
Abstract
We evaluated the feasibility and quality of uncomplicated hypertension care based on telemedicine in a rural area of northern Sweden. The intervention subjects were 91 consecutive patients with primary hypertension. For comparison, 182 age- and sex-matched patients with hypertension were randomly selected from a similar health centre. The telemedicine equipment consisted of a video link between the physician and the patients, supported by a system for accessing medical data via the Internet. During a 21-month study period, telemedicine was used in 270 (91%) of the 297 consultations in the intervention group. All health personnel involved in the telemedicine treatment rated the method as feasible. Both systolic and diastolic blood pressure improved in the two groups during the study period. In the intervention group, a higher proportion had their blood pressure within treatment goals (systolic blood pressure <140 mmHg, diastolic blood pressure <90 mmHg) both at baseline and at follow-up than in the comparison group. An adjusted multivariate model (adjustment for sex, age, time between visits, change in number of drugs between first and last visit, blood pressure at first visit) showed that the intervention group had a higher probability (OR 2.7, 95% CI 1.4–5.2) of reaching the target blood pressure levels than the reference group. Treatment of hypertension by means of telemedicine was quite feasible and at least as effective as face-to-face consultations with a physician.
Introduction
The favourable effect of the availability and continuity of general practitioners (GPs) in primary health care was recently reported in a systematic review, 1 although there is at least one study from the UK that failed to find such a positive association. 2 The importance of access to primary care on public health outcome measures, especially in low-income districts 3 and in rural areas, has been previously reported. 4 However, providing good quality health care is a challenge, especially in rural areas. In the western hemisphere, demographic changes with an ageing population with increasing life expectancy puts pressure on resource allocation. This has motivated the development of new diagnostic methods and equipment that will reduce the need for transportation of patients and specialists.
At the Lövånger health-care centre, which is situated along the coast in the midpart of the County of Västerbotten, many of the patients with chronic diseases were not attended to as would have been expected. Patients with hypertension were identified as one large group who had suffered from understaffing of GPs. Patients with hypertension have a high risk of morbidity and mortality in cardiovascular disease (CVD). 5 Therefore, attaining treatment goals for hypertensive patients is a high-priority task for primary health care.
The aim of the present study was to evaluate the feasibility and quality of uncomplicated hypertension care in rural areas (treatment in practice). A nurse-led surgery with doctor support by telemedicine was compared to a surgery with face-to-face consultations between physicians and patients.
Methods
The subjects studied were 91 consecutive patients (intervention group) with primary hypertension visiting the Lövånger health-care centre (from March 2005 until November 2006) with both known (n = 85) and newly discovered hypertension (n = 6). There were 49 women (54%, median age 64 years) and 42 men (median age 68 years). The intervention group was chosen to reflect the ordinary patient population, with the variation this might show in hypertension level and treatment status. Ethics permission was not required. In this kind of evaluation study it is important to have as much variation as possible among the patients. This is contrary to a randomized control study where the variation should be held at a minimum. 6
Study design
The two surgeries shared identical treatment protocols for hypertension, had catchment areas with a patient coverage of 95% of all hypertensive patients and they belonged to the same local management of the County Council. Consecutive uncomplicated hypertensive patients scheduled for prescription renewals or newly detected cases were included. Patients with kidney diseases and diabetes (who often have high co-morbidity) were excluded to reflect ‘everyday practice’ in primary care. The intervention group was monitored for their hypertension with the help of a local district nurse and a physician participating via videoconference. There were standard procedures for diagnosis of hypertension, i.e. systolic and diastolic blood pressure >140/>90 mmHg, according to the WHO and the International Society of Hypertension. 7,8 The visit was documented in a structured way, with consideration of test results, e.g. blood pressure, ECG, blood lipids, creatinine and potassium.
In this study the first (baseline) and the last visit (follow-up) during the twelve-month period were analysed for the intervention group. The rationale was to eliminate the influence of short-term changes caused by alternations in treatment regime. Another reason was that there is often 12 months between two visits if the patients have a well-adjusted blood pressure. Most of the intervention patients (80%) had between one and three visits during the period (baseline excluded). The idea was that the patient's hypertension should be well prepared towards their target pressure.
From the original 91 patients, three questions on the patient experience were put to the 39 patients participating directly in the videoconference (see Figure 1) with the physician: ‘What is your opinion of the contact with the physician using telemedicine compared to meeting the physician in real life?’, ‘Do you understand the treatment of your hypertension?’ and ‘In your opinion, have you received enough information about your hypertension disease?’ The responses were on a five-point scale. These three questions were judged to be the most central for evaluating the patient's opinion on meeting the doctor with the help of a videoconference.
Flowchart for patients in the intervention group
Reference group
To compare the patients being monitored with telemedicine, 182 age- and sex-matched patients with hypertension were randomly selected from patient records during the same period from an adequately staffed health centre with the same hypertension treatment programme as Lövånger. The reason for choosing two reference patients per case, matched for age and sex, was to have variation among patients in order to perform statistical process control 9 analysis, as well as to increase the power of the study. The comparator patients did not have diabetes.
Staff responsibilities
At the Lövånger health centre it is the nurses who manage the patients with hypertension. During the consultations, the patients' risk profile was assessed by asking questions about cardiovascular disease heredity, co-morbidity, smoking and lifestyle.
At the health-care centre the nurse prepared the telemedicine session by measuring the patient's blood pressure and recording the ECG, and taking blood samples. The patients were monitored with the help of guidelines for hypertension. In order to acquire the history, the nurse followed a questionnaire specially designed for hypertension patients. From this document a first summary was made about the patient in order to evaluate risk factors. Because of the preparatory work conducted by the nurse the telemedicine consultation with the physician could be limited to 15–20 minutes. The visit was documented in a structured way, with consideration of the test results. After risk estimation, the physician set the target for the blood pressure and prescribed the treatment. 7,8
Monitoring hypertension
Blood pressure was measured with the patient in a sitting position after five minutes rest. In 2001, a computerised decision support system (DSS) was introduced, and during 2004 this system was introduced as an Internet application. 7,8 Monitoring the hypertension patients followed a standard treatment programme. The programme followed the principles of the World Health Organization (WHO) and the International Society of Hypertension 10 and the 2007 recommendations from the Swedish Council on Technology Assessment in Health Care. During the teleconsultations, patients were present in the studio when there was need for examination of the heart, medication questions, and guidance and treatment discussions. All contacts between physician and nurse utilised the videoconference system and the computer-based medical chart system. The nurse was also present during all the patients' physician contacts.
Equipment
The telemedicine equipment consisted of a video link between the physician and the patients, supported by a system for communication over the Internet. 11 Both the treating physician and the nurse at the primary health-care centre had simultaneous access to the County Council's computerised medical chart.
The patient and nurse used a videoconference system (880 NPP, Tandberg), with a control centre designed for offices and a 81-cm monitor. The unit operated both as a videoconferencing system and PC display, enabling real-time, face-to-face collaboration at the desktop. The physician used a laptop, (T42, IBM), with a webcam. The camera had a resolution of 1.3 Megapixels (still images). Videoconferencing was usually conducted at a rate of 768 kbit/s. Software developed by the County Council's Department of Research and Development enabled access to the medical data.
Experience of using telemedicine
In order to evaluate the experience among those who were the subjects of the telemedicine intervention, the patients, nurse and doctor were asked about their attitude. At the study site the nurse and the physician were asked to complete a memo book after each session. This is a method used in qualitative research design. 12 For the patients, a questionnaire with three questions were distributed.
Statistics
Univariate and multivariate logistic regression was used for analysing differences between the intervention centre and the control centre in improving the proportion of subjects who reached the treatment goal (systolic blood pressure [SBP] <140 and diastolic blood pressure [DBP] <90 mmHg) at follow-up. Statistical process control was utilized to analyse the change in blood pressure over time. The data analysis was conducted using standard software packages (SAS, SAS Institute Inc., Cary, NC; SPSS ver. 15.0, SPSS Inc., Chicago, IL; Statistica ver. 8, StatSoft, Inc).
Results
Telemedicine utilisation
Telemedicine was used in 270 (91%) of the 297 consultations in the intervention group. The mean number of visits was 3.3 per patient. The main reason for not using teleconsultation was malfunction of equipment. During the consultations sound and picture were considered to be good to excellent in 90% of the transmissions. This was judged by the physician and the nurse separately.
Patients
Among the 91 patients in the intervention group, there were 39 (17 women and 22 men) who had direct contact with their GP via videoconferencing. The rest were monitored by the nurse, who contacted the physician by telemedicine when required. There were no significant differences between men and women in their opinion of the experience of monitoring their hypertension with the help of telemedicine (Table 1). The majority rated the consultation via telemedicine as least as good as meeting the GP in person.
Patients' opinions about using telemedicine (17 women, 22 men)
The nurse
The nurse found it easy to work according to the structured template. There was no redundancy in the information retrieved. The consultation with the help of videoconferencing was a good way of estimating the patient's situation, both the nurse and the physician could read the electronic chart and the test results were immediately accessible. With the patient present, telemedicine gave the opportunity for a comprehensive evaluation of the patient. For instance when using the remote stethoscope, the physician was able to listen to the patient's heart and see the person.
After working for more than a year with telemedicine, the nurse felt that it was a better way of working. It relieved the physician of routine tasks and improved the nurse's options of working more independently.
The physician
Working with videoconferencing was found to be an advantage, both in physician–patient and physician–nurse co-operation. The equipment was fairly easy to use. The remote stethoscope worked well after a learning period. It was useful for remote examination of heart rhythm and murmur. It was not useful for lung examination.
The mobility of the laptop reduced the need for specially assigned premises for the physician. It was easy to move the equipment between health centres, especially during summer when some of the places were closed due to holidays. Under ideal conditions, it took approximately 15 minutes to get the equipment running.
In the consulting phase a lot of information was non-verbal. Seeing the patient and the nurse during the consultation gave more information, with more nuances than viewing the test results and a telephone consultation. The visual link and the dialogue made it easy to modify treatment according to the actual patient and the circumstances.
Hypertension monitoring
There was a longer period between baseline and follow-up, and a higher SBP and DBP in the patients of the reference group than those in the intervention group (Table 2). Both SBP and DBP improved in the two groups during the study period. In the intervention group, a higher proportion had their blood pressure within treatment goals (SBP <140 mmHg, DBP <90 mmHg) both at baseline and at follow-up than in the comparison group. There was no significant difference in the reduction of blood pressure between the two groups (Table 2).
Baseline characteristics and differences in blood pressure at baseline and at follow-up in the intervention and reference groups. Values shown are median (interquartile range)
Time dependency
The difference in systolic and diastolic blood pressure for intervention and reference patients, between baseline and follow-up, is shown in Figures 2 and 3. There was no interaction between time, status as an intervention/reference subjects and changes in SBP or DBP (data not shown).
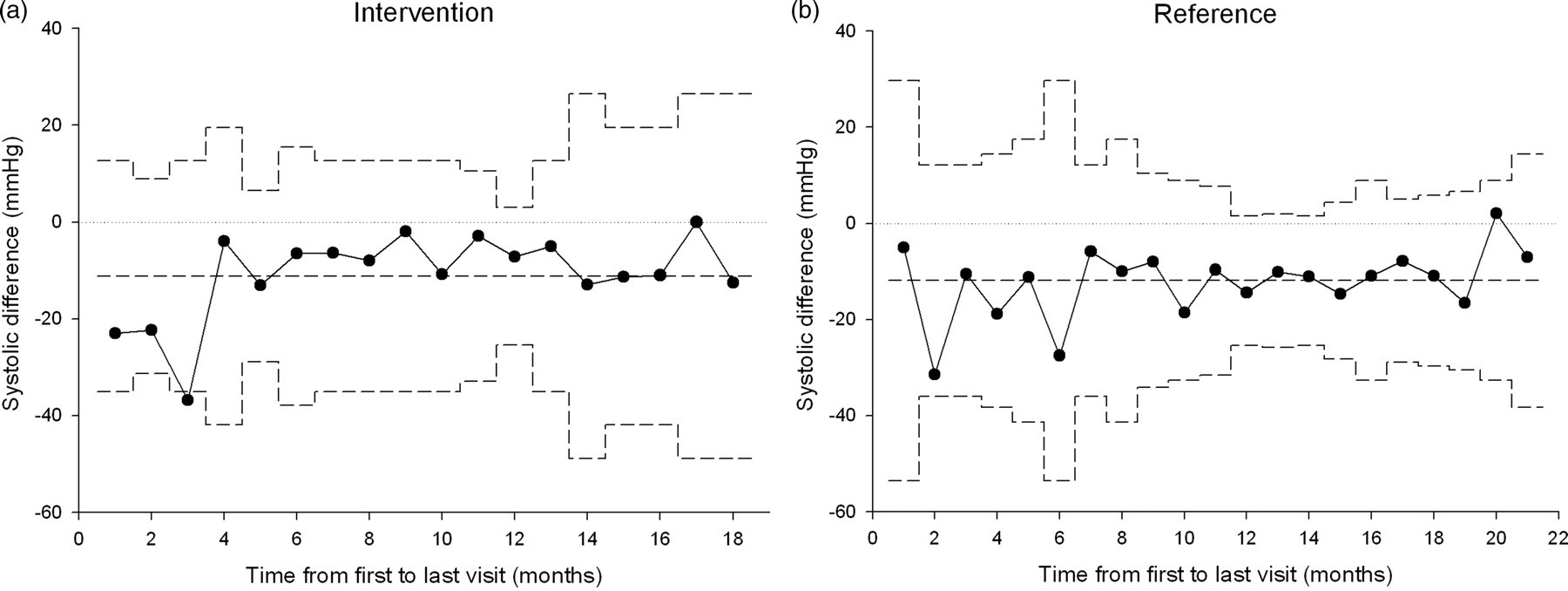
Change in systolic blood pressure related to time between baseline and follow-up. The broken lines show the mean values and 95% confidence limits (a) Intervention group (b) Reference group

Change in diastolic blood pressure related to time between baseline and follow-up. The broken lines show the mean values and 95% confidence limits (a) Intervention group (b) Reference group
Antihypertensive drugs
The number of hypertension-lowering drugs varied between the baseline and follow-up (Figure 4). There was a significant increase in the number of prescribed antihypertensive drugs between the two occasions among both in the intervention and reference groups (P < 0.001). However, the number of drugs did not differ between the two groups. In the intervention group 16 had their medication changed, 18 adjusted their dose and eight had their prescriptions renewed at baseline.

The distribution of prescribed number of hypertension lowering drugs, among intervention and reference groups (a) At baseline (b) At follow-up
Treatment
The distribution of drugs for intervention and reference groups at baseline and follow-up is summarised in Table 3. Among the intervention group ACE-inhibitors more than doubled, while the use of beta-blockers was reduced. However, beta-blockers were still the most commonly prescribed antihypertensive agent. A similar pattern was seen among the reference patients.
Percentage prescribed hypertension drugs among intervention and reference group. The percentage is calculated from all prescriptions (n = number of prescriptions)
Factors affecting the outcome
The improvement rate, i.e. the percentage who converted from being above treatment goals to reaching the goals, was higher in the intervention group (35% at start to 74% at follow-up, a change of 38%) than in the reference group (21% at start to 46% at follow-up, a change of 24%, P = 0.046 for this percentage difference between groups). In order to further evaluate what influenced the improvement rate a logistic regression was performed. The intervention group had a higher chance of improving blood pressure control (OR 1.9, 95% CI 1.1–3.2, P = 0.016) compared to the control group analysed in a univariate model. This was confirmed in an adjusted model (adjustment for sex, age, time between visits, change in number of drugs between first and last visit, SBP and DBP at first visit) where the intervention group had a higher probability (OR 2.7, 95% CI 1.4–5.2) of improving their blood pressure using the control population as a reference.
Discussion
We found that both patients and staff rated the treatment of hypertension via telemedicine equipment as feasible. The patients treated via telemedicine had a higher probability of improving their blood pressure, i.e. converting from non-reaching to reaching the treatment goals compared to control patients.
We used the health-care provider's own description in evaluating their experience of the way of working with telemedicine, with the help of their memo book. We used a patient questionnaire which was not validated. However, it contained questions relevant from our experience. We also assessed the effect of the intervention by the change to an accepted level of blood pressure control. This was a slightly different approach compared to some of the large hypertension studies, 13 but it has been shown that reaching the treatment goal is essential for reducing cardiovascular disease. 11
There were some weaknesses in our study that should be mentioned. First, our questionnaire to patients was not validated and did not include any open questions. Second, we were not able to control for all co-morbidity, even though matching for age and sex may have reduced any difference between cases and controls. Third, there were differences in blood pressure at baseline, with the reference population having higher blood pressures. We corrected for the difference in our multivariate model. Fourth, a prospective design for the reference group would have made our comparison much stronger. The strength of our study was a large study population with an appropriate reference group. Thus, we were able to control for differences in baseline blood pressure and time to second blood pressure reading.
Despite these flaws, our overall conclusion was that telemedicine was feasible in the treatment of hypertension. The technique was not a major obstacle to the consultation and it facilitated the decisions made by the treating physician. This is important as acceptance by both patients and caregivers is vital for the successful implementation of a new technique. In a recent systematic review of the clinical effectiveness of interventions using information and communication technologies, only three studies (of older date) in hypertension were identified, 14 where telephone transmission of home measured blood pressure was the mode of technology. Thus, none of these studies were similar to our study. Jerant et al. 15 showed that using telemedicine reduced hospital readmissions, emergency visits and costs. The technique was well accepted by both patients and caregivers. Thus, our study appears to be unique in employing a real-time technique to facilitate both patient–nurse–physician communication and diagnostic ability in the treatment of hypertension.
It was also important to show that using the new technique was at least as effective as standard counselling in improving blood pressure. We noted that the treatment of hypertension improved in both health-care centres and most patients reached the treatment goals in both groups. This is in contrast to numerous studies which have demonstrated the difficulty of attaining treatment goals in hypertensive patients. 16,17 The unexpectedly high proportion of controlled hypertension in our study could be due to the mild to moderate primary hypertension that the patients had at baseline. Based on our clinical experience of ‘white coat’ hypertension the procedure of the nurse measuring the blood pressure may have been beneficial in the intervention group. The number of antihypertensive drugs increased in both health-care centres with a decrease in the use of beta-blockers and an increase in ACE-inhibitors, often in combination with thiazide diuretics. However, in contrast to present recommendations, 18 beta-blockers were still the most commonly prescribed antihypertensive drug.
Conclusions
We have shown that treatment of hypertension by means of telemedicine is at least as effective as face-to-face consultations with a physician. The technique was well accepted by patients and caregivers. Whether this technique is effective on a large scale, in a different setting with a high risk population, on a long-term basis, and if it can be cost-effective for society or for patients, now needs to be evaluated.
Footnotes
Acknowledgements
The study was financially supported by the Västerbotten County Council. We also acknowledge the help and support given by Mr Per-Olof Söderström at the Västerbotten County Council for initiating the study.