
Abstract
A telemedicine application has a better chance of being accepted if the users can easily handle it and if the application fulfils the clinical needs of both patients and professionals. This requires a methodology for development in which three key matters need to be dealt with: (1) clinical content; (2) design; and (3) outcome. Concerning the clinical content, telemedicine services for patients with chronic disorders that aim to increase their level of functioning need to monitor aspects of the patient's functioning and provide adequate feedback about this. Promising parameters of functioning are related to general physical activity and muscle activation patterns. Providing adequate feedback requires choices about the content of the information, the modality of the feedback and its timing. Unfortunately, research into effective feedback strategies is still in its infancy. Concerning the design it appears that the different stakeholders involved speak different languages, that there is a lack of knowledge about aspects related to acceptance and a lack of good methods to define user requirements. Scenario-based requirements analysis is a promising technique to overcome these barriers. Concerning the outcome, evaluation of telemedicine services in everyday clinical practice has been mainly directed at measurement of technical performance and user satisfaction. Large scale clinical evaluation studies with multiple end points are needed. This development methodology with its three aspects was used for a myofeedback-based teletreatment service. This showed that telemedicine applications can be developed that have the potential to make health care more effective, efficient and accessible.
Introduction
The Western world needs to find ways of coping with the increasing number of elderly people and people with chronic diseases who need care for long periods of time. As chronic diseases cannot be cured, treatment aims to relieve symptoms and related complaints. Interventions like physiotherapy and multidisciplinary rehabilitation are therefore becoming more important. Various studies have shown that these treatments are on average effective, although for 30–50% of the patients these treatment do not have the desired effects. 1–3 This is disappointing for the patients as well as the professionals.
Different reasons for these disappointing results have been given. Patients with chronic disease are often cared for by multiple professionals. As a consequence, communication between these professionals, and between the patient and the professionals, may be less than ideal, which affects the quality of care. 4,5 Furthermore, treatments are often insufficiently tailored to the individual patient 6 and also insufficiently aimed at the patient's self management. 7 In addition, patients often experience problems with translating the skills learned from health professionals to their own home and work situation with the result that they stop doing their essential exercises. 8 This set of interacting reasons is in line with the chronic care model of Wagner, 9 which assumes that an informed activated patient and a prepared, proactive practice team are two essential parties needed to produce improved outcomes.
Besides the increasing number of people who need care for long periods and the quality of treatment, the costs of health care also need to be considered. Costs of care are high and are expected to further increase unless health policies are changed. 10 More care needs to be delivered, with a higher quality, better tailored to the needs of the individual patient without costing more money or personal effort.
There are high expectations of technology, especially Information and Communication
Technology (ICT), to make health care more effective and efficient. As a result there
have been many initiatives related to ICT and care. As we have previously pointed out,
11
these can be divided into two main categories: The use of ICT to improve current care processes by making information more
accessible. Examples of these applications are electronic medical records and
applications that improve logistics; The use of ICT for services that enable the patient to be treated in their own
daily environment. Examples of such applications are teleconsultation between
patients and professionals
12
as well as between professionals mutually,
13
remote monitoring and remotely supervised treatment.
14,15
Despite the potential of telemedicine to increase the quality, reduce the cost
and improve the accessibility of the health-care system, 75% of all initiatives fail to
survive the research phase and are not implemented as routine.
16
This brings us to the big question: how to realize telemedicine applications that
will be successful in treatment and can be integrated successfully into the health-care
system. The present paper describes a method involving three key elements for the
realization of successful telemedicine applications. We have used this method for one
specific application, a myofeedback-based teletreatment service for the treatment of
patients with chronic neck and shoulder pain.
Methods
If a telemedicine application is not accepted by its users, the patients and
professionals, it will never be implemented successfully in everyday care. Generally
speaking, a telemedicine application has a better chance of being accepted if the users
can easily handle the application and if the application fulfils the clinical needs of
both patients and professionals. This requires three key matters to be dealt with: Clinical content. Telemedicine services for patients with chronic disorders
that aim to increase the patient's level of functioning need to be able to
monitor aspects of the patient's functioning, as well as to provide the patient
with adequate feedback about this; Design. Telemedicine applications need to be designed so that they fit the
needs of the users; Outcome. The systems need to have positive effects on care in terms of
effectiveness and efficiency.
These aspects are summarised in Figure 1.

Three essential elements in the development of telemedicine systems
Clinical content
The clinical content element consists of two parts: the application needs to assess the patient's functioning in an objective way and it needs to provide feedback to the patient in order to enable him or her to change in response.
Assessing the patient's health status or functional level
Many people with chronic disorders develop a vicious circle as described in various neurophysiological 17,18 and cognitive behavioural models. 19,20 All models hypothesize that patients change their physical functioning as a consequence of their disease. However the way that people change differs, and there is insufficient evidence about who develops a chronic disorder and via which mechanism. In addition, there is insufficient research evidence about the functional status of patients during everyday life, which is necessary to define a good starting point for a telemedicine service. Promising parameters, related to the functional status of patients with chronic diseases, are general physical activity patterns and muscle activation patterns.
The average general activity pattern measured by a 3-D accelerometer worn by patients with various chronic diseases for seven consecutive days is shown in Figure 2. This figure indicates that various patient groups show differences with respect to controls of a much stronger decline in activities over the day. For a telemedicine application this means that the activity pattern over the day is important in obtaining insight about physical functioning.
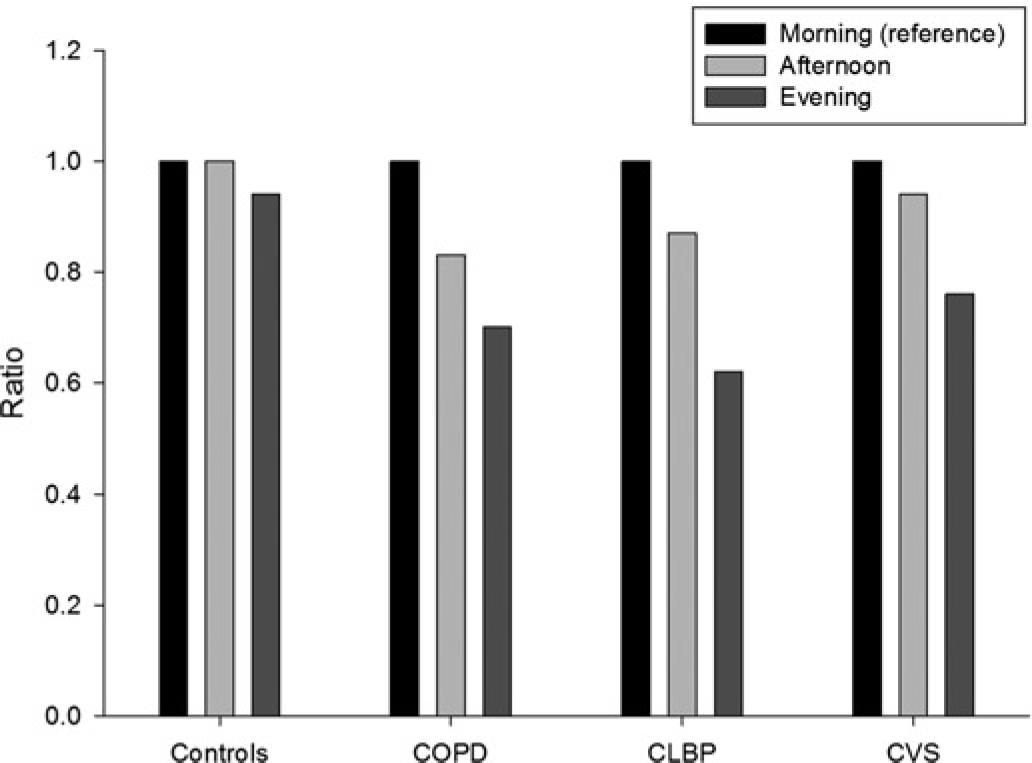
Activity levels in the morning, afternoon and evening expressed as a ratio with respect to the morning level for patients with chronic lower back pain (CLBP), chronic fatigue syndrome (CVS), chronic obstructive pulmonary disease (COPD) and a healthy control group (Controls)
Considering the muscle activation patterns, various experimental studies (e.g. van der Hulst et al. 21 ) have shown that patients with chronic pain have higher muscle activity, i.e. they show problems with relaxation of their muscles during everyday tasks, like walking. Thus a telemedicine application that aims to normalize muscle activation patterns needs to be able to quantify the muscle activation patterns and especially the level of muscle relaxation during everyday tasks.
Feedback
Once we are able to quantify the functioning of patients in their daily environment,
the next step is to give the patients insight into their functioning by providing
adequate feedback. Feedback, first defined by Rosenblueth et
al.,
22
is essential in the case of learning, no matter what is being learned.
Feedback can be divided into intrinsic feedback and extrinsic feedback. Intrinsic
feedback refers to the sensory-perceptual information of an individual which is
available when an activity is being performed. Extrinsic (augmented) feedback is
feedback which is provided on top of intrinsic feedback, mainly by external sources
such as a therapist or a technical device. In the case of augmented feedback for the
treatment of patients with chronic diseases, the feedback has three different aims.
23,24
The three aims are: Reflecting/awareness. Patients are given a reflection on their own
functioning with the aim of making them aware or increasing their awareness
of the inadequate aspects of it; Motivating. After people have become aware of the inadequate aspects of
their functioning they must be motivated to change. This function of
feedback derives from psychological oriented theories like the Social
Cognition Theory,
25
Theory of Planned Behaviour
26
and the Trans Theoretical Model
27
which state that changing functioning or behaviour is a dynamic
process. It is the consequence of the interaction between the person, the
behaviour and the environment, as well as a staged process; Changing. This function is subdivided into two different aspects: (1)
starting from the staged process of change, intentions need to be
transformed into concrete actions to change and once changed, adequate
functioning needs to be maintained; (2) to be able to change it is important
that patients have adequate motor skills to perform adequately, i.e. motor
skills learning.
28,29
An overview of these different functions of feedback is shown in Figure 3.
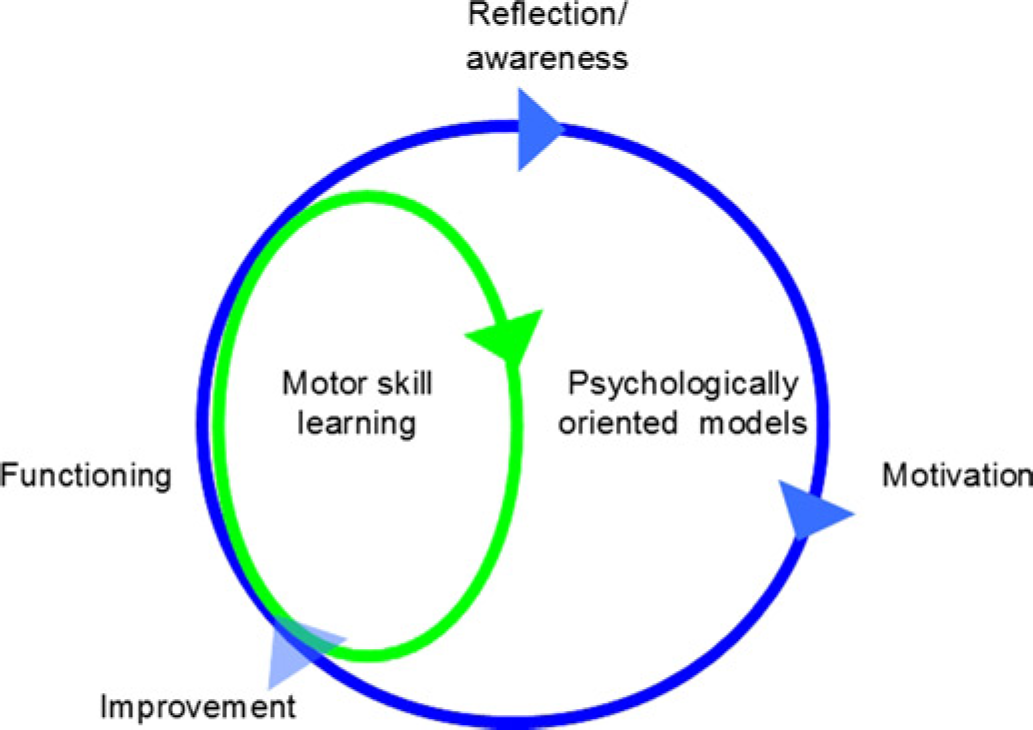
Schematic overview of the functions of feedback to produce improved functioning of patients with chronic diseases, taking into account psychological theories as well as the theories of motor skill learning
In conventional treatment to improve the physical function of a patient there is
usually face-to-face contact between the professional and the patients, where the
professional provides direct feedback by talking and showing the patient how to move
properly. In telemedicine treatment the challenge is to replace some or all of the
face-to-face feedback by feedback provided by technology. This requires choices to be made.
30
The options include:
Content of feedback. Three choices have to be
made about the content of the feedback. Will it be feedback on results (FR) or feedback on performance
(FP)? FR gives information about the performance with respect to
the goal, whereas FP gives specific information about how the task
is being performed and is therefore much richer in its information.
Research into these two different concepts has mainly focused on
learning motor skills and shows that for simple tasks both forms of
feedback are effective,
31–33
although some studies show that FP is more effective than FR.
34–36
Will the feedback be positive or negative? For simple tasks
negative feedback is more effective than positive feedback. Ashby
and O'Brien
37
showed that in more complex information integration tasks,
both forms of feedback are effective, but that the combination of
the two is most effective. When providing feedback there is always a comparison of the
patient's functioning with some form of norm. The patient's
functioning can be compared with their functioning at another
moment, i.e. a temporal comparison.
38
Alternatively a comparison can be made with a group of other
people, i.e. a social comparison.
39
Which form of comparison is most effective for improving
functioning is not yet known. Proper et
al.
40
have shown that social comparison has a positive influence
on awareness but not on the actual performance.
Modality of feedback. In conventional care
extrinsic feedback provided by the health-care professional is rich in
modality. A professional can talk, show and let the patient feel how to move
in a proper way. In technology-based feedback, choices need to be made about
which modality to use and there is also a choice between visual, auditory
and sensory feedback. Which modality is most effective has mostly been
researched in young health people and to a lesser extent in patients with stroke,
24,36
but the evidence has not been consistent. As well as the modality,
the apparatus for providing feedback needs to be considered, e.g. a device
such as a mobile phone, an object in the surroundings of the patient such as
a light, a computer or even a robot. The choice of the apparatus will
probably depend on personal preferences and the context in which the
telemedicine application will be provided. For example, at work a patient
may prefer a different apparatus than at home. Another important aspect is
what information to add to the feedback to make it more personalized. Such
information may concern location, time or the weather.
Timing of feedback. The third aspect of
feedback that needs to be considered is the timing. Two choices can be made:
(1) feedback at
predefined times which can be further subdivided into feedback during the
performance of an activity (concurrent feedback) or after the activity has
been performed (terminal feedback). Also the frequency of feedback needs to
be considered, for instance continuously, after a certain amount of activity
or after every few seconds; (2) feedback when certain events occur, for instance when the
muscle relaxation is below a certain threshold. Which timing strategies are
effective needs to be investigated and in this research not only the effects
of timing on clinical outcome but also the preferences of patients and the
chance of developing dependency on the system needs to be considered. For
instance, Voerman et al.
41
investigated the effect of different timing intervals on muscle
relaxation and concluded that feedback every 5 seconds is not ideal and may
even be irritating to the patient.
Design
As many as 75% of telemedicine applications do not survive the project phase and can be considered a failure. 16 One important reason is that the different stakeholders involved have different ideas about the telemedicine application. This leads to miscommunication and developments that do not fit the needs of the users. The applications are not then accepted by the users. 42 Better insight into aspects that are related to acceptance of technology is important. It is known that acceptance is influenced by technical aspects of the system such as ease of use, individual characteristics like age, as well as the surroundings of the individual. 43 However, these aspects are too generic to use as a starting point in developing telemedicine applications. Thus, there is a lack of knowledge about factors that influence the acceptance of telemedicine applications. There is also a need for good definition of user requirements. The methods used most often for this purpose are interviews and focus groups.
A more modern technique with potential for telemedicine is scenario-based requirements engineering 44 (see Figure 4). A scenario is a chronological description of a certain event (or series of events) that take place when using an application and can be used as the starting point for developing a common vision among all stakeholders. Scenarios help to define the people, their roles and activities, as well as the functions of the telemedicine application and the context in which it will be used. Using this scenario as a starting point, functional and non-functional specifications can be defined from which technical specifications can be derived and a prototype can be developed. The prototype needs to be tested with users at an early stage to explore whether the application fits the requirements. 16
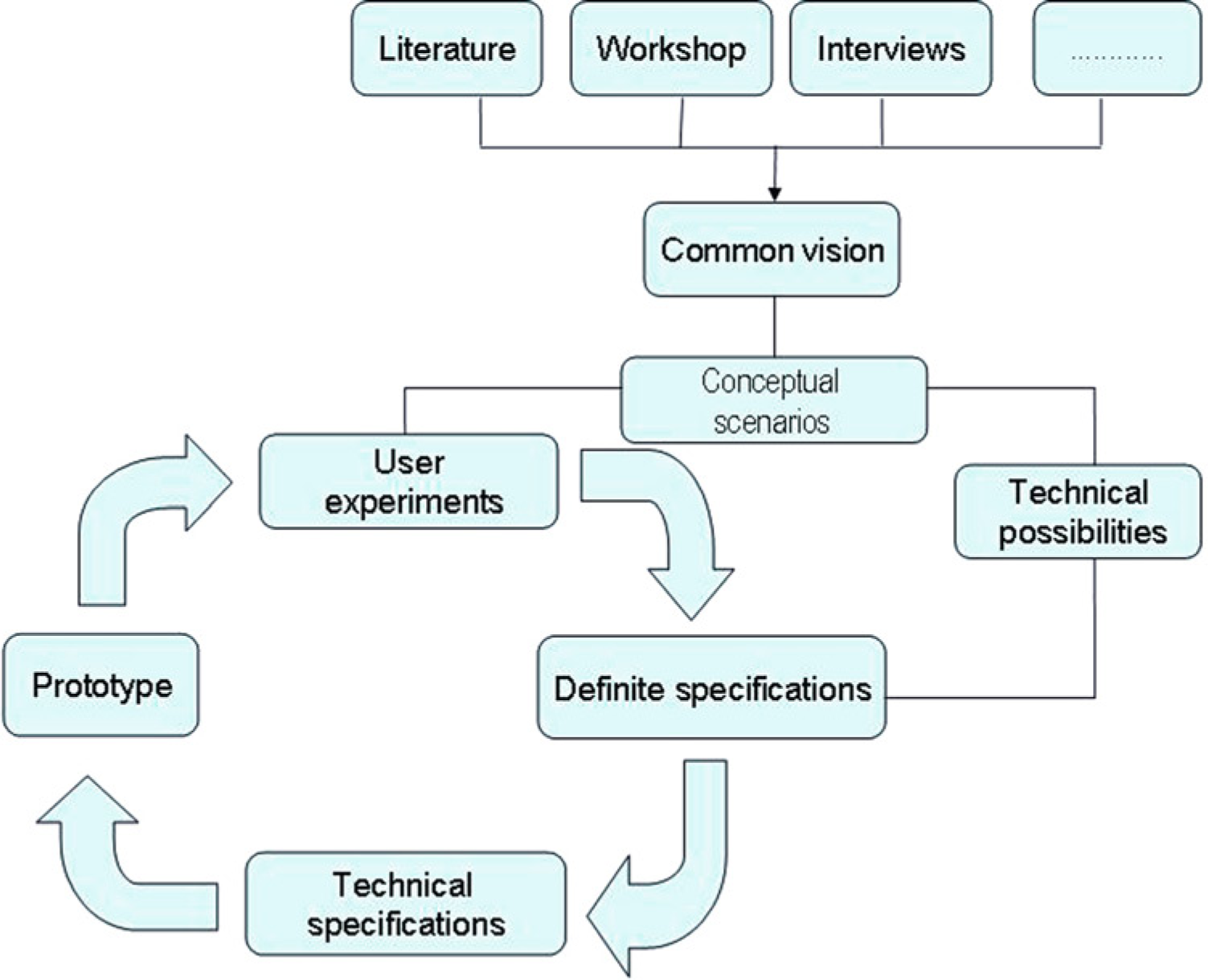
Overview of a scenario-based method to define user requirements
Outcome
Once the clinical content and the design criteria have been defined, a telemedicine application can be developed that meets the requirements of the users and that is able to monitor and give feedback on the functional status of the patient. The next step is to demonstrate the results when the system is used in everyday practice. Outcome measures usually focus on the technical feasibility of the system and on user satisfaction. 45 The results show that in general the applications are technically stable in clinical practice and that patients and professionals have a positive attitude towards using them. This type of evaluation is however not sufficient to justify subsequent large scale implementation. For this, a broader evaluation is necessary. DeChant et al. 46 have proposed a staged approach for the evaluation of telemedicine applications, starting early in the development phase. The first phase evaluation is aimed at investigating whether the requirements of the patients are met and whether the application is technically stable. At this stage the user group is small, because the results are mainly used to develop a more mature application.
After the first phase evaluation, a mature application evaluation (stage 2) focuses on clinical outcome. If these results are positive, evaluation becomes even more extensive, using multiple endpoints such as effectiveness, efficiency or accessibility of care (stage 3). The last evaluation phase (stage 4) focuses on external validity and investigates whether the application is as effective when implemented in places other than where it was developed.
Example
The three elements of the method are illustrated for the myofeedback-based teletreatment service for the treatment of patients with chronic neck and shoulder pain.
Clinical content
Experimental studies have shown that patients with chronic pain exhibit deviations in their muscle activation patterns with respect to asymptomatic controls. 47,21 This is reflected in an increased and prolonged muscle activation during and after physical and/or mental tasks, meaning a decreased capacity to relax their muscles. As the levels of muscle activations are often rather low, people are not aware of this lack of muscle relaxation. However these low levels are harmful because the same motor units of the muscle are continuously active, become exhausted and are then damaged. 48 Veiersted et al. 49 showed that a decreased ability to relax the muscles increases the chance of developing neck and shoulder problems. Thus lack of muscle relaxation is an important factor in the development of chronic pain.
Besides being an explanation for the development and maintenance of pain, poor muscle relaxation also offers a starting point for treatment. Treatment could consist of monitoring the level of muscle relaxation and providing feedback to the patient with the aim of increasing their awareness and enabling them to develop motor skills to increase the level of muscle relaxation. The norm considered useful for feedback is based on a longitudinal study 49 which showed that of a group of healthy secretaries who started working with muscle relaxation levels less than 20% of the time, had significantly higher risk of development of musculoskeletal neck and shoulder pain than those who had muscle relaxation levels higher than 20%. The 20% level is thus considered to be a healthy norm.
Design
Based on the clinical content, a scenario was developed describing the people, their roles and activities as well as the functions of the application and the context in which it was being used. Based on this scenario, the functional requirements were defined. Important criteria were that muscle relaxation needs to be monitored and feedback needs to be given when the level of muscle relaxation is insufficient. It was a requirement that the system could be used at the workplace, that people could put on and take off the system by themselves, that the system could be worn under the clothes and that the feedback would be private. Patients and professionals preferred to have teleconsultations as a part replacement for the face-to-face contacts. These requirements resulted in the system shown in Figure 5.

The Body Area Network (BAN) of the ambulant myofeedback treatment. The right-hand image is copyright MobiHealth B.V.
Muscle relaxation is measured with dry electrodes that are incorporated into a garment that people wear under their clothes during everyday life. The garment is connected to a device that vibrates quietly when the level of muscle relaxation is insufficient. 50 The patient data are sent wirelessly to a personal digital assistant (PDA) and on this PDA patients can see their own muscle activation data (i.e. this provides continuous feedback on performance). From the PDA, the data are transmitted to a web server which is accessible to the professionals. Once a week there is a consultation by telephone between the patient and the professional to discuss progress and make appointments for the following week. Treatment starts and ends with a face-to-face contact and lasts for four weeks.
Outcome
Evaluation of the telemedicine application started with the evaluation of only part of the system, namely the ambulant system worn by the patient. The first studies on this part were performed in patients with chronic whiplash disorders 51 and patients with work-related complaints. 50 The results showed that 55–60% of the patients experienced a clinically relevant reduction in pain and discomfort after four weeks of treatment. A randomized controlled trial was then performed comparing ambulant myofeedback (n = 41) with ergonomic consultation (n = 38) for patients with work-related neck and shoulder complaints in the Netherlands and Sweden. The results of this trial showed that 50% of the patients experienced a clinically relevant reduction in pain and disability, and these effects still existed after 6 months of follow-up. Compared to the control group no significant differences were found. 51 From these studies it was hypothesized that health care would be improved by use of the teletreatment service.
The first trial of the fully developed teletreatment service was conducted with 10 female workers suffering from neck and shoulder pain related to computer work. It showed that in 78% of the remote counselling sessions, sufficient quantities of data were available at the server for the therapist to make an assessment of muscle tension needed for the remote counselling sessions. Subjects reported high satisfaction with the remote counselling. However, they were less satisfied with the technical functioning of the myofeedback system. Eighty percent of the subjects reported a reduction in pain intensity and disability directly after treatment. Based on this study, it can be concluded that myofeedback-based teletreatment is technically feasible and shows promising clinical results. 15 This study also resulted in recommendations for further improvement of the application. The results are presented in the papers of Sandsjo et al. 52 and Kosterink et al. 53
Discussion
The present paper describes a method involving three key elements for the realization of successful telemedicine applications. The method is illustrated for a specific application, the myofeedback-based teletreatment service for patients with chronic neck and shoulder pain.
It appears that parameters reflecting physical functioning can give good insight into the health status of a patient and can therefore be used as starting points for telemedicine interventions. Parameters that have good potential in this respect are those related to general physical activity and to muscle activation. However, experiments also show that different disorders are reflected in these parameters in different ways. In addition, there has been little research investigating the functional status of patients in everyday life in an objective manner. This is needed for several chronic disorders to define good starting points for telemedicine services.
Once the functional status of a patient can be assessed objectively in everyday life the next step is to provide feedback to the patient in order to enable the patient to change. The challenge is to develop feedback strategies in telemedicine systems that can at least partly replace face-to-face contact with the professional. However, research into effective feedback strategies for changing functional status is still in its infancy. Research so far has only been performed for very simple tasks, healthy subjects or with a focus on motor relearning in patients with neurological disorders. There have been no studies that focus on the effects of feedback strategies on functional status or everyday tasks.
Concerning the design of telemedicine applications, one can conclude that many telemedicine applications are designed according to the technology, with the consequence that they do not fit the requirements of the users and therefore fail to become accepted. Miscommunication between the various stakeholders, lack of insight into factors related to acceptance of telemedicine applications, as well as methods and techniques to define the user requirements all represent important barriers. Scenario-based requirements analysis is a promising new method which can overcome these potential barriers. Because users are often unfamiliar with telemedicine services, they have difficulty in defining their needs and desires. Scenarios are also considered to be of potential benefit in formulating a good set of requirements. 54
Outcome evaluation of telemedicine services in everyday clinical practice is crucial, but so far, the work has mainly been focused on the evaluation of technical performance of the system and satisfaction of the user. According to DeChant et al. 46 this is the way that evaluation should be conducted for early prototypes. However, large scale clinical evaluation studies with multiple end points are needed before telemedicine services can be implemented routinely. 45 Such studies are scarce.
Notwithstanding the above, addressing these three elements does not guarantee successful
implementation. Other aspects that need to be considered are Financing, since satisfactory financial arrangements for telemedicine are
uncommon. Implementation, which is a staged process consisting of motivation or creating
awareness, learning and testing and after that real implementation. In each
phase of this process people withdraw so that only about two-thirds of the
professionals finally use the system.
55,56
Cooperation, since delivering a telemedicine service requires various
stakeholders with different backgrounds and not experienced with each other's
discipline to work together. New entities are probably needed to organize and
support this cooperation.
13
Generalisability, since telemedicine applications are often developed as
separate modules. Consequently they can only be used for a small group of
patients or for a small part of the treatment. Thus it is difficult to make any
single application financially viable. The technology. The technology will continue to develop, which will enable
applications that better fit the requirements of the users. It should also mean
that the technology behind the application becomes even more invisible, for
example by integration of sensors in clothes or in the surroundings. Concept of telemedicine. Patients with chronic diseases are often treated in
groups because they can learn from each other. However most of the telemedicine
applications developed to date focus on the treatment of individual patients.
Developing treatments that enable interaction with a group is one of the next
steps for telemedicine. It will also be important to develop applications that
incorporate gaming aspects into the applications with the aim of making
physical training more attractive and more fun. Requirements of the health-care professional. The requirements of the patient
are important, but so also are the requirements of the professionals. By using
telemedicine applications, health-care professionals are confronted with
enormous quantities of information about patients' health status, much more
than currently available from laboratory or face-to-face consultations.
Decision support systems are needed to process these data intelligently.
Telemedicine applications also need to be integrated to be able to better
support the clinicians in the so called care pathways. Health-care domains. The concept of remote monitoring and treatment for the
treatment of patients with chronic pain is expected to be applicable to a much
larger group of patients and health-care domains. For example, elderly people
who need to remain physically active or need to recover after an operation, or
overweight children who need to be motivated to become more active.
Besides this, other aspects that need to be considered in telemedicine
applications are related to:
In conclusion, telemedicine has great potential to make health-care more
effective, efficient and accessible. Although many pilot projects have failed in the
past, there is a growing awareness about the essential elements in design, development
and evaluation.
Footnotes
Acknowledgements
This work was undertaken with financial support from the EC (eTEN grant no. 046230).