
Abstract
We evaluated two 12-week long community-based obesity control programmes in Korea. One was a visiting-type programme (V-type) (n = 515) administered by a public health centre and the other was a remote-type programme (R-type) (n = 410) utilizing an Internet website and mobile phones with a short message service. The total cost for the intention-to-treat subjects was US$116,993 in the V-type programme and $24,555 in the R-type programme. In the per-protocol subjects, 66% of V-type participants (n = 117) achieved the target bodyweight reduction (5%) and 13% of R-type participants (n = 15). In the per-protocol subjects, the cost per person was $227 (V-type) and $60 (R-type). The cost per person achieving the target weight reduction was $975 (V-type) and $1637 (R-type). The average amount that participants were willing to pay was $71 (V-type) and $21 (R-type). The cost-effectiveness of the visiting-type community-based, short-duration obesity control programme was higher than the remote-type programme.
Introduction
The third National Health and Nutrition Survey in Korea conducted in 2005 reported the prevalence of obesity as 32% in adults (obesity was defined as having a body mass index (BMI) ≥25 kg/m2), with gender prevalence of 35% in men and 28% in women. 1 Overweight Koreans have relatively high risks of hypertension, type 2 diabetes and hypercholesterolaemia, suggesting the need to curb increasing obesity rates. 2 Obesity is related to metabolic syndrome, and subjects with metabolic syndrome are at greater risk of developing cardiovascular disease and other problems. 3–5 Padwal et al. 6 reported that future health-care costs would be higher for persons who are overweight, especially those with BMI ≥30 kg/m2. In addition, there are large differences in health-care costs according to the degree of obesity. Overall, a BMI of 35–40 kg/m2 is associated with twice the health-care expenditure above normal weight and a BMI of 30–35 kg/m2 with a 25% increase. 7 Therefore, a nationwide obesity control programme is desirable to prevent future serious health problems and to reduce health-related costs.
Many public health centres in Korea have been conducting obesity-control programmes as part of health promotion projects. In Korea, as in many other countries, millions of people access the Internet via personal or mobile phones, and this can be exploited to deliver a telemedicine-based weight control programme. However, there have been no published reports on the cost-effectiveness of community-based obesity control programmes. A modest weight loss in the obese, considered to be 5–10% of bodyweight, is associated with improvements in cardiovascular risk profiles and reduced incidence of type 2 diabetes. 8–10
We calculated the cost-effectiveness of two different community-based obesity control programmes.
Methods
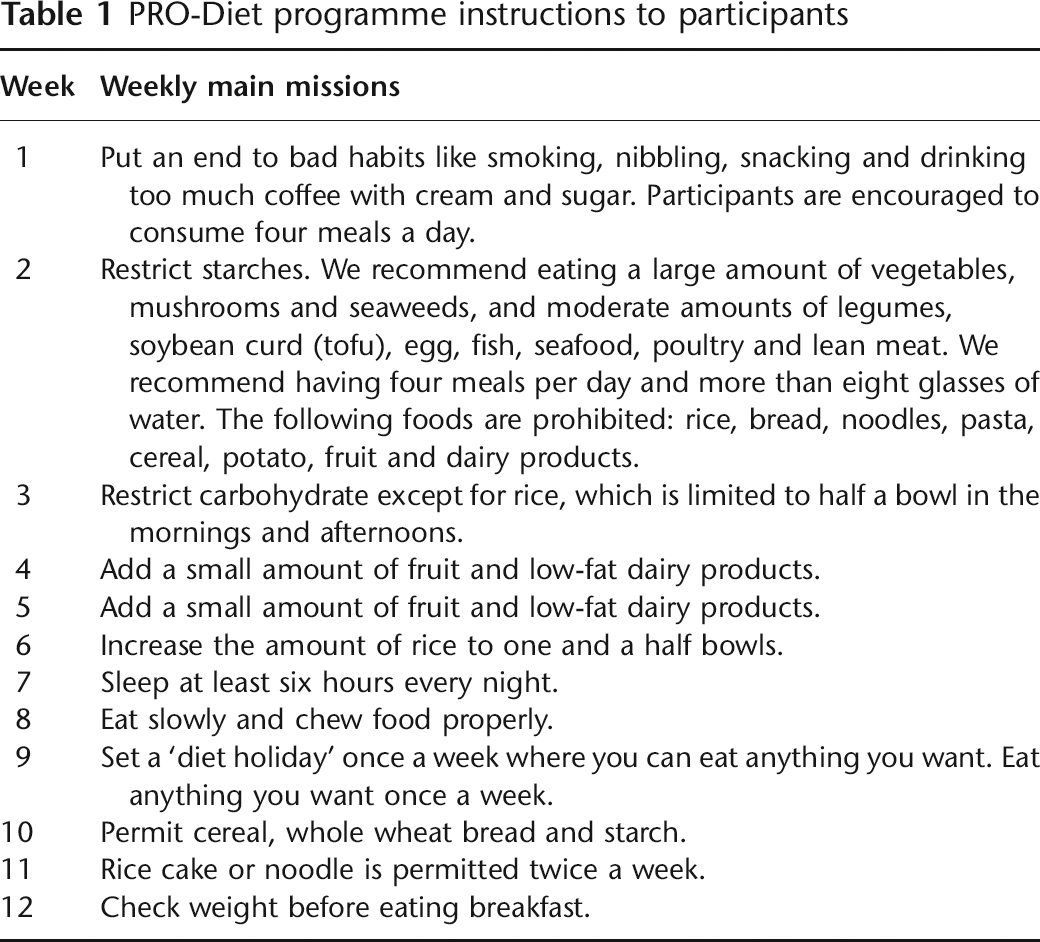
In the present study, the obesity control programmes used the Protein-Rich-Oriental Diet (PRO-Diet) regimen devised by Dr Yong-Woo Park (Reset Obesity Clinic, Seoul, Korea). The diet encourages consumption of low-saturated fat, high protein oriental foods (legumes, soybean curd, soy milk, mushrooms, nuts, seafood, fish, chicken breast and lean meat) and vegetables, while avoiding simple sugars, refined starches and high-saturated fats (see Table 1).
The study was approved by the appropriate ethics committee. From May–December 2007, we conducted a 12-week community-based obesity control programme in public health centres in two cities (Dongdoocheon and Ansan). Two types of obesity control methods were used. The first was the visiting type (V-type) which involved regular visits to the local public health centre, and the other was an Internet-based, remote type (R-type). In the V-type, participants regularly visited the public health centre at 1- or 2-week intervals for the 12-week duration of the programme, and were instructed on behaviour modification, nutrition and exercise to overcome the cause of obesity by registered nurses, nutritionists and exercise trainers. The participants were recruited by notices on local television channels and in newspapers. The inclusion criteria were BMI ≥25 kg/m2 (obesity is defined in Asia as BMI ≥25 kg/m2), age 20–64 years, overweight subjects who had central obesity (waist circumference of ≥90 cm for men and ≥85 cm for women) and aerobic exercise of at least 30 min in length 4 times a week. Exclusion criteria were uncontrolled type 2 diabetes, hypertension, habitual consumption of alcohol, cancer, history of stroke and renal disease.
Height and bodyweight were measured with minimum clothing and without shoes. Waist circumference was measured between the lower rib and iliac crest by trained nurses. Blood pressure was measured oscillometrically (TM-2655P, PMS Instruments, Tokyo, Japan) after at least 15 min of rest. Body composition was measured by body impedance analysis (In body ver. 7.0 software, Biospace, Seoul, Korea). Additional analyses for V-type subjects included standard enzymatic measurements of total cholesterol, high-density lipoprotein cholesterol, triglycerides and fasting glucose that were carried out on fresh serum samples (TBA-200FR, Toshiba, Tokyo, Japan) at the beginning and end of the programme. Participants were also asked to complete a questionnaire (response rate 34%) and nutritional status was ascertained by asking participants to record their diet for three days prior and three days following the programme. Macronutrient changes were revealed by analysis of each food diary (CAN-Pro 3.0 nutrition software, Korean Nutrition Society, Seoul, Korea).
For the R-type programme, subjects were recruited by visiting several middle and high
schools in the two cities. In registering R-type subjects, anthropometry characteristics
such as bodyweight, waist circumference, height and blood pressure similar to V-type,
and body composition were determined as described above. Participants received the same
educational information described above, and in addition received two weekly short
message service (SMS) prompts for behaviour modification
11
and were required to access the study Internet website (
Cost-effectiveness and willingness to pay
The cost of the V- and R-type programmes (US$) was summed to compare the cost per person in both types, and a simple cost-effectiveness ratio (total cost/numbers of target bodyweight achievement) was calculated. The target bodyweight was a 5% reduction of the initial bodyweight; therefore, the rate of target bodyweight achieved was the proportion of the total numbers of subjects who had achieved the target bodyweight in the per-protocol subjects in each programme.
Concerning willingness to pay, we gathered data in the self-reported questionnaires submitted at the end of the study by an open-ended method, which allowed determination of the average cost that participants were willingly to pay to take part in the community-based obesity control programme. We calculated the average cost at which the participants indicated that they would have been satisfied. Income levels were not considered, although we did assess the participation of unemployed, middle class income level housewives in the V-type programme. R-type participants were all school teachers, which automatically grouped them socioeconomically in at least the middle class. Sensitivity analysis was done after inclusion of only the essential costs of managing the 12-week programme. The V-type analysis also included and excluded the aforementioned costs.
PRO-Diet programme instructions to participants
Statistics
A general linear model (ANCOVA) was used to evaluate the significance of age, initial bodyweight, waist circumference, body fat mass, fat % mass and fat-free mass between the two groups. A standard software package was used (SPSS, ver. 11.5, SPSS, Chicago, IL).
Results
A total of 515 subjects were recruited to the V-type programme and a total of 410 subjects to the R-type. The numbers of V- and R-type subjects in the per-protocol groups were 177 and 120, respectively. The number of V- and R-type subjects in the intention-to-treat groups were 338 and 290, respectively.
Baseline characteristics
The mean age, BMI, waist circumference, body fat, % body fat and fat-free mass of the V-type subjects were significantly higher than those of the R-types, while bodyweight and height were significant lower. The proportion of V-type females was higher than that of R-type in both the intention-to-treat and per-protocol groups (Table 2).
Baseline characteristics of the subjects in the two programmes. Values are mean (SD)
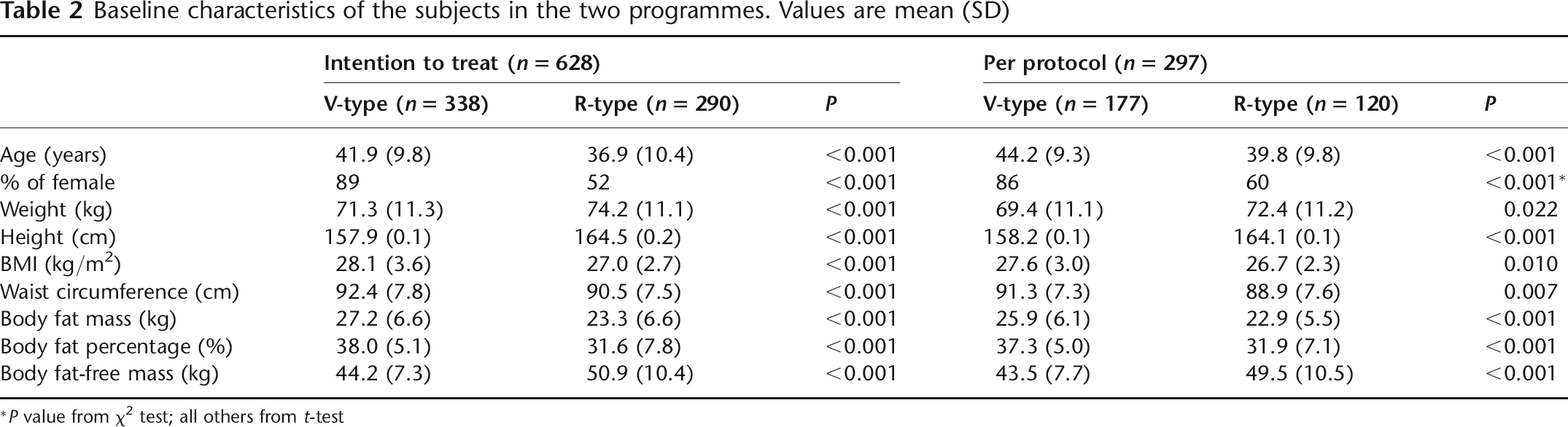
*P value from χ2 test; all others from t-test
Anthropometric changes
After 12 weeks of intervention, subjects in the per-protocol group displayed significant changes of body composition. In the 177 V-type participants, the mean changes in bodyweight, BMI and waist circumference were −4.7 kg, −1.9 kg/m2 and −6.7 cm, respectively. For the 120 R-type participants, the mean changes of bodyweight, BMI and waist circumference were −1.1 kg, −0.4 kg/m2 and −2.6 cm, respectively (Table 3). Because there were many baseline differences between the two groups, we compared them after adjusting for age, gender, initial bodyweight, BMI, waist circumference, body fat and fat-free mass. In spite of adjusting for these baseline characteristics, the mean changes in the V-type participants remained significant.
Anthropometric changes in the per-protocol groups after 12 weeks. Values are mean (SD)
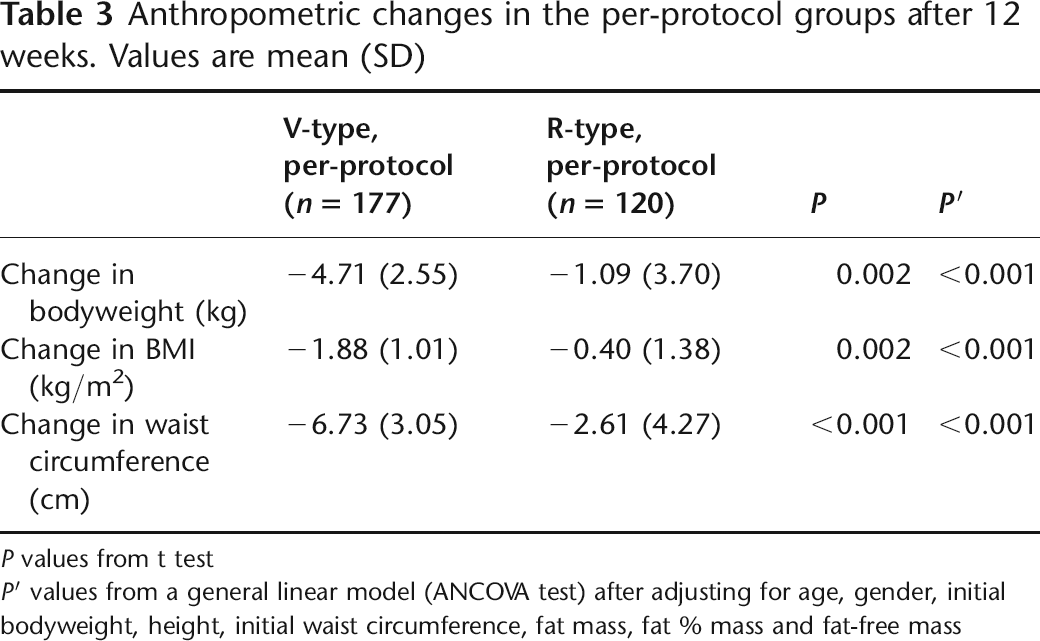
P values from t test
P′ values from a general linear model (ANCOVA test) after adjusting for age, gender, initial bodyweight, height, initial waist circumference, fat mass, fat % mass and fat-free mass
Cost analysis and willingness to pay
In the V-type programme (n = 515), the total cost comprised personnel cost, equipment purchase costs, laboratory test costs and other costs; this amounted to approximately $116,993. In the R-type programme (n = 410) the total cost comprised website development and upgrades, and personnel costs, which amounted to approximately $24,555. The essential cost of both intention-to-treat groups (eliminating other costs, such as disposable items) was $114,154 and $24,555 for the V-type and R-type programmes, respectively (Table 4).
Estimated cost in the intention-to-treat groups
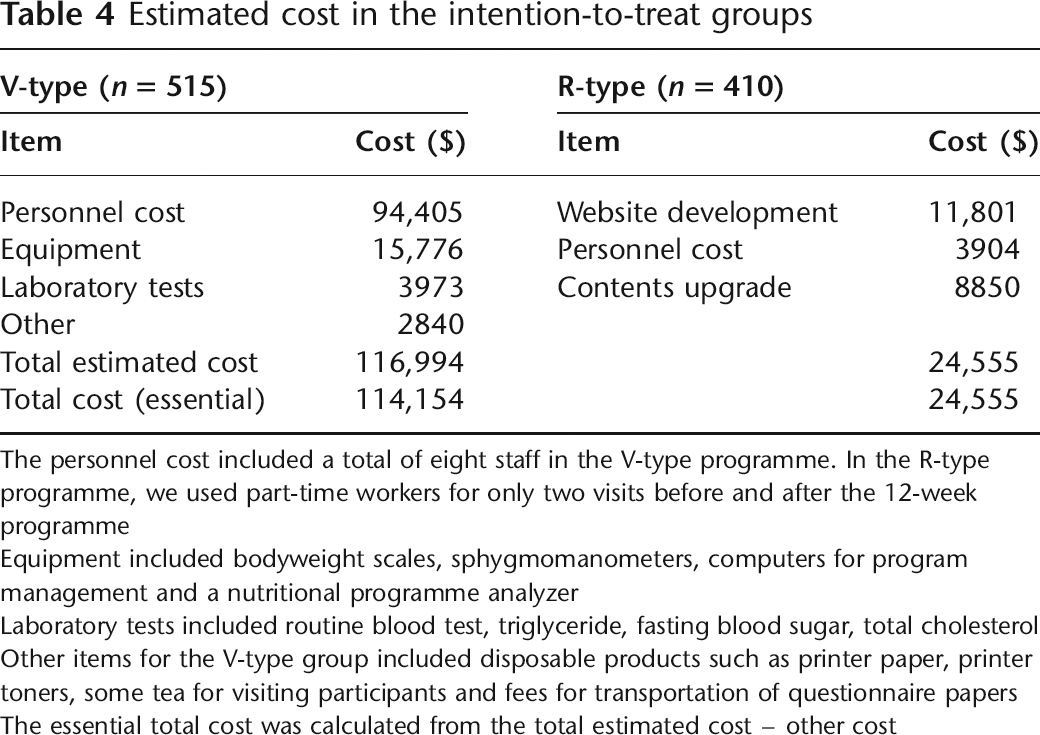
The personnel cost included a total of eight staff in the V-type programme. In the R-type programme, we used part-time workers for only two visits before and after the 12-week programme
Equipment included bodyweight scales, sphygmomanometers, computers for program management and a nutritional programme analyzer
Laboratory tests included routine blood test, triglyceride, fasting blood sugar, total cholesterol
Other items for the V-type group included disposable products such as printer paper, printer toners, some tea for visiting participants and fees for transportation of questionnaire papers The essential total cost was calculated from the total estimated cost – other cost
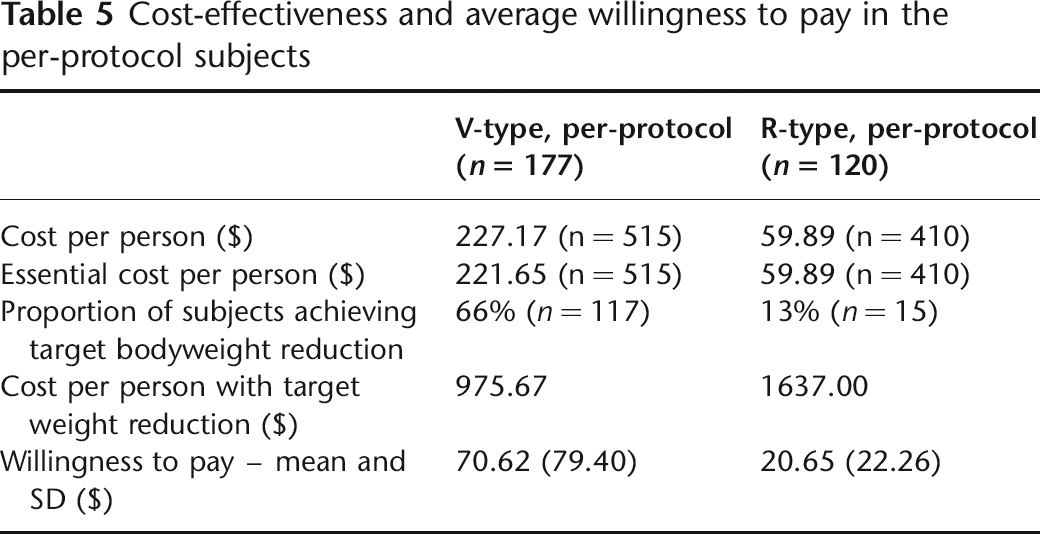
For the intention-to-treat subjects in the two programmes, the cost was $227 per person for V-type and $60 per person for R-type. For the per-protocol subjects, 66% of V-type subjects achieved the target bodyweight reduction (n = 117) and 13% of the R-type subjects (n = 15). Thus the essential cost for people who achieved the target bodyweight reduction was $975 per person in V-type and $1637 per person in R-type. The higher willingness to pay of $71 for V-type participants than the $21 for R-type participants was evidence of a greater degree of V-type participant satisfaction (Table 5).
Cost-effectiveness and average willingness to pay in the per-protocol subjects
Discussion
While community-based public health obesity control programmes have been operating in Korea for several years, information on the performance of the different approaches is lacking, particularly concerning cost-effectiveness. The present small-scale investigation indicates that regular visits to a public health centre offering the programme (V-type) are more cost-effective ($975/person achieving target bodyweight reduction vs $1637/person achieving target bodyweight reduction) and produce greater participant satisfaction, in terms of willingness to pay, than the remote type approach (R-type) based on mobile phone messaging and the Internet. Furthermore, per-protocol analysis demonstrated that achieving the target bodyweight reduction occurred more frequently in the V-type programme than in the R-type.
An intensive prevention programme incorporating group lifestyle modification practices and the use of generic medication can be cost-effective. As an example, one study on a type 2 diabetes prevention programme documented a lifetime cost-effectiveness of $8800/quality-adjusted life year (QALY) and $29,900/QALY, respectively. 12 In obesity control/prevention, several cost-effectiveness reports have been published concerning group and mixed family-based treatment for childhood obesity, 13 clinical and cost-effectiveness of surgery for morbid obesity, 14 and a new approach to assess health benefits from obesity interventions in children and adolescents. 15 However, no reports have been published on community-based obesity control programmes aimed at adults.
In our previous study on a community-based obesity control programme, 11 we used only mobile phone SMS delivery as the instrument of behaviour modification. Even though the number of participants was small, the results indicated a potential benefit of the approach for the control of bodyweight in community. Many health-promotion programmes aimed at obesity control have been conducted in public health centres in Korea in an effort to curb the growing obesity rate. However, these initiatives have been hampered by budgetary limitations and lack of staff. This is frustrating, as the need for obesity control is pressing, especially for those of lower socioeconomic status, and this effect is highly consistent among women but less consistent among men. 16 Yoon et al. noted significant dose-response relationships between income and obesity in men. 17 Another persuasive reason for community-based obesity control programmes is the increasing prevalence of obesity in the middle-aged population in Korea. 1
Limitations
There were some limitations in our study. For example, the short duration of the intervention period (12 weeks) made it impossible to calculate QALYs; only the simple cost-effectiveness ratio could be used to evaluate the two programmes. Second, the recruitment of participants from only two cities in Korea could have introduced a selection bias. Furthermore, there was little diversity in age, income levels and other indicators of socioeconomic status which might reveal differences in willingness to pay. In addition, the laboratory tests and other analyses involved in the V-type programme might have produced differences that would otherwise not have been apparent had similar testing been done on R-type participants.
Per-protocol and intention-to-treat numbers were relatively low because some subjects who enrolled at baseline dropped out and some did not visit the public health centre on the final assessment day for various private reasons. Also the programmes were not compulsory and there was no reward for completing them.
Future work
The short duration of the study hampered the accurate determination of programme cost-effectiveness. A longer duration programme involving more precise monitoring might reveal an increased cost-effectiveness of the R-type approach. In fact, the V-type programme of the present study was based on face-to-face education at individual and group level, while the R-type did not provide this, which reduced its cost. Participation in Internet-based obesity control programmes may be expected to increase in the future.
In conclusion, the cost-effectiveness of the visiting type short-duration obesity control programme offered by a public health centre was higher than a remote type programme.
Footnotes
Acknowledgements
The obesity control programme was funded by the Gyeonggi Provincial Office, 2007, and conducted in two public health centres in Dongdoocheon and Ansan, Gyeonggi-do, Republic of Korea. We thank Biospace for the use of the body impedance analysis equipment. We thank the registered nurse, dieticians, exercise trainers and secretaries in the two public health centers. We are grateful to Professor SS Shin, Ajou University School of Medicine, for comments on the analysis of the cost-effectiveness and Professor KH Chun, Graduate School of Public Health, Ajou University, for comments on the willingness to pay.