
Abstract
In January 2007, a telestroke system was established between a community hospital lacking a neurologist on call and a stroke centre 70 km away. The telestroke system allowed urgent remote evaluation of the patient by a specialized neurologist, supervised thrombolytic treatment or a decision for urgent transfer to the stroke centre. During the first year of operation of the telestroke system, we studied all acute ischaemic stroke patients admitted to the community hospital and compared the results with the previous year. Approximately the same number of acute stroke patients were admitted to the community hospital in each year (201 cases in 2006 and 198 in 2007). The telestroke system was activated 75 times in 2007, the number of stroke patients evaluated by a specialized neurologist increased (17% vs. 38%, P > 0.001) and interhospital transfers were reduced (17% vs. 6%, P = 0.001). The number of thrombolytic treatments was doubled: 4.5% (n = 9) in 2006 vs. 9.6% (n = 19, 12 of them in the community hospital) in 2007 (P = 0.073). The telestroke system also reduced the time to tPA treatment from symptom onset (210 vs. 162 min, P = 0.05) and increased the number of patients treated in the 0–3 hours window (40% vs. 63%, P = 0.09). Telemedicine improved the quality of care administered to acute stroke patients admitted to a community hospital and reduced the number of inter-hospital transfers.
Introduction
Stroke is the leading cause of long term disability, the second cause of dementia and the third cause of death in most industrialized countries. Despite this high social and economic burden, only moderate therapeutic progress has been made in the last few years. Only three measures have proved their efficacy in acute stroke care: urgent evaluation by a specialized neurologist 1 , admission to a Stroke Unit 2 and thrombolytic treatment with tPA within three hours of the onset of symptoms. 3 While the first two measures can benefit virtually any patient suffering a stroke, the success of thrombolysis depends on strict inclusion criteria that prevents its use in a large number of patients. Moreover, the use of tPA in hospitals which treat only a few cases each year can reduce its efficacy and even increase the mortality. 4
Because of the limited availability of expert specialized care in most community hospitals or rural areas, it is impossible to offer equity in access to health care. 5 Inter-hospital networks allow urgent transfer to a Stroke Centre of every patient suspected of suffering an acute stroke, i.e. expertise is concentrated at specific hospitals rather than spread throughout the entire network. These networks have been shown to increase the number of thrombolytic treatments. 6 However, equity is only partly improved at the expense of an excessive number of unnecessary ambulance transfers. 7
The combination of telemedicine systems with transfer policies may offer immediate expert neurological evaluation, on-site initiation of thrombolysis and accurate selection of the patients who may benefit from transfer to a Stroke Centre. 8,9 We have examined the impact of the implementation of a telemedicine system on care for acute stroke patients.
Methods
In January 2007, we initiated a telemedicine system linking a certified Stroke Centre with a community hospital located 70 km away where a neurologist on call was not available and where patients could not receive tPA treatment or be admitted to a Stroke Unit. The Stroke Centre offered access to a specialized neurologist 24 hours a day, a certified Stroke Unit and had vast experience in thrombolysis treatment.
Before telemedicine
Prior to the availability of telemedicine, and in accordance with the recommendations of the Brain Attack Coalition 10 and the institutional ‘Stroke guide for Catalunya’, an inter-hospital network was created allowing immediate urgent transfer to the Stroke Centre of every patient suspected of suffering an acute stroke in the community hospital. Patients were often transferred between the two centres and seminars were given to all physicians working in the community hospital emergency room. Physicians at the community hospital were advised to transfer patients to the Stroke Centre as emergencies if the time from onset was less than six hours or there was progressive neurological worsening. In doubtful cases physicians could consult the stroke-neurologist at the Stroke Centre by telephone. When patient transfer was decided on, the Stroke Centre was always pre-notified and the stroke code activated. 11 At the Stroke Centre, patients were immediately evaluated by a neurologist and the appropriate therapeutic intervention decided: thrombolytic treatment, admission to the Stroke Unit or return to the community hospital.
With telestroke system
The telestroke system consisted of a videoconference unit that allowed stroke experts at the Stroke Centre to see the patient and interact with physicians at the community hospital. The remotely controlled camera (Tandberg 880, Internet Protocol minimum bandwidth 512 kbit/s, image resolution 1024 × 768 pixels) allowed the neurologist to focus and zoom on different areas. Neuroimaging scans could also be remotely evaluated separately via PACS. When the telestroke system became available, physicians at the community hospital were instructed to teleconsult on the arrival of any suspected acute stroke patient to the emergency room (<6 hours from symptom onset). The patients' neurological status was assessed with the NIH stroke scale, and scores obtained at the bedside and remotely were recorded. Physicians at both sites could discuss the treatment options, including the need for urgent transfer for rescue therapies such as thrombolysis in the 3–6 hour window, intra-arterial procedures or decompressive craniectomy. Patients treated with tPA at the community hospital not eligible for transfer were admitted to the local ICU for close monitoring. In these cases the neurologist followed the progress of the patient with repeated teleconsultations in the following days if needed. In the 3–6 hour window, patient selection for thrombolytic treatment was decided according to an institutional protocol. 12 For tPA-treated patients we defined clinical improvement as a reduction of at least 4 points in the National Institute of Health Stroke Scale (NIHSS) at 24 hours. Complete neurological improvement was defined as NIHSS ≤ 1 at discharge.
For each patient, demographic and clinical data including decision to treat with tPA or transfer to Stroke Centre were recorded prospectively. If a transferred patient did not receive thrombolysis at the Stroke Centre and could be retransferred to the community hospital within 24 hours, the transfer was considered unnecessary. Four months after the telestroke system was launched, a satisfaction survey was done among community hospital physicians. The study was approved by the appropriate ethics committees.
Statistical analysis
Statistical analysis was performed using a standard package (SPSS 12.0). Statistical significance for inter-group differences for categorical variables was assessed by χ2 test or Fisher's exact test. For continuous variables, Student's t-test or the Mann-Whitney U test were used.
Results
A total of 201 acute stroke patients were admitted to the community hospital emergency room in 2006 and 198 were admitted in 2007. During the year the telemedicine system was activated in 75 cases (38%), after teleconsultation stroke diagnosis was confirmed in 97% of cases. Teleconsultations were made by 12 different physicians at the community hospital and were equally distributed during the day (Figure 1). The mean age of the patients was 75 years and the mean time from symptom onset was 151 min. The median NIHSS scores were 7 (bedside) and 8 (remote). The inter-rater agreement was excellent (kappa 0.98).
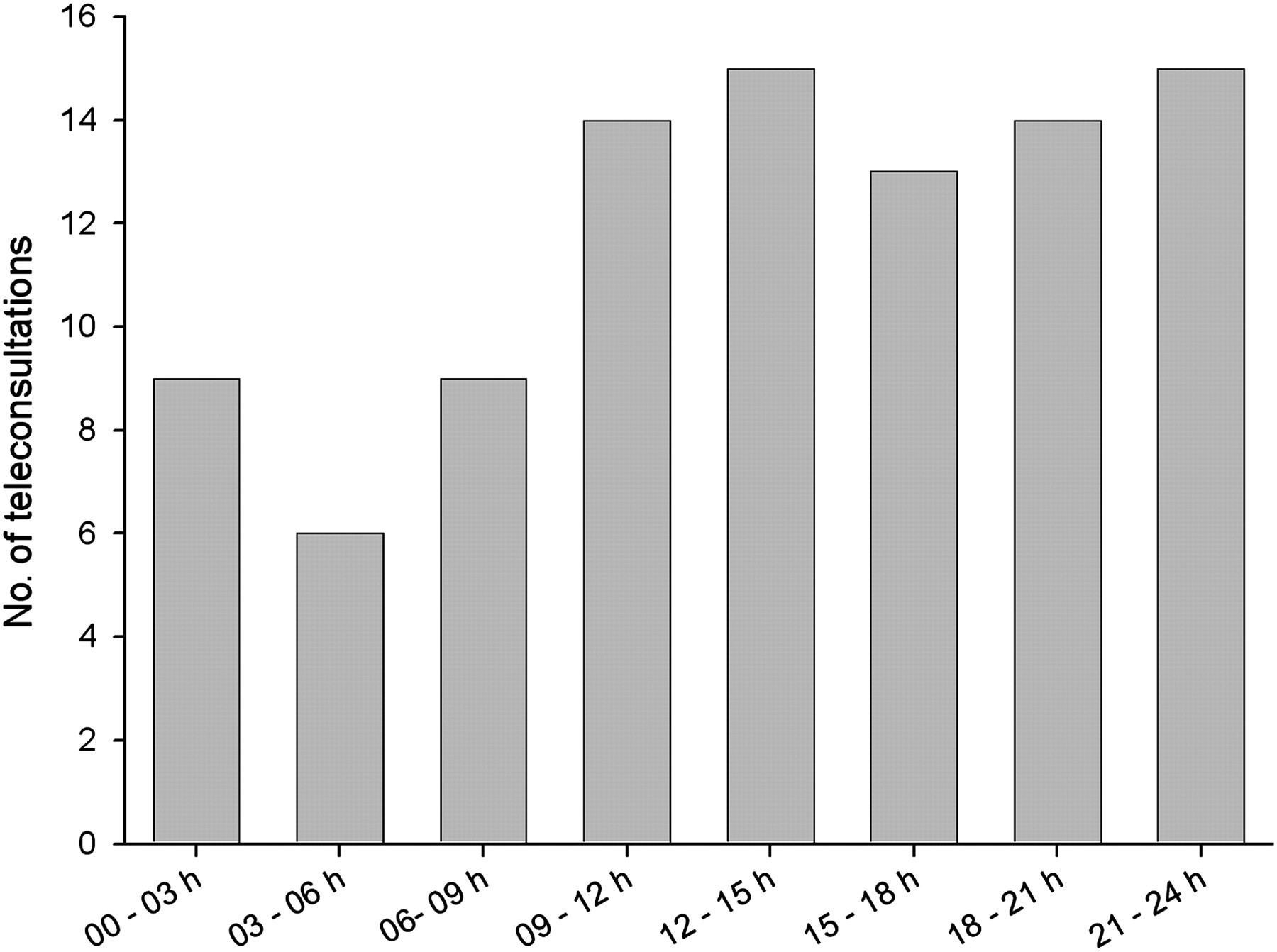
Distribution of teleconsultations according to time of the day
The proportion of patients transferred to the Stroke Centre dropped from 17% in 2006 to 10% in 2007 (P = 0.04). The proportion of patients urgently evaluated by a specialized neurologist increased from 17% in 2006 to 38% in 2007 (P < 0.001). After evaluation at the Stroke Centre the number of unnecessary transfers also fell, from 51% in 2006 to 20% in 2007 (P = 0.02). No differences were observed in the number of patients admitted to the Stroke Unit: 11% in 2006 and 8% in 2007 (P = 0.34) (Table 1).
Acute care measures received by stroke patients admitted to the community hospital
Thrombolytic treatment
The number of patients who received tPA treatment increased from 4.5% in 2006 to 9.6% in 2007 (P = 0.07) (see Table 1). The telestroke system made possible the supervised introduction of thrombolysis in the community hospital: 12 patients received intravenous tPA on site in 2007. The baseline characteristics for patients treated with tPA were similar in both years except for variables related to time (Table 2). The telestroke system allowed an important reduction in the time from symptom onset to tPA treatment: 210 min in 2006 vs. 162 min in 2007 (P = 0.05). The number of patients treated with tPA in the 0–3 hour window also increased from 30% in 2006 to 68% in 2007 (P = 0.04).
Characteristics of tPA-treated patients according to hospital of primary admission
*NIHSS: National Institute of Health Stroke Scale
The number of patients who benefited from thrombolysis achieving a clinical improvement was similar in both groups (70% in 2006 vs. 59% in 2007, P = 0.39). At discharge a similar number of patients achieved a complete neurological recovery (30% vs. 47%, P = 0.57). Rates of haemorrhagic transformation (20% vs. 22%, P = 0.89) and symptomatic haemorrhagic transformation were also similar (0% vs. 0%) (see Table 2).
Finally, the satisfaction survey at the community hospital revealed that the telestroke system was considered very helpful for the attending physician in terms of diagnosis and treatment decisions and provided an overall benefit for the patient.
Discussion
The telestroke system increased the number of patients urgently evaluated by a neurologist and treated with tPA. It also reduced the costs and inconvenience of ambulance transfers. During the first hours after stroke onset, ‘time is brain’ 13 and any measure that makes possible an urgent evaluation by a specialized vascular neurologist is likely to have a positive effect on clinical outcome. 1
In the last decade, following the approval of thrombolytic therapy, pre-hospital clinical pathways have been developed to increase the number of acute stroke patients arriving at the emergency room within the therapeutic three-hour time window. 6 An institutional health system solely based on urgent patient transfer to a central Stroke Centre may be able to increase the access to thrombolysis for patients living in rural areas. However this is far from being ideal as most of the patients will not be transferred and therefore evaluated by a stroke specialist. Moreover the potential benefit of thrombolysis may be blunted by a longer time to initial treatment in those patients living in remote areas. 7 The benefits of these networks rely also on an excessive number of unnecessary transfers which increases the costs, discomfort and may even harm patients by challenging blood pressure control and other therapies. The combination of telemedicine with transfer policies may be a useful approach as it offers immediate expert neurological evaluation of most patients, on-site initiation of thrombolysis where appropriate and accurate selection of patients who may benefit from a transfer to a Stroke Centre, 14 thus reducing the number of unnecessary journeys. These remote evaluation systems have been implemented successfully 15 and their spread in Europe is considered to have high priority. 16
Previous studies have shown that a neurologist working through a telestroke system can help to confirm the diagnosis of stroke and accurately measure the degree of neurological impairment, obtaining similar NIHSS scores as at the bedside. 17,18 The excellent correlation observed in NIHSS scores in our study validates the telemedical use of the Spanish version of this scale. The German TEMPIS telestroke network that links up to 12 community hospitals to Stroke Centres demonstrated a notable increase in the number of tPA-treated patients without safety concerns. 8 However, some quality indicators such as the rate of stroke patients treated with tPA or the door-to-needle time could not achieve the same quality levels as at the Stroke Centre. 9 Our study showed not only that a telestroke system can safely increase the rate of tPA-treated patients in a community hospital up to rates similar to most major stroke centres (10%), but also reduce the number of ambulance transfers, thus saving time and money.
In our study, teleconsultations were performed by 12 different physicians. The turnover rate of the attending staff in community hospitals is frequently high and hinders the training of stroke experts in the emergency departments of these hospitals. The results of the satisfaction survey among physicians at the community hospital showed that the telestroke system was not viewed as a time-consuming or meddling device, but rather as a valuable consulting tool.
There is strong evidence that admission to a specialized Stroke Unit results in lower rates of death, dependency and need for institutional care at discharge. 19,20 Despite the fact that the benefit of Stroke Units has been known since the 1980s, their adoption has been slow. In Europe, the proportion of acute stroke patients admitted to a Stroke Unit varies from 5 to 33% 21,22 despite the 1996 EUSI recommendations suggesting that all stroke patients should have access to a Stroke Unit by the end of 2005. 23 Our study showed that the implementation of a telestroke system did not significantly affect the number of patients admitted to a Stroke Unit. Physicians and health-care providers are urged to find different alternatives in order to meet the official recommendations.
Our study showed the benefits of a telestroke system for acute stroke patients in terms of access to excellence, therapeutic measures and the clinical effect on tPA-treated patients. The limited number of patients in our study showed an improvement in clinical processes more than in clinical outcome. However the increase in the number of patients having access to widely proven effective therapeutic measures can be considered as a surrogate marker of clinical outcome.
Telemedicine improves the quality of medical care and reduces the number of inter-hospital transfers of acute stroke patients admitted to a community hospital. A telemedicine system allows urgent expert evaluation and the supervised use of thrombolytic treatments in those centres lacking a neurologist on call. Health-care policies attempting to achieve equity of access to acute stroke care should consider the use of telemedicine systems.
Footnotes
Acknowledgements
This work was supported by a grant from the Instituto de Salud Carlos III: evaluación de tecnologías sanitarias (PI07/90607). We thank M Glòria Torras, Ismael Cerdà and the fundació I2CAT.