
Abstract
We examined videoconferencing in comparison with face-to-face office visits in primary care. Four physicians took part in the study and 175 patients were recruited from a general medical practice. Patients were interviewed and examined in both face-to-face and virtual settings, the order being randomized. Patients and clinicians were surveyed by questionnaire after each visit. Physicians were very satisfied with videoconferencing but preferred face-to-face overall (P < 0.0001). For videoconferencing, the physical examination and the ability to order appropriate laboratory tests were the least satisfying elements of the encounter. Patients were also very satisfied with videoconferencing but overall preferred face-to-face (P < 0.0001). This difference was significant for gastrointestinal, musculoskeletal and respiratory complaints. However, in terms of willingness to pay (WTP) for videoconferencing access, patients with musculoskeletal and respiratory complaints were the most willing. Age and gender did not significantly predict WTP. The technical quality of the videoconference had a significant effect on satisfaction with the clinical encounter but did not correlate with the patients' WTP for videoconferencing. Travel costs up to $40 and travel times up to 4 hours did not influence the WTP of patients. For non-rural, relatively mobile patients, videoconferencing appears suitable for short visits for relatively simple complaints.
Introduction
Videoconferencing has been relatively little used in primary care work. We have investigated the use of low-cost videoconferencing equipment, i.e. based on PCs with web cameras. We also examined patients' willingness to pay (WTP) for this form of access. 1 WTP is a standard method for eliciting patient preferences. WTP is the maximum amount a person is willing to pay for a good or service. This WTP may be in the form of out-of-pocket expense or in terms of proxies such as travel time. WTP can be elicited via open-ended questions, through binary options like standard gamble elicitation, or through bidding. People's WTP has been shown to correlate with the value they place on education, income and health care. 2–4
The present paper reports information gathered on this topic during a randomized controlled trial which compared videoconferenced visits to face-to-face encounters.
5
The objectives of the present study were to examine the feasibility, effectiveness and acceptability of a face-to-face office visit compared to a videoconference visit. We examined:
The physician's ability to diagnose and treat in both modes; The acceptability of videoconferencing to patients and clinicians; The conditions where evaluation via videoconferencing was acceptable to clinicians; How much patients might value access to this service and for what kinds of conditions.
Methods
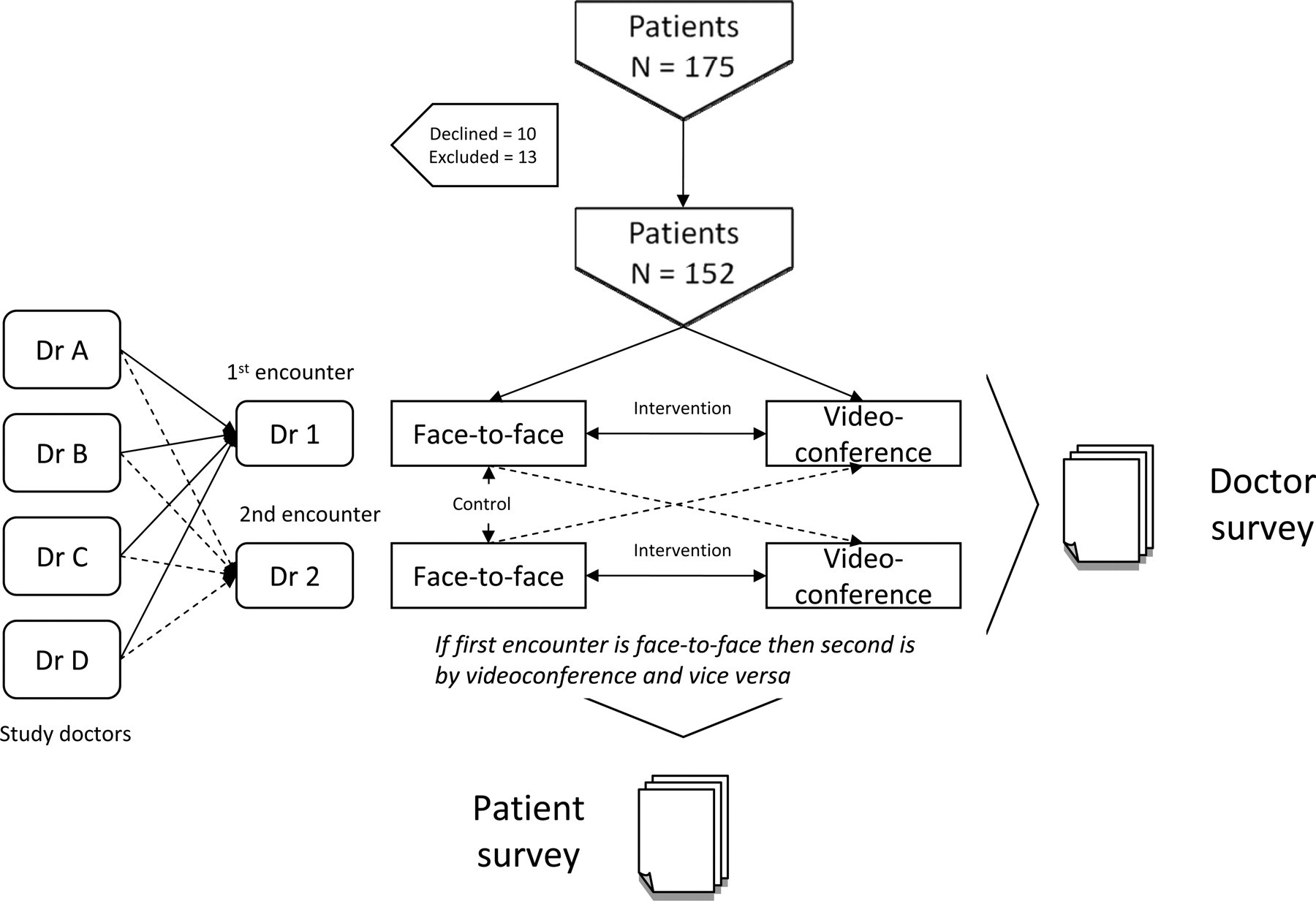
A randomized cross-over design was used. 5 Once patients were enrolled, they were randomized to one or other arm of the study (see Figure 1). They then completed a visit with a primary care physician, either by videoconference (V) or face-to-face (FF). After the first visit, both patients and physicians completed an evaluation questionnaire. The patients then completed a second visit via the other modality with another physician in a separate examination room in the same clinic on the same day. Patients and physicians then completed a second questionnaire. A control group of patients had both visits in the face-to-face modality with two different physicians. Four physicians participated in the study and conducted all visits. The study was approved by the appropriate ethics committee.
Study design
Between September 2007 and March 2008, 175 sequential patients (aged 18–85 years) were recruited from an adult primary care practice in Boston. Patients were invited to participate when they arrived at the physician's office. To qualify for inclusion in the study, subjects were required to be existing patients in the physician's practice. Patients were excluded if, in the physicians' judgement, the patient required emergency medical attention. After recruitment, the patients were randomized to a face-to-face clinical encounter followed by a videoconferenced clinical encounter, or the reverse. Four physicians were randomized to either the first or second patient encounter with the patient.
Web cameras were installed on the desktop computers in the primary care offices. The web cameras (Quickcam Fusion, Logitech) were used in conjunction with desktop videoconferencing software (version 8.02, Polycom). The speed of transmission was 384 kbit/s.
For a videoconferenced visit, patients were positioned in front of the web camera and the physician conducted the visit via the video system. During the encounter, the physician took a history, carried out a physical examination (although this was limited to visual inspection), decided on management and then arranged follow-up care if required. During the virtual examination, patients were asked to describe and point to the affected area or move the camera to focus on the affected area. They were instructed how to do this by their physician during the visit. Subjects did not receive training or instruction prior to the videoconference. Once the visit was completed, the physician and patient completed evaluation questionnaires about the visit in separate rooms.
The initial visit was followed immediately by a second visit, using the other modality, with a different physician. This second encounter was also followed by the patient and the physician completing evaluation questionnaires.
In addition to the questionnaire information, the following information was collected for each patient by the physician: age, gender, diagnoses (up to five), chief complaint, whether a new diagnosis was made during the encounter and whether new therapy was initiated during the encounter. In addition, questions relating to satisfaction, quality and the patient-doctor interaction were elicited using Likert scales ranging from 1 = poor to 5 = excellent. The questions relating to WTP were framed in terms of ranges of out-of-pocket expense, for example, 0–$10, $11–$20, $21–$30.
The key outcomes were satisfaction, perception of quality and WTP.
Results
Of the 175 patients who were invited to participate, 10 declined due to the extra time required, and 13 were excluded because of a primary gynaecological or urological complaint requiring a physical examination, leaving a final total of 152. The numbers of patients in the study arms was control FF:FF = 47, intervention FF:V = 37 and V:FF = 68. An overall comparison between face-to-face visits and videoconference visits with regard to clinical decision making and physician agreement has been reported elsewhere. 5
The mean age of the patients was 46 years (range 22–84). Forty percent were male. The most frequent chief complaints and primary diagnoses concerned: cardiovascular, musculoskeletal, gastroenterology, respiratory, gynaecological/urology or ear, nose and throat systems (see Table 1).
Chief complaints. Numbers in the categories of dermatology and laboratory abnormality were too small for subset analysis
Physician preferences
The overall physician satisfaction showed a significant preference for face-to-face consultation. However, physicians rated their overall satisfaction with videoconferencing highly (4.8 vs. 4.3, P < 0.0001). When considered by diagnostic category, physicians found the physical examination capabilities in the videoconferencing mode to be the least satisfying. Physicians also felt less satisfied with their ability to choose and order appropriate laboratory tests in the videoconferencing mode. Despite these differences, clinicians found practically no difference in their ability to conduct excellent histories (i.e. Likert scale 4 = good to 5 = excellent) via videoconferencing (see Table 2).
Doctor satisfaction with diagnostic category. All comparisons were performed using a two-tailed t-test
ns = P ≥ 0.05
Patient preferences
Patients were consistently more satisfied with face-to-face visits than with videoconference visits (4.6 to 4.3, P < 0.0001). When considered by diagnostic category, this was significant for gastrointestinal, musculoskeletal and respiratory complaints. However, the WTP measure was highest for videoconference access in the case of musculoskeletal and respiratory complaints, while patients were least willing to pay for access in the case of gastrointestinal and cardiovascular complaints (see Table 3).
Patient satisfaction with diagnostic category and WTP for videoconferencing. All comparisons were performed using a two-tailed t-test
ns = P ≥ 0.05
When comparing new to chronic problems, there was a trend for patients to be less satisfied with videoconferencing for chronic complaints (P = 0.1). As the number of prior visits for the complaint increased (i.e. patients with chronic problems), the less satisfied they were with videoconferencing.
Demographics
Age and gender were not significantly associated with patient responses to videoconferencing. There was no significant difference between men and women with regard to overall satisfaction with videoconferencing or with WTP, although there was a non-significant trend for men being more willing to pay for videoconferencing (the mean for men was $22.20 compared with $18.12 for women).
Technical quality
The satisfaction with the clinical encounter was significantly related to the technical quality of the videoconference. There was no significant relation with the patients' WTP for the service (see Table 4). There was a significant correlation between the overall comfort of the physician with the technology and their satisfaction with the encounter. The patients' perception of the overall comfort of the physician with the technology was also correlated with the patient's satisfaction with the encounter (P < 0.0001).
Satisfaction with the technical quality of the videoconference
Doctor-patient interaction
Another element which presumably contributed to satisfaction was the quality of the doctor-patient interaction as manifested by attention, communication, clinical skills and overall comportment. There was a trend in WTP for attention given to patient (see Table 5).
Quality of doctor-patient interaction. All comparisons were performed using a two-tailed t-test
ns = P ≥ 0.05
Diagnoses and therapies
Overall satisfaction rose slightly with the number of concurrent chronic diagnoses (Satisfaction = 4.38 + 0.08*number of diagnoses, r2 = 0.02, P = 0.01). Satisfaction with videoconferencing declined if either a new diagnosis was made (4.5 vs. 4.5, P = 0.2) or a new therapy was started (4.2 vs. 4.5, P = 0.01).
Travel and personal costs
Monetary travel costs or costs in terms of travel time did not appear to significantly influence the patients' overall satisfaction or WTP through the range reported (up to $40 and up to 4 hours). In addition, losing time from work or needing childcare did not influence WTP. Overall satisfaction was slightly less if childcare was needed (4.4 vs. 4.7, P = 0.1), although there was no change in WTP. Comments in the survey indicated that most patients took sick days to come to the clinic or had established childcare services. However, when a patient's support system (family and friends) was involved in facilitating the appointment, WTP for videoconferencing access rose from $18 to $26 (P = 0.1) (Table 6). When non-work related personal time was curtailed, the WTP for videoconferencing also increased, although this was not significant. Most people agreed that this should be paid for by insurance rather than out of pocket. Those that thought insurance should pay priced it at $23 (P < 0.01). There was no significant change in WTP for being away from work for patients having to pay for travel costs.
Costs to patient and support system
Order of visit type and diagnostic category
To examine whether or not the order of visit modality or the diagnostic category, influenced either patient or physician satisfaction with videoconference visits, we constructed regression models predicting the difference in satisfaction between the two modes of clinical interaction. In the regression model, the order of intervention was not significant, suggesting equal satisfaction with the two modes of clinical interaction. However, the diagnostic categories as a whole helped to explain the differences in satisfaction between the two modalities, indicating that videoconferencing was better suited for some conditions than others. The explanatory effect of diagnostic category was stronger for patients than physicians (data not shown).
Discussion
The present study suggests that videoconferencing may be useful in primary care consulting. The results indicate that both patients and doctors were generally satisfied with videoconferencing, although face-to-face interaction was preferred. Videoconferencing appeared to be better suited for some kinds of complaints than others, which is consistent with previous work showing that telemedicine can influence both the style and the effectiveness of patient-doctor communication. 6–8
In the group we studied it appears that, as measured by WTP and satisfaction, videoconferencing was preferred for short discrete problems rather than problems requiring repeated visits. This contrasts with a chronic care model of telemedicine, where telemedicine was thought to be most beneficial for chronic care management, for diseases such as heart failure. 9,10 One could hypothesize that the patients are making a rational decision, recognizing that telemedicine applications have a lower rate of information transfer between physicians and patients. It is possible that this difference is deemed important by patients in managing the subtleties of their care.
In our study, the cost or time required for travel did not seem to make a major difference in WTP for a telemedicine visit. This may have been partly due to the travel times being relatively short, as our patients lived in metropolitan, not rural areas. They were also relatively healthy and did not have any chronic conditions sufficiently severe to make it difficult for them to travel. This may be a limitation of our study, since telemedicine is often directed at rural patients or those requiring chronic care. However, we feel that the local outpatient setting has great potential for the use of videoconferencing as the technology becomes cheaper.
Another reason that the influence of travel costs on WTP may have been blunted is that our population was partly shielded from out of pocket costs, because their parking was free. In addition, patients are accustomed to co-payment, which may have anchored their responses. (In the future it may be better to frame WTP questions as trade-offs, with co-pays or deductibles, to get closer to what people are actually willing to pay.) However, when the costs were framed as lost family, friend or personal time, patients were more willing to pay for the videoconferencing service. Finally, when asked if their insurance should pay for the service, the majority agreed. Valuing the service from a clinician's perspective versus a payor's perspective remains a challenge in creating viable business models for this type of clinical activity.
Some of the strongest predictors for clinician preference or lack thereof were related to the core activities of the clinician: the history-taking and the physical examination. Videoconferencing provides a satisfactory way for obtaining the history of present illness. However, when a clinical examination or laboratory test is deemed necessary videoconferencing becomes less acceptable, despite evidence that it does not impair clinical decision-making. While technical quality influenced patient satisfaction with the visit it was not sufficiently distracting to alter their WTP for the service. What was far more significant to the patient was the perception that the physician was paying attention to what was said, taking time to explain what the clinical plan was, and the quality of the physicians' clinical skills and manner.
In conclusion, it appears that videoconferencing in the outpatient setting is useful, and both patients and clinicians are willing and able to use it. However, it is not a panacea which can replace all other forms of clinical access. Rather, in the non-rural environment and for relatively mobile patients, it is likely to be most suitable for short visits for relatively simple non-chronic problems (e.g. patients receiving care in an open access model where same-day appointments are guaranteed) or in an urgent care setting.
Footnotes
Acknowledgements
The study was supported by the Massachusetts General Physicians Organization.