
Abstract
We conducted a feasibility study to find out whether a simple preliminary examination using telemedicine for diagnosis was sufficient to identify sleep-related breathing disorders (SRBD). Night-time pulse oximetry recordings were made in normal home surroundings on patients suffering from sleep apnoea/SRBD by doctors with a range of non-specialist backgrounds. The readings were transmitted to the relevant sleep laboratory, examined and the results returned to the referring doctor. From 80 patients (aged 29 to 60 years), 58 complained about characteristic symptoms (snoring, daytime sleepiness); 33 of these patients showed additional symptoms of associated diseases. In eight patients associated diseases were found without any symptoms. The findings were compatible with SRBD in 58 cases (73%); 12 of these were asymptomatic patients. A total of 57 patients had to be referred to a sleep laboratory for differential diagnosis by full polysomnography. Of the 22 patients (28%) without pathological findings following pulse-oximetry, 12 were symptomatic. The system described here is suitable for the creation of referral networks and for the identification of patients from institutions not trained in sleep medicine, who would otherwise not have been referred for specific diagnosis to a sleep laboratory.
Introduction
Patients with sleep apnoea often complain about non-specific discomforts and usually consult doctors who are not specialised in sleep medicine. In most cases these patients suffer from cardiovascular diseases or psychological problems such as depressive moods, depression or lethargy. In the literature there are numerous references concerning links between sleep-related breathing disorders (SRBD) and increased cardio- or cerebrovascular risks. A large number of studies have documented an association between SRBD and lack of concentration, general lack of performance, reduced memory and depression. 1–4
These patients mainly consult doctors – such as general practitioners, internal medicine specialists, cardiologists, neurologists, psychiatrists, ear, nose and throat (ENT) specialists – or are inpatients in medical facilities which do not have cardiorespiratory polysomography available. In most cases referral for further diagnosis is not feasible due to the large number of potential patients and limited capacity. A differentiated examination of sleep apnoea via polysomnography in a sleep laboratory is costly and time-consuming.
As a preliminary screening method, night-time pulse-oximetry is a simple and cost-effective method of detecting sleep-related breathing disturbances. 5,6 The time-averaged oxygen-saturation, as well as the desaturation-index, are of predictive value compared to the apnoea-hypopnea index used in polysomnography as an indication for the need for night-time respiration-therapy. 7–10 Pulse-oximetry will not replace the gold standard of full polysomnography. It can however be regarded as a suitable pre-selection method for those patients who show only minor clinical symptoms.
A preliminary diagnosis by pulse-oximetry requires interdisciplinary co-operation between doctors who are not specialised in sleep medicine and those in sleep-medically qualified institutions (e.g. sleep laboratories). The latter are responsible for referral of patients with suspected sleep apnoea for final diagnosis via polysomnography. Telemedicine is an interface between sleep-medical experts and referring professionals. The aim of the present study was to examine the feasibility of using a simple pulse-oximeter via telemedicine to achieve the pre-selection of patients requiring further diagnosis.
Methods
Patients with the following problems were considered for the study: coronary cardiac diseases, heart insufficiency, cardio-arrhythmias, hypertension, adiposity/obesity, stroke/transient ischaemic attack (TIA), diabetes mellitus, depression, day-time sleepiness and snoring. Prior to the examination, the patients were advised about symptoms, risks and the diagnosis of sleep apnoea in a specially produced patient information film.
The night-time examination recordings were transferred to the iDoc-Institute and subsequently evaluated in the sleep laboratory of the Karl-Hansen-Clinic (Bad Lippspringe). The final diagnosis was then forwarded with a recommendation for any required measures or treatment to the referring doctor. In case of alarming findings further diagnosis was undertaken and therapy was introduced (see Figure 1).

Screening examination procedure. There were five stages: 1. Outpatient night-time data collection. Step 1. Information. The patient or interested party watched the information-film at the doctor's or specialist's centre (e.g. in the waiting area). Step 2. Pulse-oximetry. If the patient wished to undergo screening on the basis of the information received, the doctor issued a measuring device for use at home to record the night-time data. 2. Upload to the system. The patient returned the device to the doctor for initial diagnosis. The recorded results were transmitted to a central server. 3. Scrutiny of data and report. A somnologist in the associated regional sleep-medical centre scrutinised the data and made the findings available to the patient's doctor. 4. Receipt of the expert's report. 5. Recommendation for treatment in cases of pathological findings. Referral for outpatient-polysomography or direct referral to a sleep laboratory. The findings of the evaluation were directly discussed with the patient in the referring institution. In case of alarming values, further clarifying diagnostic tests by a consultant or direct follow-up treatment in a sleep-medical centre were recommended.
Patients
The study was approved by the appropriate ethics committee and participation in the study was voluntary. The measurements were performed between June 2005 and January 2006. There were 80 patients (26 women) on average 30–60 years of age (see Table 1). They suffered from existing diseases possibly caused by a sleep-related breathing disorder (see Table 2). There was a total of 133 diagnoses, as some patients had multiple diseases. To assess the daytime-pathology the Epworth Sleepiness Scale (ESS) was applied. 11 Usable scores were obtained in 25 cases (the questionnaires of 55 patients were either incomplete or missing altogether).
Demographic data of the groups according to the findings following pulse-oximetry
Distribution of associated disease patterns (some patients had multiple diagnoses)
The inclusion criteria were agreement to wear the measuring device at night and the ability to apply the device, consent to undergo the examination and accept the costs. The exclusion criteria were intolerance of pulse-oximetry, or intellectual or physical difficulty with applying the device, e.g. forms of dementia, severe neurological disease or severe endocrine disorders.
Examination procedure
After a detailed medical history and declaration of consent the patient was introduced to the application of the pulse-oximeter for recording. The questionnaires (ESS) were explained and handed out. The screening was performed at the patient's home, usually between 21:00 and 08:00.
On the day following the night-time screening, the patients took the pulse-oximeter back to the centre or clinic. The pulse-oximetry data were then transmitted to the server and, together with recorded risk factors and the ESS-score, forwarded to the sleep laboratory at the Karl-Hansen Clinic for manual evaluation. A somnologist then evaluated the data without knowledge of the individual patient. The analysis was based on one night's data. The final diagnosis was sent back to the referring doctor with a recommendation for further action.
In cases where the pulse-oximetry revealed no pathological findings but the patient complained about sleep quality, further diagnostic tests were conducted according to the guidelines of the German Sleep Society (DGSM). In cases of pulse-oximetry without any pathological findings and no sleep-specific complaints, no further tests were performed. Patients with pathological pulse-oximetry results were advised to undergo further diagnostic examinations in the sleep laboratory.
Measuring instrument
A compact wrist-pulse-oximeter was used (Model 3100 WristOx, Nonin, Plymouth, Minnesota, USA). The pulse-oximeter could store up to 8 hours worth of data at intervals of 1 second. The measurement sensor was a conventional adult finger clamp sensor. The pulse-oximeter switched on automatically as soon as a finger was clamped into the sensor and switched off when it was removed. An interface-cable was used for data transfer to a PC. The analysis of the collected data was effected via standard software (nVISION, Nonin, Plymouth, Minnesota, USA).
Technical infrastructure
Every participating doctor and care institution could connect to the server using a web-browser on the individual PCs. For distribution of anonymised data, appropriate security criteria and encryption mechanisms were implemented.
Target criteria
The event-definition for the analysis of the pulse-oximetry measurements was based on a drop in oxygen saturation (>4%), duration (>10 seconds) and cumulated desaturation period (minutes <88%). The evaluation criteria regarding the severity of desaturation were the desaturation-index (events per hour), the minimum oxygen saturation (in %) and the desaturation period (in minutes).
Taking into account the AASM-criteria,
12
we established the following severity classification in respect of suspected sleep apnoea:
No pathological findings: saturation >95% or desaturation index <5 /h Minor: saturation >85% or desaturation index <15/h Moderate: saturation >81% or desaturation index 15–30/h Severe: saturation >81% or desaturation index >30/h
If one of the two criteria was not met (e.g. a desaturation index >30/h but saturation of only 82%), the higher severity code was applied (‘severe’ in this example). In addition, consideration was given to the pulse-frequency variability on final individual evaluation. The event-analysis was based on manufacturer-recommended settings (change in pulse-frequency: 6 beats/minute over >8 seconds).
Statistical analysis
The connection between the patients' previous symptomatic and asymptomatic conditions, the severity code regarding suspected Obstructive Sleep Apnoea Syndrome (OSAS) based on pulse-oximeter recordings and comorbidities were investigated. The Spearman correlation coefficient was calculated with SPSS version 12. Factor analysis was performed using the main-component method as per SPSS version 12.
Results
A total of 58 of 80 patients complained about characteristic symptoms (snoring, daytime sleepiness). In addition to the symptoms, 33 of the patients had one or more associated diseases. Eight patients with associated diseases were free of symptoms.
In total 58 patients (73% from 80 patients) had – on the basis of the defined criteria – minor, moderate or severe medical findings compatible with sleep apnoea; 12 of these patients were asymptomatic. A total of 23 patients (29% from all 80 patients, or approximately 40% of the 58 patients with suspected sleep apnoea) with severe specification were referred to the sleep laboratory for further tests and subsequent therapy. Altogether 35 patients (44% from all 80 patients or approximately 60% of the 58 with suspected sleep apnoea) had minor (n = 25) to moderate (n = 10) findings with the necessity for further consultation with the authorised doctor.
A total of 22 from all 80 patients (28%) had pulse-oximetry findings which did not correspond to the defined severity criteria regarding oximetry and pulse frequency and were evaluated as non-pathological (without findings). Twelve of these patients (55%) however showed sleep-specific symptoms (snoring, daytime sleepiness or ESS >10) and therefore required referrals for further tests. Faulty measurements did not occur (see Figure 2).
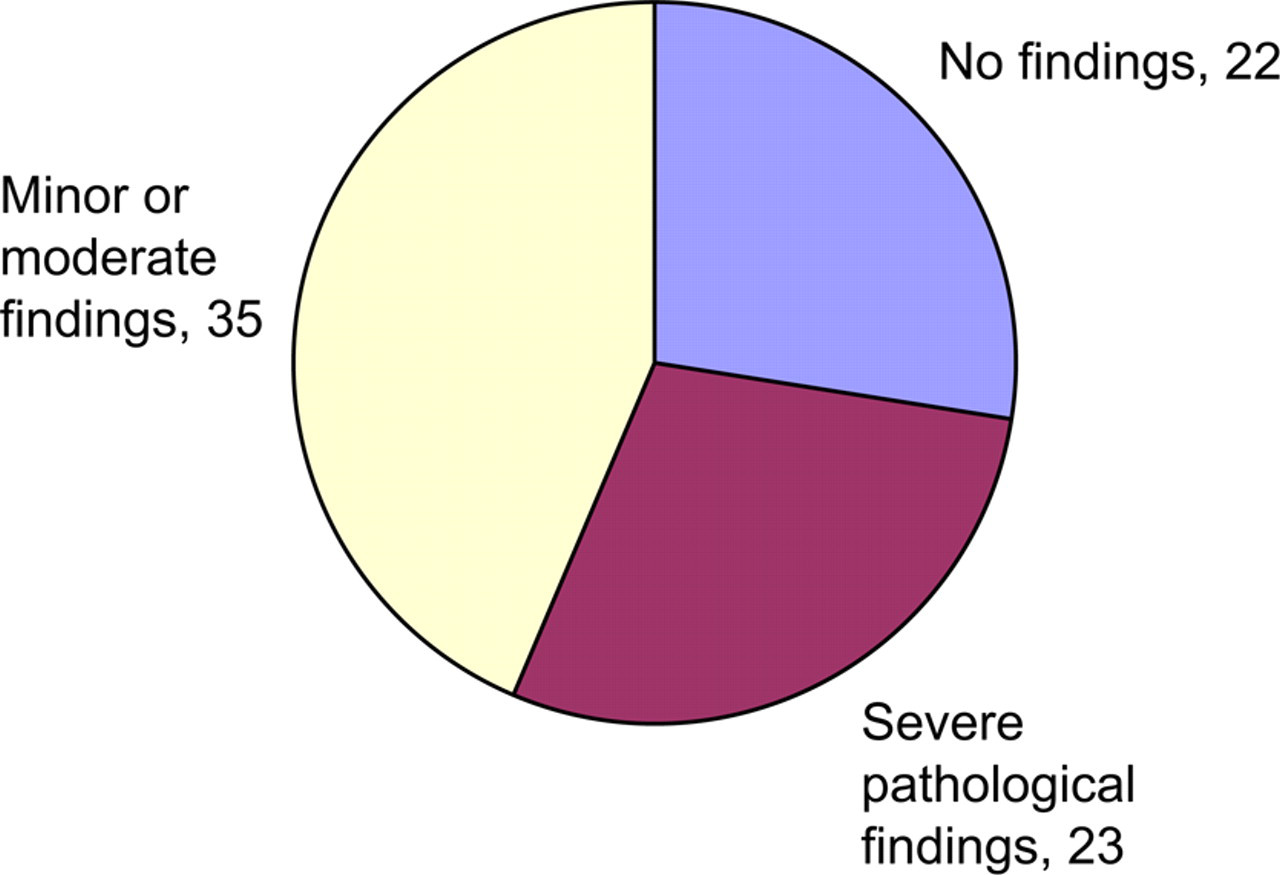
Findings in the patient group (n = 80)
In 14 patients who were examined with no associated diseases or symptoms found, 2 patients had moderate and 5 had minor findings with sleep apnoea being suspected.
To analyse the association between pre-existing cardiovascular diseases and the severity code of the pulse-oximetry, the diagnoses coronary heart disease, heart insufficiency, cardiac dysrhythmia and hypertension were grouped together. The correlations were positive throughout so that there was a positive link between the severity of the pathological finding and these attendant diseases. However, the correlation coefficient was low (r = 0.32). Adiposity with r = 0.63 had a stronger correlation, but it was not significant (P = 0.37). There was also a slight correlation with regard to daytime sleepiness with r = 0.44 and snoring with r = 0.40 (P = 0.6).
The ESS was applied only to a few patients. There were 7 ESS-scores without pathological finding (<10) in group 4 (with severely suspected sleep apnoea) and at the same time 4 clearly pathological ESS-scores (>11) in group 1 (oximetry without pathological finding and no suspected sleep apnoea) and also group 2 (minor suspected sleep apnoea) (see Table 1). A dependency in relation to the severity code was not identifiable.
The range of associated disease patterns did not reveal any obvious dependency on the severity code and in all three analysed groups there were patients without clear signs in the history. There was only a slight trend towards snoring in groups 3 and 4 (Group 1/Group 2 with 50% or 56% compared to group 3 with 80% or group 4 with 74%).
There was no data loss on any of the recordings and it was possible to evaluate all recordings. All patients accepted the sensor after a short trial period of use.
Discussion
Simple, easily applicable procedures may be useful for sleep diagnosis on a widespread basis by involving general practitioners and consultants, as well as non-medical institutions (e.g. pharmacies or – particularly in rural areas – mobile nursing services). A telemedical co-operation as described in the present study, can assist in the identification of asymptomatic patients and in preventative risk-screening for people with cardiovascular diseases or stroke/TIA, which would otherwise remain undetected. In this way the quality of patient care can be raised.
The telemedical iDoc-system used in the present study can assist in reducing referrals by identifying patients with strongly suspected OSAS. To interpret the findings from pulse-oximetry, co-operation with experienced sleep-medical specialists is of paramount importance. Only the qualified evaluation by a somnologist can help to avoid errors in analysis.
More widespread pre-screening will increase the requirement for further sleep-medical tests and therapy. However, from a cost-benefit point of view, gaining a tentative diagnosis at an early stage, will enable earlier diagnosis of sleep apnoea and therapy can be initiated earlier. The financial strain on the health-care system due to complicated cardiovascular comorbidities should be minimised. 13,14
Limitations
The present study had some limitations. For example, it lacked co-operation with certain specialties in which diagnosis for early risk prevention is also indicated, e.g. urology (erectile dysfunction), gynaecology (eclampsia), nephrology (renal failure), paediatrics (attention deficit hyperactivity syndrome/SRBD). The defined severity gradings and the pre-settings/ranges of the pulse-oximeter can also be regarded as limitations.
The system was developed for the identification of SRBD in respect of the typical cyclic saturation changes dependent on the airflow limitation. Low basic saturation values indicate other pulmonary diseases as obesity-hypoventilation-syndrome or COPD. In cases where daytime sleepiness has been identified as the main symptom, further sleep medical investigation will be required – even if pulse-oximetry has revealed no pathological findings. This is important in order to exclude or to differentiate other triggering diseases such as restless-leg-syndrome or upper-airway-resistance syndrome.
To compare the final results of polysomnography with those of oximetry it is necessary to examine sensitivity and specificity. This work is in progress.
Conclusion
Telemedical co-operation is an important element in the referral chain for sleep disorders. The telemedical evaluation of the night-time measurement does not require further training for the referrer, as the analysis is performed by a qualified sleep laboratory. The system described here is suitable for the creation of referral networks and for the identification of patients from institutions not trained in sleep medicine, who would otherwise not have been referred for specific diagnosis to a sleep laboratory.
Footnotes
Acknowledgements
We thank all doctors and patients who participated in the study. The study was supported by the iDoc-Institut for Telemedicine and Health Communication.