
Abstract
Only 42 of the 116 public hospitals in Queensland employ qualified pharmacists to staff their pharmacies. We undertook a feasibility study to determine if pharmaceutical reviews, undertaken face-to-face by a visiting pharmacist, could be replicated using telemedicine. The study was conducted in two phases, with the same pharmacist coordinating the project from the main hospital to two rural hospitals, which relied on supply nurses for all their pharmaceutical services. All inpatients admitted between October 2006 and May 2007 were included in the study. In Phase I the pharmacist made weekly visits to both facilities, to perform face-to-face pharmaceutical reviews of the current inpatients. In Phase 2, all pharmaceutical reviews were performed remotely by the pharmacist by telephone or videoconference. In Phase 1, 186 pharmaceutical activities were performed (mean 3.9 per patient). Of these, 78 pharmacist-initiated changes were recommended and 47 (60%) were implemented. In Phase 2, a total of 296 activities were performed (mean 3.1 per patient) and of the 140 recommendations made by the remote pharmacist, 74 (53%) were accepted. Of the accepted recommendations, there were 11 major interventions (those with a potential to prevent harm to the patient) in Phase 1 and 32 in Phase 2. There were no significant differences in the pharmaceutical activity rates in the two phases. Telepharmacy therefore may be an effective method of providing pharmaceutical reviews for patients in rural inpatient facilities, without an on-site pharmacist.
Introduction
In 2004, the Australian Health Ministers recommended that every Australian hospital should have a process for reviewing medication prescribing and dispensing, and for documenting the use of medicines. Pharmacists are trained to provide such reviews in order to achieve the best possible outcomes for the patient. However, only 42 of the 116 public hospitals in Queensland have pharmacies staffed with qualified pharmacists. The remaining hospitals rely on supply nurses for their pharmaceutical needs. Recruitment and retention of rural and remote hospital pharmacists has been difficult, with the number of pharmacists falling from 80 per 100,000 population in 2000 to 73 per 100,000 in 2005. 1 New ways of providing services must therefore be considered.
Previous studies into telepharmacy have focused on its potential applications for remote dispensing and patient counselling in outpatient clinic settings. 2–4 These studies were generally successful in improving access to medications in rural areas and improving medication education and adherence.
Few telepharmacy studies have investigated the impact of remote pharmacist involvement on improving patient safety and reducing medication misadventure. Nissen et al. investigated the use of telepharmacy in improving the quality of pharmaceutical services in rural and remote areas. However, the study was limited by technical failures. 5 Bynum et al. investigated the use of telepharmacy on improving inhaler techniques among young asthma sufferers and found that telepharmacy was superior to providing education by written instruction alone. 6
The present feasibility study was designed to investigate the use of telemedicine to expand the service capability of a rural pharmacy. The aim was to determine if a remote telepharmacy review process could achieve similar results (i.e. patient outcomes) to reviews undertaken in person by a pharmacist, and to determine if telepharmacy could improve medication management in rural settings.
Methods
The study was conducted in two phases, with the same pharmacist coordinating the project from the main hospital (Toowoomba) to two rural hospitals (Laidley and Gatton), which relied on supply nurses for all their pharmaceutical services. All inpatients, both public and private, who had been admitted for longer than 24 hours and for whom a completed medication chart was available, were included. Ethics approval was not required for the study.
Phase 1
A pharmaceutical review of the current inpatients (total 48) was undertaken, in person, by the pharmacist, at the two rural sites, once a week, during an eight-week audit period (Oct–Dec 2006). A pharmaceutical review was defined according to the standards of the Society of Hospital Pharmacists, and involved the assessment of the patient for the purpose of evaluating the response to medicine therapy and detecting and managing potential or actual clinical problems in liaison with the patient, medical and nursing staff. 7
All pharmaceutical activities performed by the pharmacist were documented. An activity was defined as any task performed by the pharmacist in the course of their daily duty to constitute a clinical pharmacy service to hospital inpatients. Data were collected on numbers of, and problems associated with, medication histories, medication charts and discharge medication records (DMRs) using standard data collection forms designed by the Safe Medication Practice Unit (SMPU) in Brisbane.
The pharmacist's recommendations were conveyed via the use of a Medication Action Plan (MAP) form, produced by the SMPU. Verbal communication was used if immediate action was required. All patients requiring intervention were identified to the medical and nursing staff.
At the end of Phase 1, registered nurses at both sites completed training modules in medication history-taking and discharge medication record production. Both modules were produced and taught by the SMPU.
Phase 2
Phase 2 was initially conducted over a 16-week period (Jan–May 2007). All inpatients were reviewed remotely by the pharmacist (total 97 patients).
Daily inpatient handovers were performed between the remote pharmacist and an on-site nurse. These handovers were performed by telephone or videoconference. The videoconferencing systems (MX990, Tandberg) were connected at a bandwidth of 256 kbit/s. Handovers included an update on each inpatient; current status, presenting complaint (if newly admitted), observations, test results and any plans for discharge (see Table 1). The nurse was responsible for faxing/scanning the patients' medications charts (if new) and the medication history (MAP form) where applicable. The remote pharmacist had access to pathology results and the enterprise-wide liaison medication system (eLMS), which enabled DMRs to be reconciled remotely.
Processes in the two types of pharmaceutical review

Videoconferences with the remote pharmacist were arranged for patients, selected by the nursing staff as appropriate candidates. These consultations offered an opportunity to provide medication counselling and obtain clarification on medication histories. During Phase 1 patients were able to freely consult with the pharmacist during their weekly on-site visit.
Audits of medication charts, medication histories and DMRs were repeated by the pharmacist, using the same data collection forms as in Phase 1.
Data analysis
Data on all pharmaceutical activities were analysed. The scheme used to categorise these activities into drug-related problems, was adapted from several different studies. 8–10 Activities were categorised into one of six categories: (1) drug choice; (2) dosage; (3) interactions; (4) monitoring; (5) counselling; and (6) other activities.
Interventions were defined as any action by the pharmacist that directly resulted in a change in patient management or therapy. 7 Interventions defined as being of major significance had the potential to cause harm to the patient if direct action was not taken. This approach has been used before. 11
NCSS, a statistical software program, was used to produce descriptive statistics to report the demographic and pharmaceutical activity data for the study population. Differences in patient characteristics and numbers of activities were analysed using either an unpaired t-test or Mann-Whitney U statistic. Categorical data were analysed using the chi-squared test.
Results
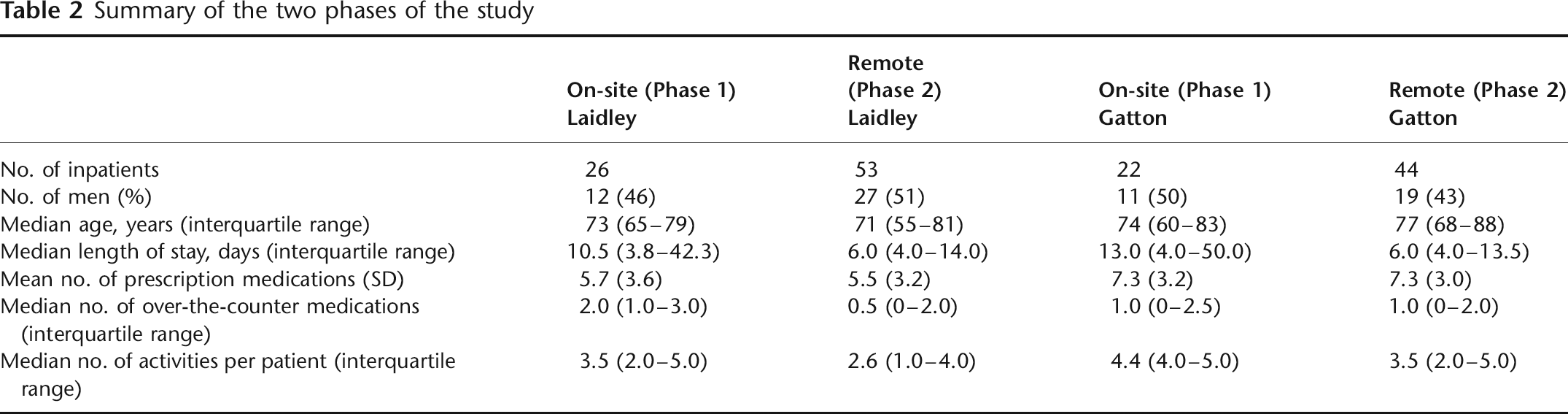
Information was collected on 48 patients in Phase 1 and 97 patients in Phase 2. There were no significant differences between age, sex and mean number of medications taken on admission, between the two phases. The baseline characteristics of the patients are shown in Table 2.
Summary of the two phases of the study
There were daily telephone consultations with staff at Gatton and Laidley, and twice weekly videoconferences with staff at Laidley. A total of 14 videoconference consultations were conducted with patients at the two sites.
Pharmaceutical activities
In phase 1, 186 pharmaceutical activities were performed (mean 3.9 per patient). As a result of these, 78 interventions were made by the pharmacist and 47 (60%) were implemented. In Phase 2, a total of 296 activities were performed (mean 3.1 per patient) and of the 140 interventions suggested by the remote pharmacist, 74 (53%) were accepted by the clinician and subsequently changes were made to the patients' medication regimen.
The frequency of the various activities performed and examples of each are shown in Table 3. The most frequently performed clinical activities were documenting a medication history and identifying a medication omission. No significant differences in the overall rate of occurrences of activities (using the frequency data) were observed between the two phases.
Summary of the activities recorded by the pharmacist
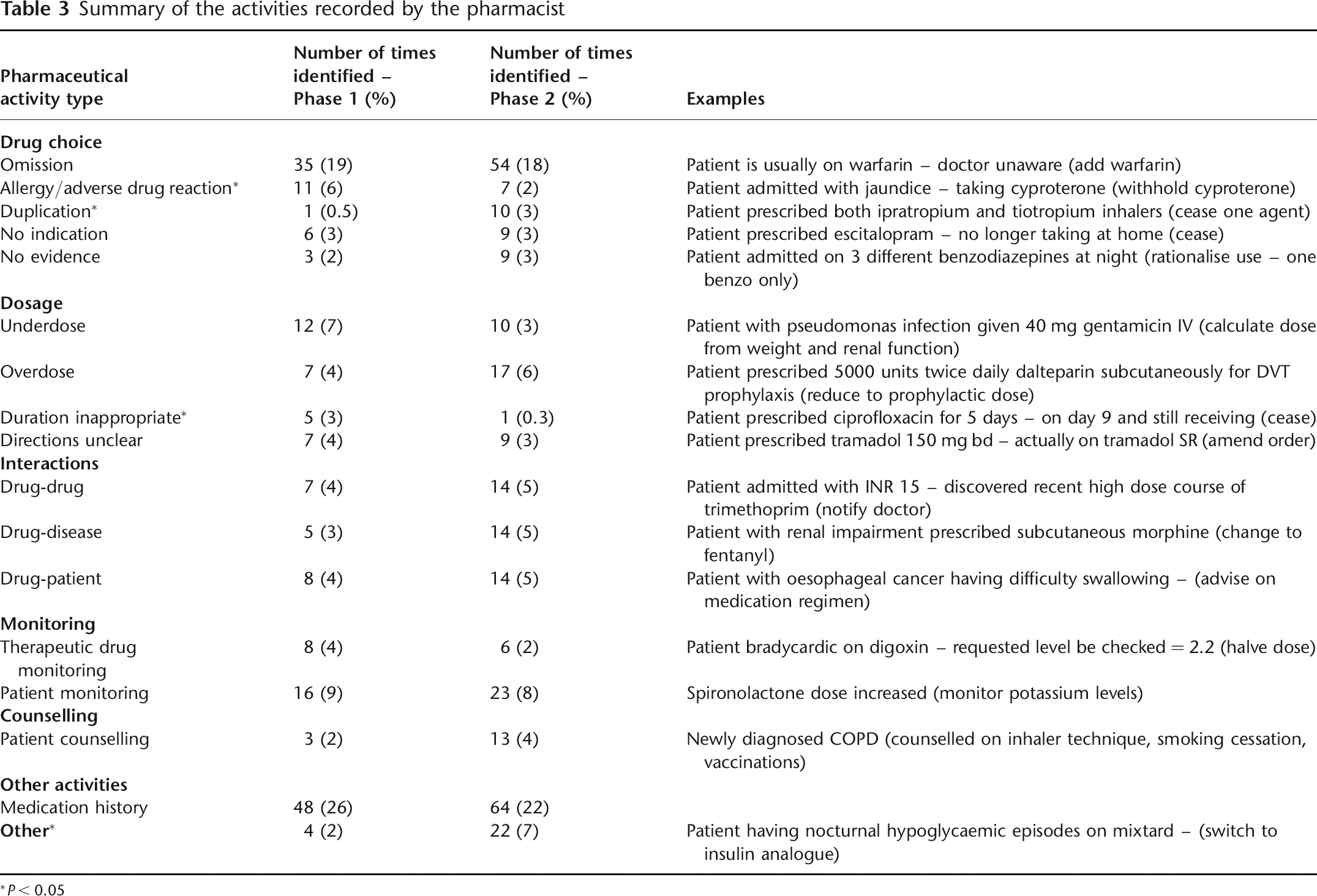
*P < 0.05
All activities were included in the study, irrespective of actual or potential significance. Major interventions accounted for 11 (23%) of the accepted interventions in Phase 1 and 32 (43%) in Phase 2. This difference was significant (χ2 = 4.9, P = 0.03). Overall for every 17 activities performed by the pharmacist in Phase 1, one successful major intervention was achieved. In Phase 2, one in nine activities performed by the pharmacist led to a major intervention. Furthermore, pharmacist interventions were made on approximately 2 out of every 3 patients reviewed in both phases.
Medication history and reconciliation
Documentation of admission medication histories significantly increased in Phase 2 compared with Phase 1. Following the introduction of the MAP form in Phase 2, significant improvements were noted in medication history documentation with the number of medications with missing dose and directions falling to 5% (χ2 = 6.6, P = 0.01).
There were discrepancies between medication histories taken by clinicians and those taken by the remote pharmacist. The percentage of patients with at least one discrepancy in their medication history fell from 61% in Phase 1 to 49% in Phase 2. This reduction was not significant.
Discharge medication record production and reconciliation
During Phase 1, Gatton hospital had no technology for producing DMRs. Seventeen patients (89%) at Laidley received a DMR on discharge. Over half of these were noted to contain errors (medications omitted, added or dose discrepancies) when retrospectively reconciled by the pharmacist. The accuracy of the DMRs improved significantly from 7 (41%) in Phase 1 to 48 (81%) in Phase 2 (χ2 = 10.7, P = 0.001).
Discussion
The results of the present feasibility study demonstrate that telepharmacy can be used successfully to provide remote pharmaceutical reviews for inpatients at rural facilities. Although this service cannot replace the benefits of having an on-site pharmacist, the trends from this pilot show that it may be an effective alternative.
Few significant differences were noted in the proportion or frequency of activities performed in the two phases and similar proportions of activities were documented in each of the six broad categories (drug choice, dosage, interaction, monitoring, counselling and other). Clinical pharmacy activities have been well studied in large, metropolitan hospitals, 12,13 although only limited data are available in smaller, rural facilities. Fiore et al. identified the need for improved support services to supply nurses in rural and remote areas and noted the shortage of pharmacists and geographical isolation to be continuing problems. 14 Fiore et al.'s study fully supports the more active involvement of pharmacists at rural facilities.
One in 17 activities averted major patient harm in Phase 1 compared to one in nine activities in Phase 2. This may have been due to the increased frequency of review (daily versus weekly) and may demonstrate the value of regular, remote pharmacist input, rather than an irregular on-site service. As discussed earlier, many models for improving access to medication in rural areas have focused on supply matters and have often avoided the direct involvement of a pharmacist. Given the potential benefit in reducing medication misadventure, demonstrated by the trends in the present small study, further investigation of the telepharmacy model appears to be worthwhile. The proportion of major interventions made was lower than described in other studies (25% reported by Dooley et al.), 12 but may reflect the less-acute nature of rural hospitals. The proportion of interventions accepted was lower in Phase 2 and lower than described in other studies (84% accepted in a hospice study 15 ). This may have been due to the consultative nature of the recommendations, or the benefit of having direct communication with the prescriber during on-site visits in Phase 1. The uptake of recommendations from the remote pharmacist may have also depended on the rapport developed with the prescriber and perhaps the frequency of contact.
Medication history discrepancies continued throughout the study, despite an encouraging uptake of the MAP forms and nurse education.
Limitations
The study was open to many sources of bias as the same pharmacist performed, documented and analysed the activities. Thus personal bias cannot be excluded. Some variation in patient type may have arisen between Phase 1 and 2 as there was a non-significant difference in length of stay between the groups. This difference in length of stay was probably due to the patient recruitment method, as patients were only seen once a week in Phase 1 and hence shorter stay patients were more likely to be missed in Phase 1.
Other limitations included inadequate follow-up of activities, an inability to accurately confirm whether patients were taking over-the-counter products and herbal medications in Phase 2, and a shortage of suitable patients for interview via videoconference. Fewer clinical consultations occurred than had been originally anticipated, possibly due to the high proportion of older patients admitted to the facilities and hence a lower level of independence with medication management. Accessibility to the fixed videoconference equipment may also have reduced the patient numbers. Ward-based, mobile videoconference equipment would have helped to overcome this. It is unknown as to what degree the training provided during Phase 1 affected the results obtained during Phase 2. However, it is likely that a combination of training and regular follow-up from the remote pharmacist contributed to these positive outcomes.
Conclusion
The implementation of a telepharmacy service to two rural hospitals suggested a trend towards better documentation of medications, reduced medication risk and improvements in the overall nurse supply system. Responses to questionnaires sent out to doctors, nurses and patients showed that the service was a valuable resource at sites which previously had no pharmacy input, while also helping to achieve a minimum standard of pharmaceutical review. The telepharmacy service has the potential to avert patient harm. Videoconferences enabled a good rapport to develop between local staff and the remote pharmacist.