
Abstract
We conducted a six-month randomised controlled trial of home telemonitoring for patients with chronic obstructive pulmonary disease (COPD). A total of 40 stable patients with moderate to severe COPD who had completed pulmonary rehabilitation took part. They were randomised to receive standard care (controls) or standard care plus home telemonitoring (intervention). During the monitoring period, patients in the telemonitoring group recorded their symptoms and physical observations twice daily. The data were transmitted automatically at night via the home telephone line. Nurses could access the data through a website and receive alerting email messages if certain conditions were detected. The patients completed the St George's Respiratory Questionnaire, Hospital Anxiety and Depression and the EuroQoL EQ-5D quality of life scores before and after pulmonary rehabilitation, and then periodically during the trial. There were significant and clinically important improvements in the scores immediately following pulmonary rehabilitation, but thereafter there were no differences in quality of life scores between the groups at any time, or consistently within either group over time. The study showed that telemonitoring was safe but, despite being well used, it was not associated with changes in quality of life in patients who had stable COPD.
Introduction
Despite better understanding of disease mechanisms and treatment standardisation, 1 chronic obstructive pulmonary disease (COPD) remains a leading cause of death and morbidity worldwide 1,2 with patients remaining extensive health-care users. 3 Quality of life (QoL) is reduced in COPD for many reasons, 1,4,5 even in stable, well-managed outpatients. 6 Despite good improvements in QoL following pulmonary rehabilitation (PR) it often deteriorates over time. 7 Repeated PR can stabilize QoL, even if exercise tolerance and lung function continue to decline 8 but this requires substantial resources and the benefits of successive cycles of PR become smaller. 8
Integrated case management (where simultaneous input from different specialities is applied simultaneously and adapted to the changing needs of the patient) has improved QoL in COPD, 9 but timely and accurate data transfer are vital. Information technologies have helped integrated case management to reduce hospitalisations for COPD. 10 Videoconferencing is well established in lung cancer multidisciplinary meetings 11 but little use has been made of videoconferencing for COPD work. Telemonitoring has been used to reduce admissions and costs in the home management of chronic respiratory failure 12,13 and for conducting remote outpatient consultations. 14,15
Regular home telemonitoring by a specialist team might improve or sustain QoL gains after PR by making patients feel more secure and by avoiding unnecessary doctor visits. Since worsening symptoms are usually present for days before patients with COPD are admitted to hospital with an exacerbation, 16 remote monitoring might allow earlier intervention to ameliorate exacerbations which themselves worsen QoL in COPD. 17 Alternatively, such an active monitoring process might worsen QoL by making patients feel under increased control from clinical staff, and being continually reminded about their illness by completing daily questionnaires.
The Better Breathing Study 17 aims to improve the care pathway for COPD by implementing integrated home-hospital and rehabilitation services. The present study was conducted to see if home telemonitoring is feasible and whether it improves QoL for patients.
Methods
We conducted a randomised trial followed by a six-month passive (observational) period. Ethics approval was obtained and the trial registered (ISRCTN 41424840).
Participants
A total of 99 subjects were identified from our PR database. The exclusion criteria and patient flow chart are shown in Figure 1. We approached eligible patients until we obtained 40 patients with the following: a primary diagnosis of moderate to severe COPD, according to a standard definition and prescribed optimum medication, 1 who had completed at least 12 from 18 sessions of our outpatient PR programme. They were enrolled a median of eight months after completing PR (range 2–19 months). None of the patients were using pulmonary ventilation at home.
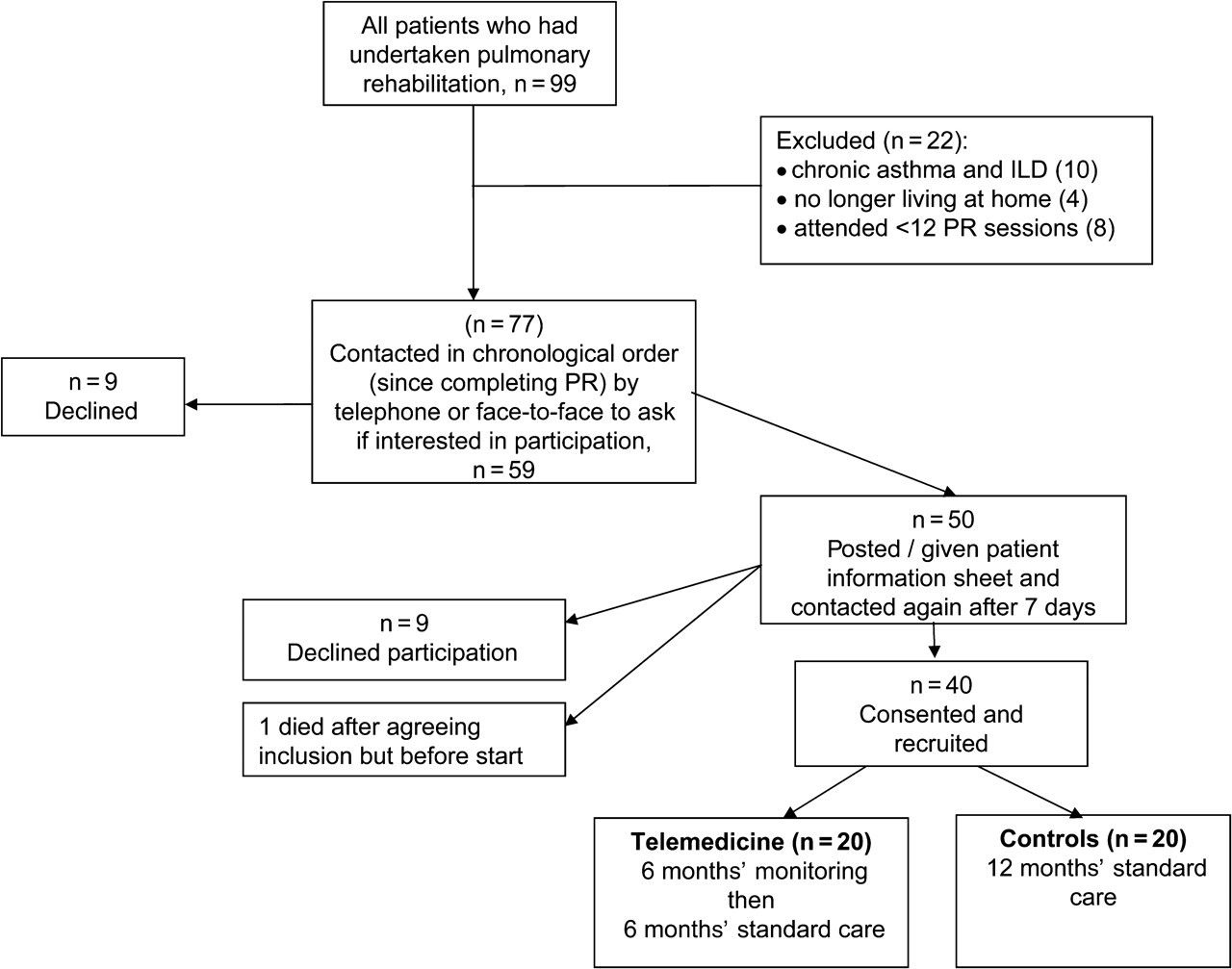
Patient flow chart
All participants had to be known to our community-based Chronic Disease Management Team (CDMT). If contacted, a member of the CDMT could visit the patient at home within one working day for clinical assessment, take sputum cultures and recommend treatment escalations (e.g. home steroids or home antibiotics). The CDMT liaised with general practitioners (GPs) and was in regular contact with the hospital respiratory consultants to discuss any difficult cases. Patients were otherwise on optimum medications.
Procedure
Following consent, subjects answered some baseline questions, including whether they were a regular Internet user which was used as a surrogate for computer ability. Occupation was used to estimate socioeconomic grouping according to established criteria. 18 Participants were randomised into two groups using a random number generator. Allocation used sealed opaque envelopes. Those in the control group received standard care, including CDMT support for 52 weeks.
Those in the intervention group (telemonitoring) received standard care plus a handheld telemonitor (Docobo Health Hub, Docobo Ltd, Bookham, UK) for 26 weeks. Then the monitors were removed, followed by standard care only for a further 26 weeks. The monitor connected via an ordinary telephone line.
A separate team installed the monitors and trained subjects in their own homes in January 2008. Each patient training session lasted for less than one hour. The installation team also dealt with any technical problems and had to visit two patients over six months when the signal was lost. The CDMT received two training sessions each lasting approximately one hour from the equipment manufacturers before the project started.
Following installation of the home monitors, patients provided answers to questions, twice each day regarding the condition of their chest over the preceding day or night. Patients were not sent reminders. Patients recorded their oral temperatures at home, using a manual thermometer (model FT04-1, Beurer, Ulm, Germany) and typed the result into the telemonitor. They then placed their index finger into a pulse oximeter probe (Nonin Inc, Minnesota, USA) connected to the monitor.
The data were transferred to a central server at 02:00 daily via the home telephone line. Health professionals could access the server via a secure Internet connection. If there were seven consecutive days without a data upload to the central server, a member of the CDMT telephoned the patient or sent a message to the monitor's screen.
If two or more of the following occurred in a single monitoring session, then an email message was sent automatically to alert the CDMT and copied to the hospital respiratory nurses:
Any question scoring ‘much worse than usual’; Pulse rate greater than 120 per minute; Oxygen saturations less than 88%; Temperature greater than 38.5 C.
The CDMT telephoned the patient when an email alert was received.
Both patient groups were instructed to seek help from their GP or an emergency doctor if they felt that urgent treatment was needed. It was emphasised that the monitor was not a replacement for standard support but was intended to work in conjunction with it. The CDMT and hospital nurses could liaise with hospital or primary care medical teams and none of the other clinical staff (e.g. hospital doctors and GPs) knew the telemedicine group allocation.
Quality of life measures
Patients in both groups completed the St George's Respiratory Questionnaire (SGRQ), and the Hospital Anxiety and Depression Score (HADS), both pre- and post-PR.
Following enrolment into the trial, patients in both groups repeated these scores and the EuroQoL EQ-5D questionnaire via face-to-face interview at baseline (0 weeks), and then via postal survey at 4 weeks, 25 weeks (just before the monitors were removed from the intervention patients), 30 weeks (shortly after the monitors were removed) and after 52 weeks. The intervention group had home monitors for the first six months. After the monitors were removed they had a further six-month period of passive-intervention, i.e. 12 months in total. The control patients had their QoL measured at similar times during the 12 months.
Statistical analysis
We used the Statistical Package for Social Sciences (SPSS) version 16.0 (Chicago, Illinois). Following confirmation of normality, paired sample t-tests were used to assess differences in questionnaire scores for the pre-PR and immediately post-PR periods. Following confirmation of normality and sphericity (Mauchly's test), repeated measures ANOVA models with the main factors ‘Time’ (levels: Baseline, Week 4, Week 25, Week 30, Week 52) and ‘Group’ (levels: ‘Standard Care’ and ‘Docubo’) were used to assess the magnitudes of the individual questionnaire scores. Interaction effects among the main factors were also assessed.
When ANOVA indicated a significant effect of time on the questionnaire scores, post hoc testing using the Bonferroni adjustment identified the pair-wise locations of the significantly different scores.
Our primary aim was to test the null hypothesis that there was no difference in total SGRQ score between patients with COPD receiving home telemonitoring and those receiving standard support, over time. Our secondary aims were to test the null hypotheses that there was no difference in HADS and EQ-5D scores between the groups at any time once they had completed PR.
We prospectively recorded health-care usage, participant views (on completion) and telemonitor usage to help explain any differences in QoL scores. A senior respiratory clinician (separate from the research team) independently reviewed the medical records of any deaths or withdrawals to determine if telemonitoring contributed towards adverse consequences, e.g. causing unusual delays in treatment.
Results
Table 1 describes the two study groups after PR and immediately prior to the telemonitoring trial. The telemonitoring group had a significantly longer period (number of months) since completing PR and had a slightly higher MRC dyspnoea score at baseline.
Characteristics of the two groups at baseline. The values shown are the mean (SD) or median (interquartile range)
*P = 0.02
† P = 0.006
‡ P = 0.03
SGRQ scores
The total SGRQ scores were improved immediately following PR, with a mean reduction in score of 7.2 (95% CI = 3.1 − 11.4, P = 0.001). This change was deemed clinically important.
The ANOVA indicated: (a) that there was no Time × Group interaction effect on the SGRQ score (P = 0.19), indicating that the telemonitoring and control groups had similar scores over time; (b) that there was a significant and large main effect of Time on the score (P = 0.023), and this was attributable solely to a significant (and clinically important) larger score at Week 30 compared with Week 4 (mean difference 6.2 (95% CI = 0.4 − 12.0, P = 0.031); and (c) that the score was not influenced by group (P = 0.903). Figure 2 shows the SQRQ scores at each of the assessment points (separated by group for the intervention/observation period only).

St George's Respiratory Questionnaire (SGRQ) scores in the two groups. The error bars represent the SEM
Hospital anxiety scores
Hospital anxiety scores were improved immediately following PR (mean score reduction = 1.5; 95% CI = 0.6 − 2.4, P = 0.002).
The ANOVA indicated: (a) that there was no Time × Group interaction effect on the score (P = 0.83), indicating that the telemonitoring and control groups had similar scores over time; (b) that there was a significant effect of Time on the score (P = 0.006), and this was attributable solely to a larger score (trend only) at Week 52 compared with Week 0 (mean difference 2.9; (95% CI = −0.01 − 5.9, P = 0.051); and (c) that the score was not influenced by Group (P = 0.52). Figure 3 shows the hospital anxiety scores at each of the assessment points (separated by group for the intervention/observation period only).
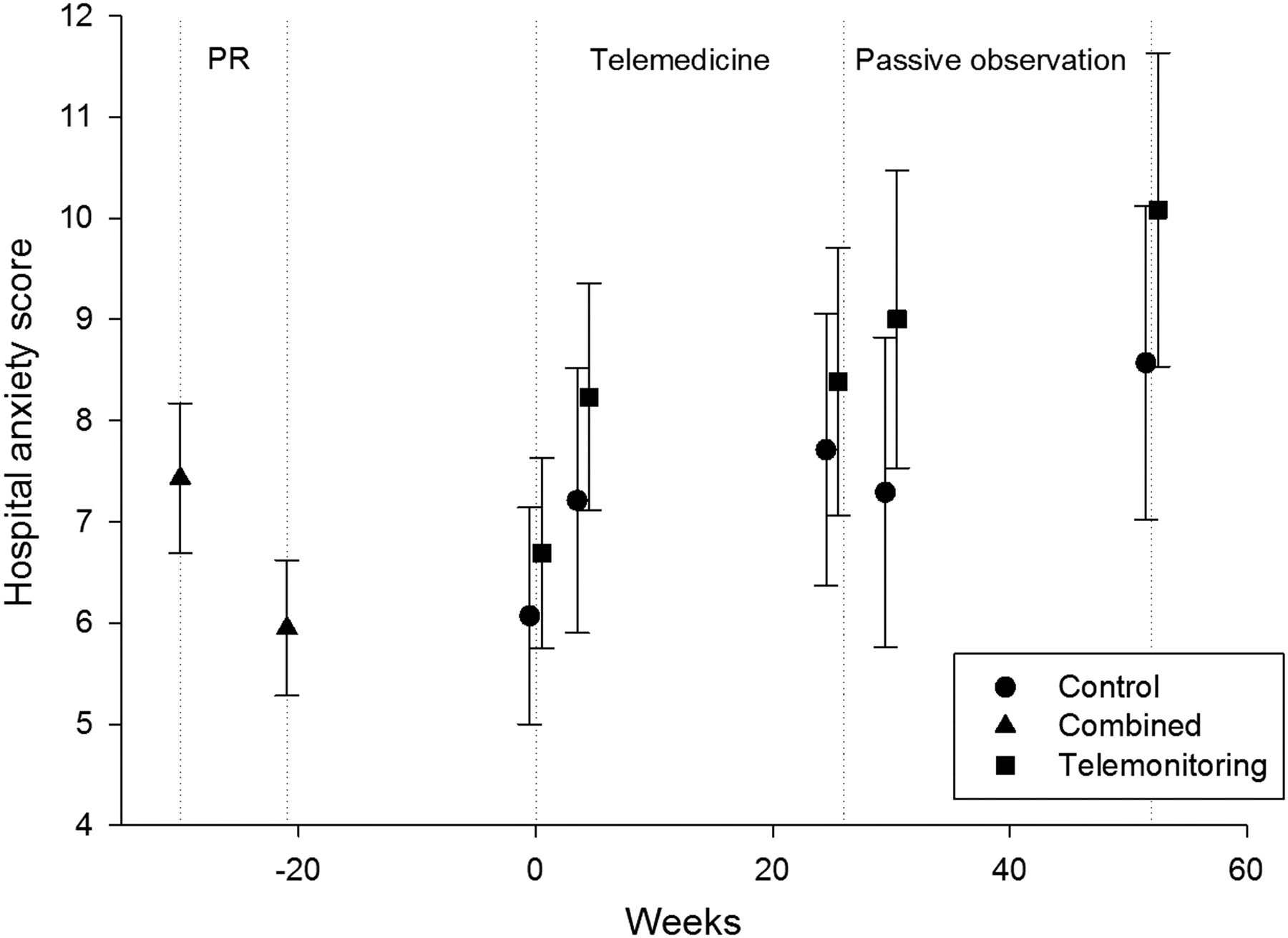
Hospital anxiety scores in the two groups. The error bars represent the SEM
Hospital depression scores
Hospital depression scores were improved immediately following PR (mean score reduction = 1.2; 95% CI = 0.2 − 2.2, P = 0.022).
The ANOVA indicated: (a) that there was no Time × Group interaction effect on the score (P = 0.70), indicating that the telemonitoring and control groups had similar scores over time; (b) that there was a significant effect of Time on the score (P = 0.022), and this was attributable solely to a significantly larger score at Week 52 compared with Week 4 (mean difference 1.7; 95% CI = 0.05 − 3.4, P = 0.040); and (c) that the score was not influenced by Group (P = 0.35). Figure 4 shows the hospital depression scores at each of the assessment points (separated by group for the intervention/observation period only).

Hospital depression scores in the two groups. The error bars represent the SEM
EQ-5D scores
EQ-5D scores were not recorded pre- or immediately post-PR. The ANOVA indicated: (a) that there was no Time × Group interaction effect on the score (P = 0.64), indicating that the telemonitoring and control groups had similar scores over time; (b) that there was no effect of Time on the score (P = 0.15), and this was attributable solely to a significantly larger score at Week 30 compared with Week 4 (mean difference 6.2; 95% CI = 0.4 − 12.0, P = 0.031); and (c) that the score was not influenced by Group (P = 0.45). Figure 5 shows the EQ-5D scores at each of the assessment points (separated by group for the intervention/observation period only).
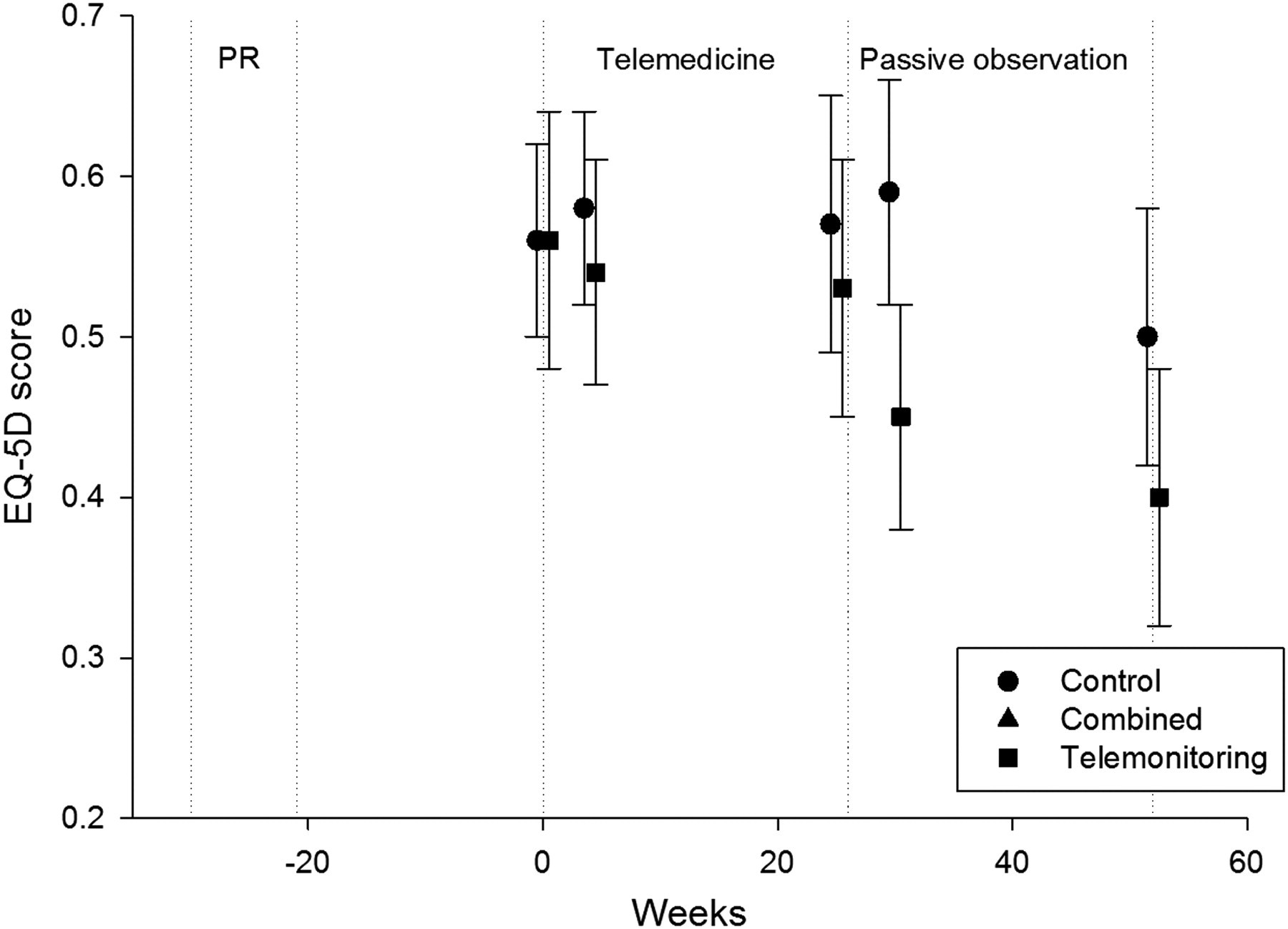
EQ-5D scores in the two groups. The error bars represent the SEM
There were no differences in the number or duration of hospital admissions or in any CDMT contacts (P > 0.15 throughout). There were two deaths in the telemonitoring group – one man died after 15 days in hospital of multi-organ failure following a gastrointestinal haemorrhage; one lady died 2 months after being admitted to a nursing home with a diagnosis of ‘old age.’ Neither had used their monitors for 15 days before their death and neither death was attributed to previous use of the monitors. There was one withdrawal in the telemonitoring group after three months because the patient found it too cumbersome, when she wanted to travel. All three had been good users prior to withdrawing and their last recorded symptoms, heart rate and oximetry showed no worrying trend. We obtained no user satisfaction ratings from these three subjects.
None of the 17 telemonitoring patients, who completed the study, reported difficulties in using the monitors. The majority (15 or 88%) found it ‘helpful’ or ‘very helpful’; one patient ‘neither agreed nor disagreed’ that it was useful and one patient found it ‘inconvenient’.
Discussion
For stable COPD patients, who have completed PR and are already supported by a specialist CDMT team, continuous home telemonitoring with alerts was not associated with any important difference in multiple QoL measures. That there were no consistent changes in any QoL measure in the telemonitoring group, during the monitoring versus passive-observational periods, further supports this. We could not reject the null hypothesis. This lack of change compares with significant and clinically important improvements in the same group using the same QoL measures, immediately after PR.
Other studies have applied different types of telemedicine in COPD. Mair et al. reported technical difficulties 19 and patient reticence 20 in implementing real-time home video monitoring at set times for COPD patients. It is possible that our implementation was easier because the technology was more reliable and easier to use. We chose simple equipment that did not need an Internet connection. As we did not attempt real time monitoring, our patients had more flexibility in inputting data. Our subjects were recruited from patients well known to the specialist teams, rather than from emergency departments, 20 and the 18 who refused trial participation had similar socio-demographics and QoL scores post-PR to the participants (no significant differences throughout). The most important reason for ease of recruitment was probably because we offered telemedicine in addition to rather than instead of home CDMT visits.
We hoped that continuous monitoring might improve patient confidence, ameliorate exacerbations or improve QoL indirectly by reducing unnecessary travel (visits) or the burden on caregivers. In another randomised controlled trial (RCT) assessing the impact of telemedicine on QoL in respiratory disease, Whitten et al. studied patients with COPD and/or congestive heart failure (CHF). Their intervention group was prescribed a combination of conventional face-to-face and telemedicine visits (n = 83), and a control group received only usual home care (n = 78). Data were collected via the Short Form 36 (SF-36), Outcome and Assessment Information Set and patient charts. Like us, they found that the addition of telehealth was not a significant predictor of health and well-being. Interestingly, those receiving telehealth had worse ratings on the SF-36 general health subscale after the intervention, but this was only significant when controlling for a number of key variables in the model and overall, patients were satisfied with the technology and the way that care was delivered via this modality. 21
In a nonrandomised study, Trappenburg et al. found that health-care utilisation (especially hospital admissions) was lower in 59 patients who received a home telemonitoring device, the Health Buddy, for 6 months compared to a similar cohort of 56 patients with COPD. They also found no significant changes in health-related QoL as measured by the Clinical COPD Questionnaire, at follow-up between both study groups. 22
The telemonitor that we used was compact, simple to use and has been used successfully in other clinical conditions. 23–25
One reason for the lack of benefit in QoL in our patients could be explained by the exacerbations. We found no differences in the number or duration of hospital admissions, emergency room attendances or self-reported exacerbations between the groups at any time point. There were no differences in clinic attendances, the duration or number of CDMT contacts (details omitted for brevity). We emphasise that our system was not real-time and there was usually a 12–24 hour delay between the patient providing data to the monitor and the data being accessed by the CDMT, but we do not believe this is the reason for the lack of benefit because most COPD exacerbations develop over several days. 16 Dale et al. reported the effects of a different home monitoring system (recording pulse, oxygen saturation, body weight) for patients with COPD over a three-month period. 26 This was popular with patients and seemed to avert some of the predicted increase in hospital admissions but it is difficult to separate the effects of the monitoring from the protocol's additional daily telephone calls. Vontetsianos et al. used telemedicine monitoring via a visiting nurse in 18 well-motivated patients with advanced COPD who had previous admissions. They reported a decrease in hospitalizations, emergency visits and use of health services, but the patient's disease knowledge and self-management also improved. 27 Again, it is difficult to see what additional benefit the real-time video link offered on its own, as it was only set up during the nurse home visits. Maiolo et al. studied 30 patients with various respiratory illnesses, on long-term oxygen. In total, 23 completed the study and twice weekly home monitoring of heart rate and arterial oxygen saturations was found to be associated with a 50% reduction in hospital admissions, a 56% reduction in acute exacerbations and overall cost savings of 17%. Patients were satisfied with the quality of the personal telemonitoring in 96% of cases. 28 None of these studies recorded QoL scores and none were RCTs.
We did not use telemedicine to deliver a home exercise programme or other intervention to improve QoL. Such an active process of educational approach, rehabilitative prescription and life style changes is difficult to deliver effectively through a simple device alone but a change in QoL might occur if this was combined with a continuous educational reinforcement by nurses.
We believe that we used appropriate measures of QoL. Since its invention 29 the SGRQ has been widely validated in assessing QoL in COPD and a change in 4 units on the total score is considered clinically important. 30 We found significant and clinically important changes immediately after PR, in keeping with most other studies. 31 We did not analyse the subscales of the SGRQ, as the clinical importance of these subscales is still debated, particularly in small studies. The EQ-5D 32 and HADS 33 have also been used extensively in COPD.
It was a pre-requisite of the Better Breathing Study that participants had completed PR. However, our home CDMT service has also been associated with reduced COPD admissions. 34 It is therefore likely that our participants were already optimized, i.e. additional telemonitoring would have produced little extra clinical benefit. We believe this is the main reason that we obtained a negative result. The relatively good baseline QoL scores and persistent low number of health-care contacts in both groups (e.g. only four admissions in the telemonitoring group versus eight in the control group during the six-month intervention) reflect the well-being of our study population. As our subjects were so stable even eight months after PR, it is unlikely that telemonitoring offered for at least a year within completing PR would add very much.
The strengths of our study include its randomised design and it being based in a non-teaching hospital unit serving a town and rural population, so it can be generalized to most settings. The assessors of the QoL scores were unaware of group allocation and we used more than one measure of QoL, all of which showed the same trends. Our subject demographics, criteria for PR and changes in QoL following PR are typical. 31 Our telemonitoring technology was simple and readily deployed. It provided a median of 97% available data capture in the monitoring period. We had 85–90% response rate for the QoL questionnaires throughout the study.
The main weakness of the study was its small size. We chose 40 patients mainly due to funding constraints, but also because we felt this would be adequate to assess safety and feasibility. The study size made it difficult to control for all potential confounding factors at baseline and when comparing more than 13 variables, it is likely that some differences will occur through chance, despite randomisation. We do not know whether the time difference from completing PR to trial entry is important.
There have been calls for better-designed studies of telemedicine, noting in particular the lack of RCTs. 35 The present study represents the first RCT of telemedicine in the home monitoring of stable, already optimized COPD patients, to report specific QoL outcomes. It shows that telemonitoring is safe but, despite being well used, it was not associated with changes in QoL.
In summary, we believe that stable COPD patients can be followed up by their primary care teams without telemonitoring. Thus it is important that future studies on telemedicine in COPD concentrate on other patient groups, such as those with multiple hospital contacts, those unable to complete PR and those without community team support.
Footnotes
Acknowledgements
We are grateful to Pat Hodgson for collecting pulmonary rehabilitation data, to Jeanette Munn, Annette Coslett-Hughes and Marilyn Beebe from the Careline Telecare Team; to Dr Yasir Syed and Dr Gareth Collier; to Helen Rees, Jenny Wiley and Jane Douglas of the COPD CDMT team; to Sarah Rees from Informing Healthcare Wales; to the staff at the Medical Electronics Department, Prince Philip Hospital and to Docobo Ltd, UK. Financial support was provided by an EU grant (C046225).