in pain (P = 0.004) and vitality (P = 0.001) than the control group (Figure 3).
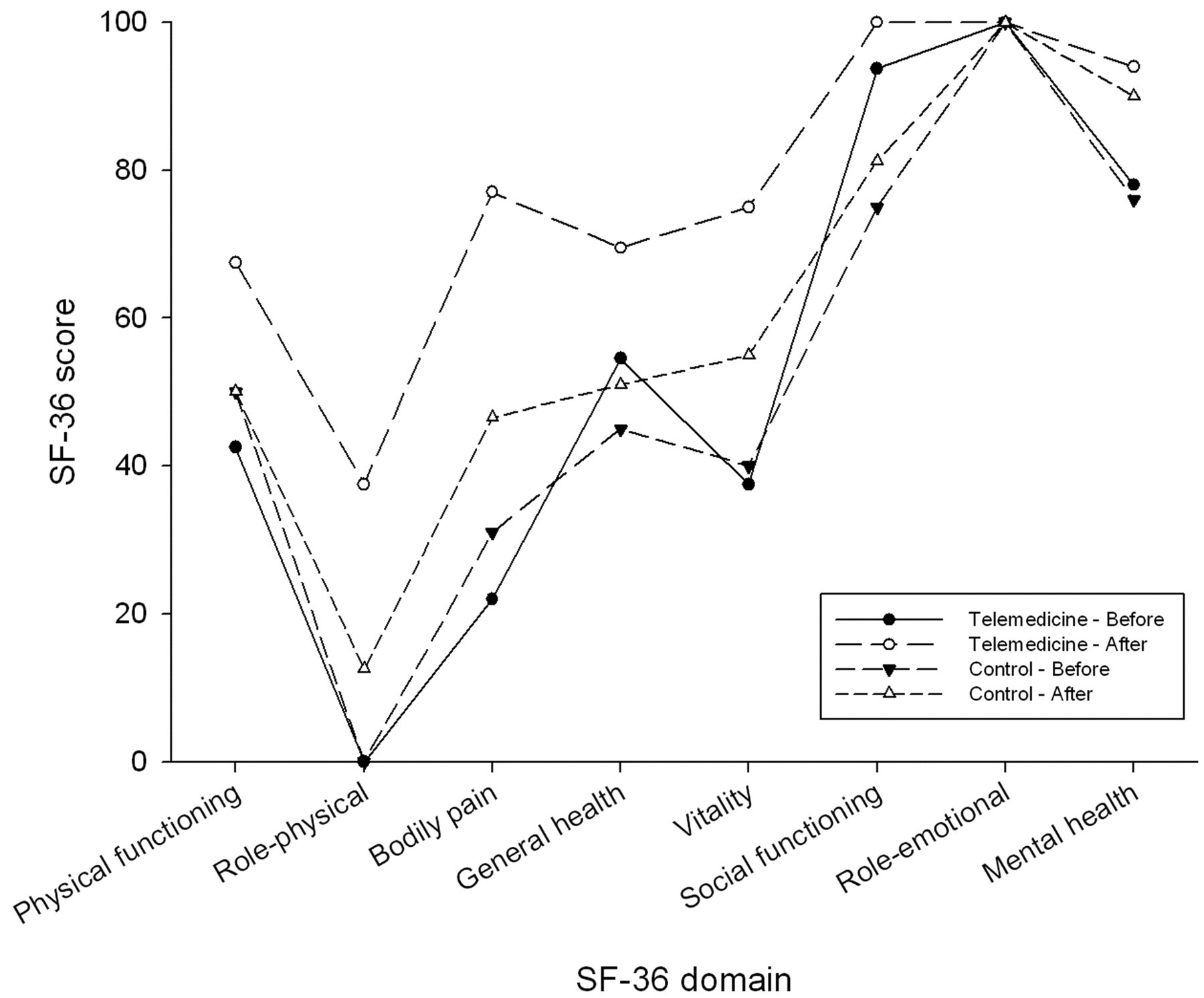
Patient questionnaire results for health-related quality of life
Discussion
The results showed that physiotherapy using video communication between the patient's home and the hospital was feasible and effective for persons who had undergone a shoulder joint replacement. The telemedicine group improved significantly more in terms of shoulder pain, mobility and function as well as in pain and vitality domains in health-related quality of life than the control group.
The strengths of the study were that all patients had the same kind of operation from the same surgeon, and there was no difference in respect to the length of stay at the hospital or in the written physiotherapy standard programme of exercises. The home exercise programme was a continuation of the exercises given at the hospital. The difference in the intervention between the groups was the manner in which the physiotherapy was supplied to the patients, the number of treatments and the varying physiotherapist.
The physiotherapist who treated the patients was not the same person as the assessor. Our procedure of using the same assessor, who used standardized measures in all assessments throughout the study, is a procedure which has been recommended by other authors in order to guarantee the consistency of the examination variables over time. 40
The present study was designed in a nonrandomized fashion. The telemedicine group and the matched control group included two of the most common diagnoses indicating shoulder replacement: osteoarthrosis and rheumatoid arthritis. The validity of the study was strengthened as no patient refused to participate. As there were small groups – ten in the telemedicine group and twelve in the control group – it was not appropriate to randomize as a randomization could have resulted in an uneven recruitment, with one group with mainly rheumatoid arthritis patients and one group with mainly osteoartrosis patients. Other techniques, such as cluster-, or block randomization would render it more difficult to obtain participants in the study due to inclusion- and exclusion criteria, the amount of technical equipment and practical facilities to get the technique. The size of the study was based on an analysis of statistical power. A weakness of the study is that the treatments were not delivered by the same therapists, which might have resulted in a bias.
The outcome variables were based on pain, shoulder function and mobility, areas of improvement (pain, ADL, sport and recreation, and work) which were given priority by the patients and overall satisfaction and health-related quality of life. The measures used are all well recognized.
We were aware of the weaknesses of the study that the manner in which the physiotherapy was supplied to the patient could not be blinded, either to the patient or the therapist, and the physiotherapist who made all the assessments was not blinded. It is reasonable to assume a positive attitude and expectancy among those who were included in the telemedicine group. The patients rated four assessments by themselves and three together with the assessor, which can be seen as a bias. Considering the above information we did our best to be objective and minimize the influence on the patients, even though it was impossible to eliminate it completely.
One explanation for the improvements in the telemedicine group is the more extensive, frequent and continuous physiotherapy which occurred. There was no break in the rehabilitation chain and no period of inactivity for the shoulder, when the telemedicine patients were discharged from the hospital. The different number of physiotherapy sessions between the groups could be explained by long travel distances, something which complicates frequent meetings even if specific physiotherapy is available.
The patients and the physiotherapists in the telemedicine group had no complaint about the technical voice and image quality. The different techniques used to transfer image and voice fulfilled our expectations. Agrell et al. indicated that it is the attention of the staff, not the quality of the image, which is important in home telecare. 41 Furthermore, Melander-Wikman showed that elderly patients want physiotherapy support when they are tired of exercises and close to giving up. 42 Elderly patients also need repeated teaching to encourage them to remember their exercises. 43
In the present study the distance sessions varied in length from 10 to 60 minutes. This finding is consistent with the telerehabilitation study by Tousignant et al. 44 The fact that the physiotherapist could give instructions to a patient on a regular basis could be one explanation for the effectiveness of this method. Our results of the continuity of duration of the contact indicate the importance of the patient and the physiotherapist checking on the training regularly.
Another explanation could be that the patient could stay at home, prepare and focus on the training. The telemedicine group was also supervised by a physiotherapist from the hospital who was familiar with this type of patient. Brems has shown that availability of physiotherapists with special knowledge about shoulder operations influenced the result after the operation. 1 The present study indicates an increased accessibility to frequent and specific physiotherapy. The study might have produced a different result if both groups had treatment by one and the same physiotherapist both in the telemedicine and the control group. This would be an interesting topic for another study.
The telemedicine group had significantly less pain compared to the control patients. This may be explained by the physiotherapists' transfer of information and knowledge about the shoulder, how to perform accurate exercises and how to manage situations with pain. It is possible that telemedicine promotes participation and responsibility by the patient, which is one of the cornerstones in the rehabilitation process. 6,45
A challenge to refine physiotherapy at a distance may be the development of indirect techniques to bring the therapists hands ‘through the wires’, by the use of robotics, or to develop the physiotherapist role in order to compensate for not being in the same room as the patient. It would be interesting to see more studies about physiotherapy at a distance, both long term follow-ups and studies on its cost effectiveness.
In conclusion, despite current limitations, there seem to be clear benefits from physiotherapy at a distance with a telemedicine technique that allows patients to obtain access to physiotherapy at home.
Footnotes
Acknowledgements
The project was funded by the Centre for Distance-Spanning Healthcare at Luleå University of Technology, and Norrbotten County Council in Sweden. We also thank all the patients and colleagues who participated in the study.