
Abstract
We developed a hands-free portable device which can provide two-way, real-time audio and video communication between hospital doctors and emergency medical technicians (EMTs) providing pre-hospital care. The device was based on an ultra mobile PC with a camera, a microphone/earphone set and a WIBRO modem for wireless Internet connection at an average data transmission rate of 1 Mbit/s. Feasibility tests were conducted in 55 real emergency situations over a period of three months at five different Rescue Centres in Seoul. Successful communication between an EMT and a doctor was achieved in 46 cases (84%). The device showed acceptable performance in terms of audio/video transmission time delays and maximum transmitted video frame rates, both outdoors, inside a building and in a moving vehicle at 70 km/h. Eight control centre staff and 11 EMTs who used the device completed a questionnaire. Despite acceptable basic performance, the device was found to be limited in terms of the contribution it made to the medical control of EMTs. However, improvements in device performance should produce higher quality pre-hospital emergency medical care in the future.
Introduction
The Korean emergency medical service is a publicly operated system which provides emergency medical technicians (EMT) who are trained in basic life support. There are two levels of EMTs, namely, EMT-1 and EMT-2, and their roles are limited to basic procedures (Table 1). Advanced level procedures, such as endotracheal intubation and intravenous cannulation, must be performed under the control of a doctor. However, no emergency system capable of providing pre-hospital medical control has been established in Korea. In 2006, only 37% of patients received proper emergency medical care at the pre-hospital stage. 1 In other words, patients are seldom treated appropriately during the pre-hospital stage.
Roles of EMT-1 and EMT-2
Improved pre-hospital medical care requires the medical supervision of EMTs, directly or indirectly. Direct control means the supervision by a doctor of treatment administered by an EMT, whereas indirect control involves appropriate training and education of the EMT. In the context of direct control, various transmission methods have been developed, including the Global System for Mobile communication (GSM), 2 radio frequency (RF) wireless telecommunication, 3–6 satellite communication 7 and the Integrated Services Digital Network (ISDN). 8 These devices can be used to transmit audio and video information to and from a doctor. However, the use of such devices is often restricted, so for example a patient must be moved to a fixed location like an ambulance or a camera position. If such devices were more portable, doctors could guide EMTs more easily and patients would be treated more efficiently. However, to our knowledge, there have been no reports of the use of a portable wireless transmission device for medical control in emergency medical services.
Wireless Broad Band Internet (WIBRO), a form of mobile Worldwide Interoperability for Microwave Access (WIMAX), is a newly commercialized wireless Internet service in Korea. WIBRO provides an average data transmission rate of 1 Mbit/s, even in a vehicle moving at 90 km/h, and a small WIBRO modem connected to a portable PC enables the Internet to be accessed. Thus, if EMTs could use the WIBRO service, they could communicate with doctors from inside a building or from an ambulance. We have developed a hands-free portable device which can provide two-way, real-time audio and video communication between EMTs and doctors by utilizing the WIBRO service.
Methods
The device consists of a portable computer, a portable camera attached to goggles, a microphone, an earphone and a WIBRO modem (Figure 1). The camera (Talkcam MX6, V-Gear, China) is attached to goggles (S-506V, OTOS, Korea), so that when the goggles are worn, the camera captures the visual field of the user. The camera provides 1280 × 1024 pixel resolution at 30 frames per second, and has an auto-focusing function, which operates from 4 cm. The WIBRO modem (KWD-U1300, KT, Korea) weighs only 20 g and has dimensions of 7.7 × 3.1 × 1.2 cm. The camera and the WIBRO modem are connected to an ultra mobile PC (B1SE, Wibrain, Korea) via USB ports. This mobile PC weighs 500 g and has dimensions of 19.2 × 8.2 × 2.8 cm. It is equipped with a 12 cm screen with 1024 × 600 pixel resolution and a touchscreen function. The computer is contained in a leather bag, which enables it to be carried easily. The total weight of the device is about 1 kg (Figure 2). The system architecture is shown in Figure 3. Audio and video information is sent to the computer, combined by a messenger program (Windows Live Messenger, MSN, USA) and transmitted to the Internet via WIBRO. The doctor can obtain this information using the messenger program on any PC connected to the Internet. Furthermore, the EMT and doctor can communicate in real-time.
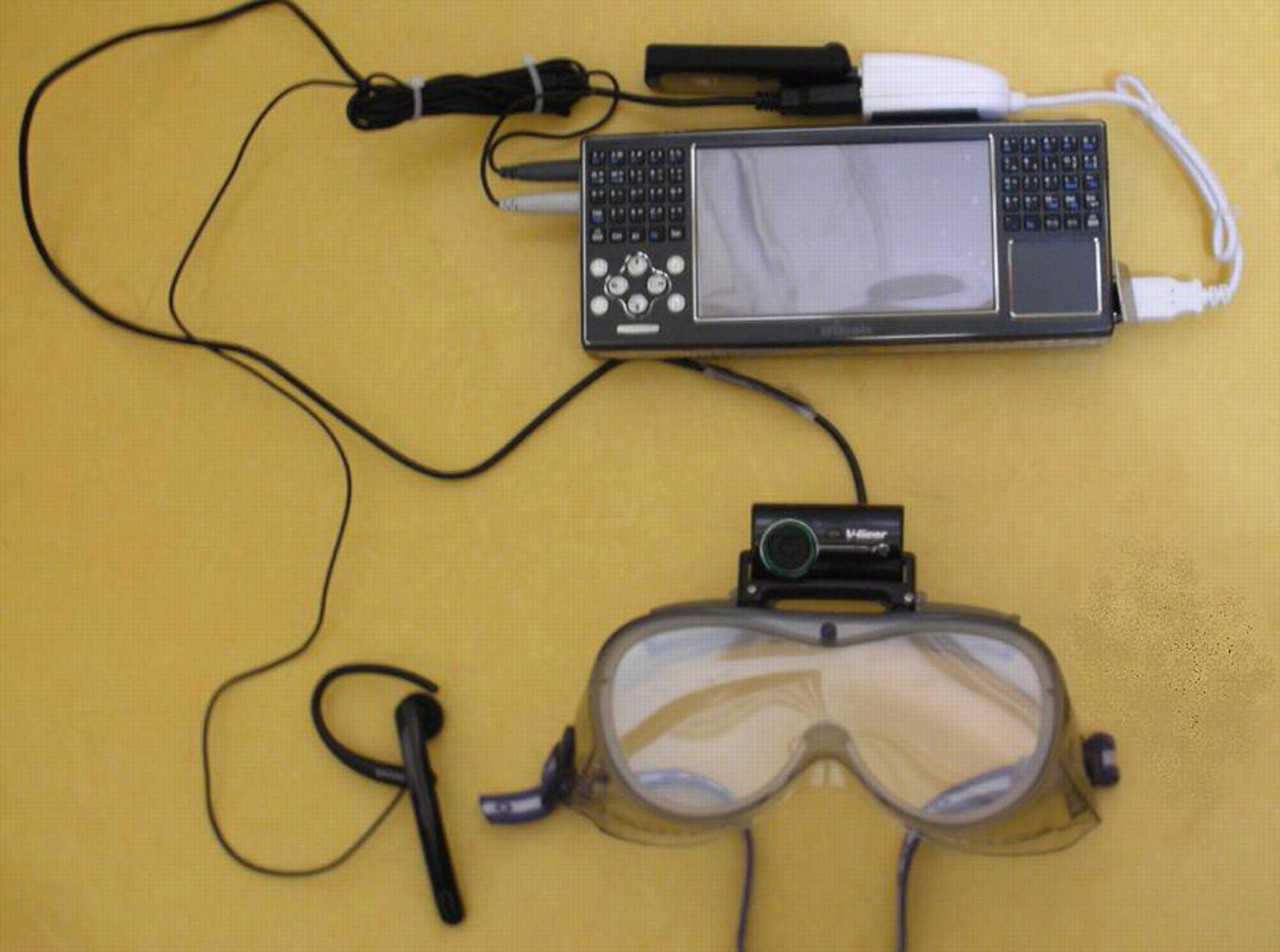
Wireless real-time audio-video transmission device

EMT wearing the device
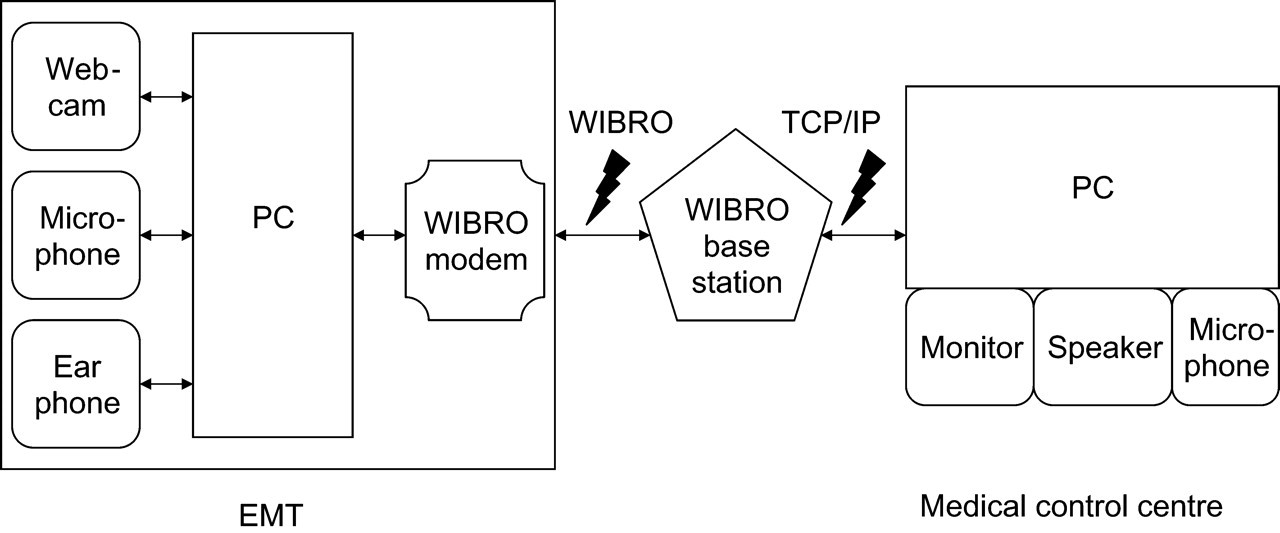
The functional transmission system
To evaluate the performance of the network and the device, we first performed a ping test to measure round-trip time in milliseconds for a data packet to travel from the device to the doctor's PC and back again. We also measured the time delay during transmission of audio/video information and the maximum frame rate. The test was conducted out of doors, inside a building and in a moving vehicle. We also tested five devices over a three-month period at five Rescue Centres in Seoul. Three EMT-1s at each centre were instructed how to operate the device during a one-hour lecture and a one-hour practice session. They then used the device for trauma patient treatment only during the three-month trial period. Ethics committee permission was not required, but verbal consent was obtained from the patient in all cases. Five board certified emergency doctors and three pre-trained EMT-1s participated in the exercise as staff members at the medical control centre. The medical control centre was located at the Emergency Department at Seoul National University Hospital, a Regional Emergency Centre in Seoul metropolitan area. Medical control was available 24 hours per day and 7 days a week.
During the exercise, information was recorded by staff members at the medical control centre each time the device was used. Staff at the medical control centre recorded transmission clarity and assessed the contribution made to medical control using a ten-point scale and counted the number of breaks during transmission. After the three-month exercise, EMTs and medical control centre staff were asked to complete a questionnaire. For each of the questions, the respondent was asked to choose a number between 1 and 9, where 1–3 indicated ‘disagree’, 4–6 ‘neutral’ and 7–9 ‘agree’.
Results
The results of the performance assessment are summarised in Table 2. The device performed best outdoors and functioned well on a moving vehicle. During the three-month exercise, the device was used in 55 cases (see Table 3). The overall success rate was 84%. In most cases, transmissions were made out of doors (Figure 4). Transmission failure occurred randomly in all locations (Figure 5). Two of the eight transmission failures (25%) were due to technical faults (see Figure 6). The unit was most frequently used for patient evaluation (46%) (Figure 7).
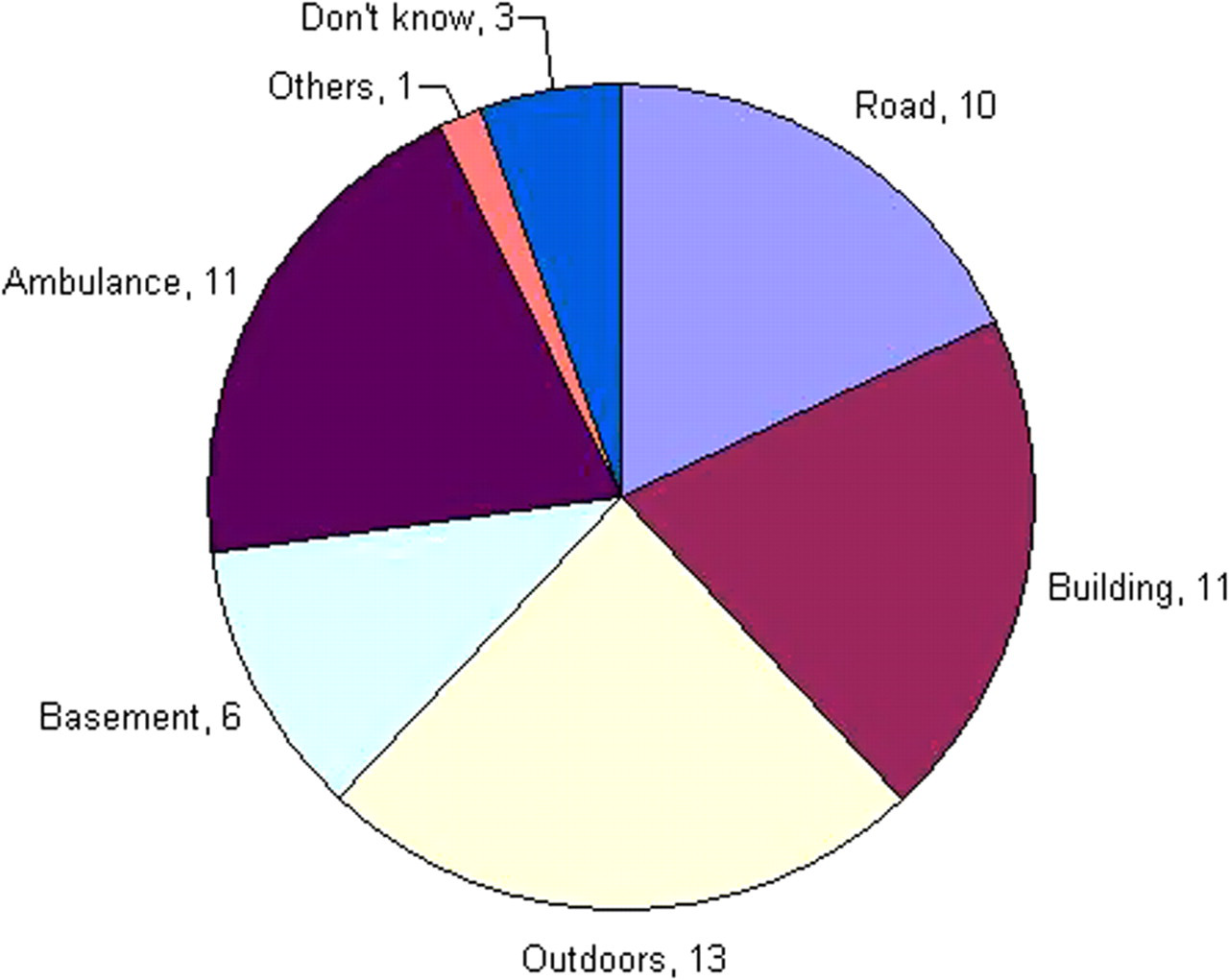
Locations where the device was used (n = 55)
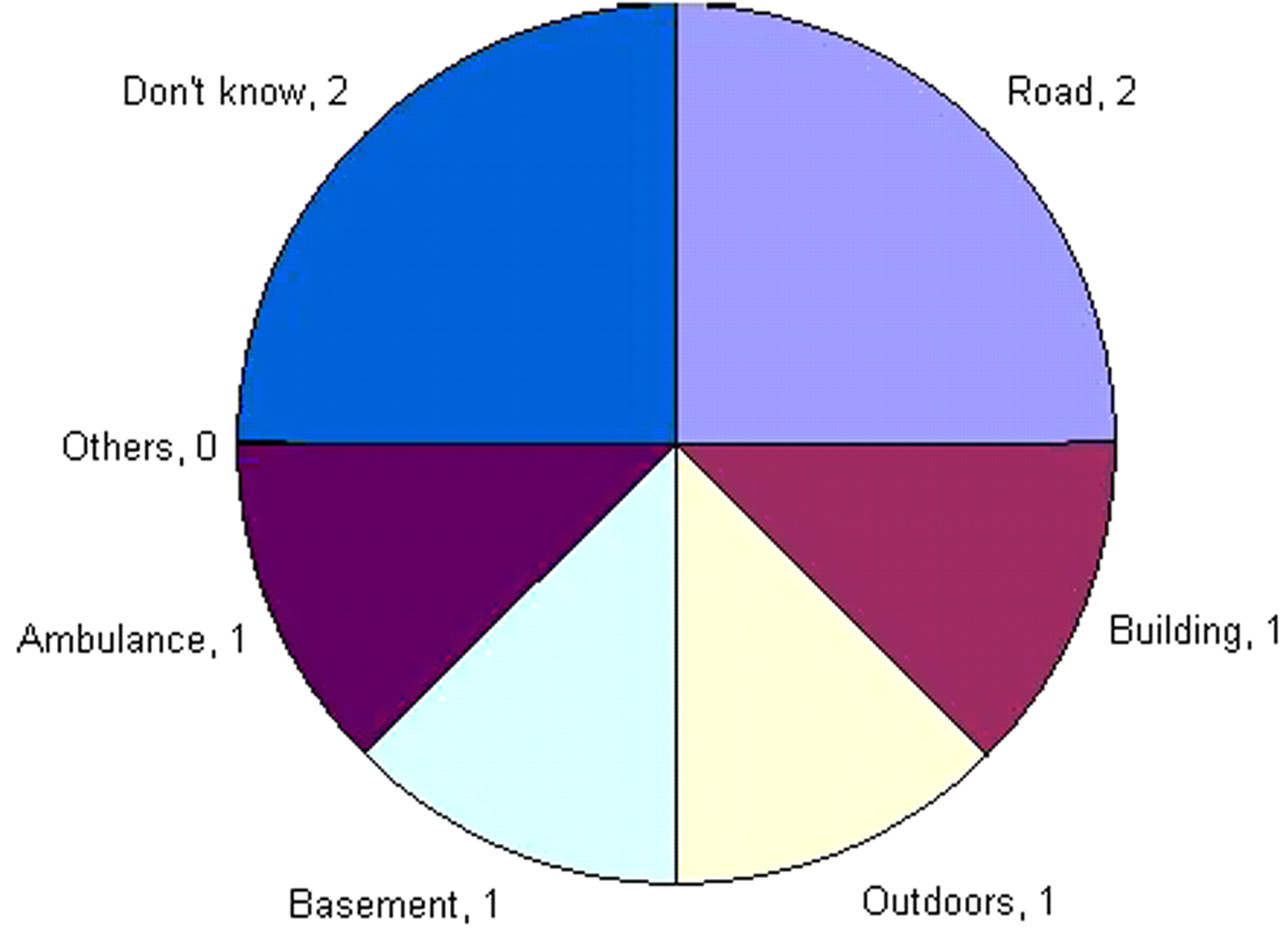
Locations where transmission failure occurred (n = 8)

Causes of transmission failure (n = 8). The category ‘others’ represents unidentified causes
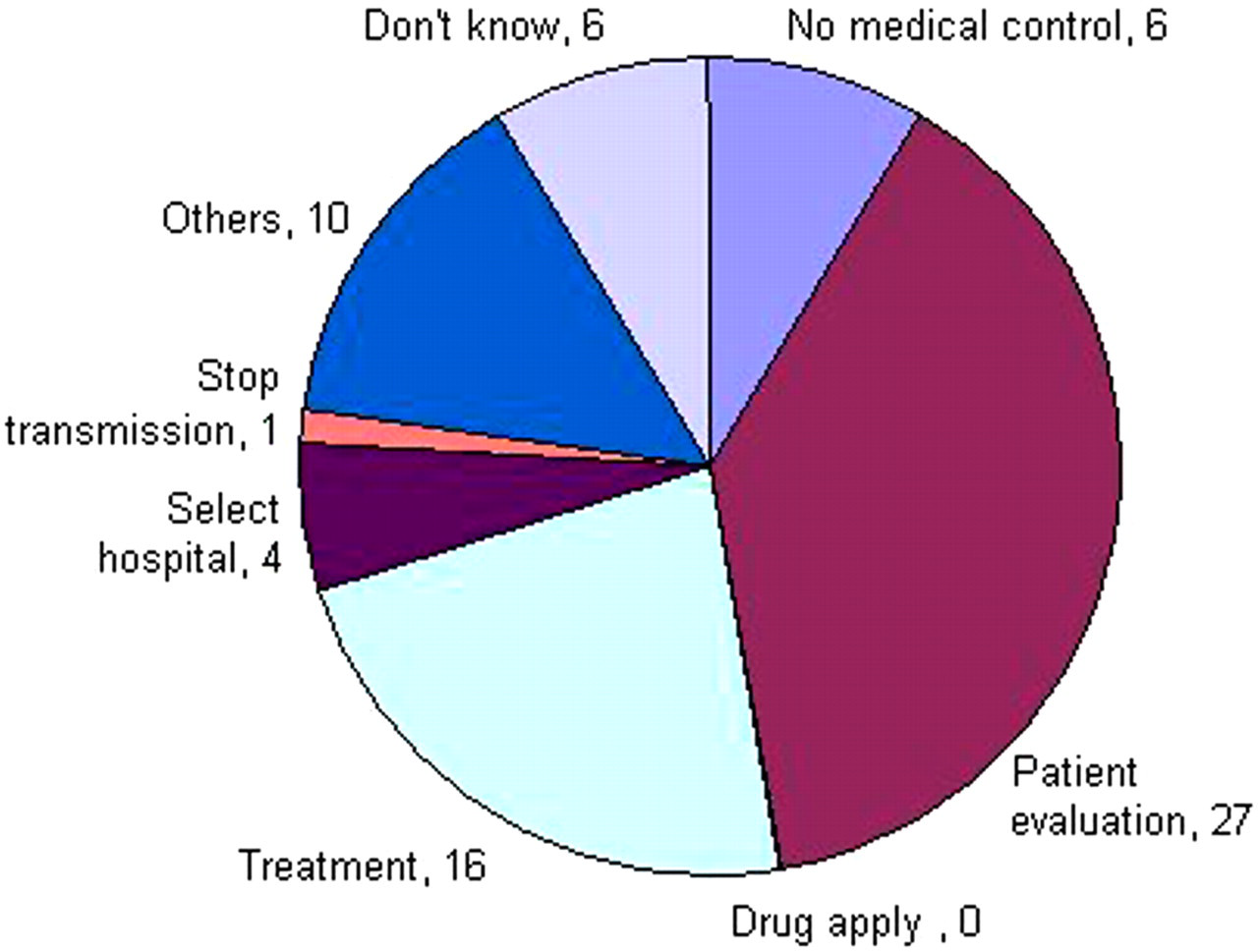
Types of performed medical control (n = 70)
Results of performance tests
Results in real emergency cases, based on the questionnaire responses
*i.e. two-way transmission was achieved, despite some breaks during transmission
Eight control centre staff (3 EMT-1s and 5 emergency doctors) and 11 EMTs who used the device completed the questionnaire. Table 4 shows the responses given by the 11 EMTs and Table 5 shows those of the centre staff. The answers were grouped into three categories of ‘Agree’, ‘Neutral’ and ‘Disagree’ so that the degree of unanimity can be better represented. Both EMTs and centre staff agreed on the helpfulness of the device for trauma patient diagnosis (question 6) but disagreed on the stability and reliability of the device (questions 3 and 4). They split on the ease of use of the device (questions 1 and 2). They were also asked to score ‘This device must be adopted for use by Pre-hospital Emergency Medical Services’, and showed lower or neutral agreement level (4.5).
EMT questionnaire results
Medical control centre staff questionnaire results
Discussion
Our results demonstrate that the transmission of medical information is feasible, even from a vehicle moving at 70 km/h. The quality of audio and video transmission, based on the records of the medical control centre staff, was judged to be intermediate, and the average number of breaks during transmission was not considered to be a problem. However, the questionnaire results showed that although EMTs and medical staff thought that the device was useful at emergency scenes, they found it inconvenient to use. One problem encountered was that sudden head movements by the EMT made visualization impossible for the doctor, even when overall transmission quality was good. Another problem was that repair and maintenance were difficult. The present study demonstrates the need to develop a customized device for emergency medical control that has greater stability and is more convenient. To produce the experimental unit, we integrated hardware and software designed for general purpose use. Our experience suggests that a custom-made unit is required for emergency medical purposes. Furthermore, if portable health monitoring instruments were included, medical control could be enhanced by including ECG or other health status information.
Nevertheless, all users agreed that a suitable unit could enhance EMT utility and the level of performance of pre-hospital emergency care, and we believe that the concept of information transmission is appropriate. In one particular case, the unit proved highly effective. This case involved a 33-year-old man who had fallen down a hole, and had suffered a penetrating injury of the thigh caused by an iron bar protruding from the ground. The patient was trapped, caught by the fixed iron bar. The EMT at the scene asked the doctor at the medical centre for advice about treatment prior to removing the patient from the hole for transfer to hospital. The remote doctor ordered that the bar not be removed, but rather that it be cut several centimetres from wound and protected with a blanket. This was done, and the patient was transported to the Regional Emergency Centre, where he received appropriate treatment from the waiting doctors.
We believe that future improvements to the device, in terms of its performance and usability, will contribute to direct medical control during the pre-hospital stage and to the establishment of a higher quality pre-hospital emergency medical service.
Footnotes
Acknowledgements
This research work was supported by the Nano/Bio Science & Technology Program (2008–00863) of the Ministry of Education, Science and Technology (MEST), Republic of Korea.