
Abstract
We investigated the potential prognostic factors for clinically relevant improvements in pain intensity and pain-related disability after myofeedback-based teletreatment. Sixty-five female computer users, 56 female patients with whiplash-associated disorders and 18 female patients with non-specific neck and shoulder pain participated in the study. They received myofeedback-based teletreatment or usual treatment. Questionnaires concerning prognostic factors, pain and disability were completed before the start of the intervention (baseline) and at follow-ups at the end of the intervention, and after 3 and 6 months. Logistic regression analyses were performed in order to investigate prognostic factors for clinically relevant improvement. In the intervention group, improvement in pain intensity was predicted by baseline pain intensity. Baseline pain intensity and disability, and fear-avoidance and endurance related pain coping responses were prognostic factors for outcome in pain-related disability in this group. There were few differences between the intervention groups; fear-avoidance coping responses influenced the outcome after teletreatment only. Myofeedback-based teletreatment appears to be an useful telemedicine intervention, especially for participants with moderate to high levels of pain and disability, high perceived help/hopelessness, and those who tend to deal with their pain by avoiding social and physical activities.
Introduction
A randomized controlled study was performed to investigate the effects of a myofeedback-based teletreatment service intervention among female computer users, female patients with whiplash-associated disorders and female patients suffering from non-specific neck and shoulder pain. 1 The myofeedback-based teletreatment intervention is based on the Cinderella hypothesis, 2 which states that muscular pain may be caused by overuse of low threshold motor-units. 3 The treatment aims to promote muscular relaxation, allowing recovery of the low threshold motor-units, by signalling the patient when there is a lack of muscular relaxation according to a preset value. 4
An important feature of the myofeedback intervention is the fact that it is a telemedicine service. The remote monitoring and treatment are expected to increase treatment efficiency because one therapist can treat several patients simultaneously, and intramural care can be replaced by less costly extramural care. 5 Besides improving the efficiency, telemonitoring services should increase treatment effectiveness because treatment can be performed with much higher intensity and in the daily environment of the patient. Recent studies have shown some evidence for this. 5 For example, behavioural telehealth interventions have been found to be effective in the treatment of mental health problems, e.g. in providing psychotherapy. 6 Research suggests that interventions aiming at self-regulation training for chronic pain patients can be effectively delivered via telemedicine. 7 Also, a pilot study among female workers with neck and shoulder pain related to computer work indicated that remotely supervised myofeedback training is technically feasible and improves the clinical outcomes. 8
The main clinical results from the teletreatment study are reported in other papers in this special issue. 9,10 These studies showed reductions in pain and disability among people receiving myofeedback-based teletreatment, with similar improvement among people in the control group receiving treatment as usual. 9,10
It has been suggested that successful treatment of musculoskeletal pain depends on identifying the patient at the right time and providing the right intervention 11–13 or, in other words, that a certain intervention will be more beneficial within a subgroup of patients defined by certain characteristics. The aim of the present study was to identify prognostic factors, in order to be able to answer the question ‘who is likely to benefit from receiving myofeedback-based teletreatment for neck and shoulder pain?’
Previous studies of primary care patients have found prior pain intensity and duration, pain-related disability, pain coping strategies, pain-related fear of movement and a depressed mood to predict clinical outcome among patients suffering from upper extremity disorders and whiplash-associated disorders. 14–20 However, few studies have investigated prognostic factors for outcome after myofeedback training, and, to the best of our knowledge, no studies on prognostic factors for outcome after remotely supervised myofeedback training have been reported in the literature. Results from a recent randomized controlled study among female computer users suggest that myofeedback training (not including the teletreatment component) in combination with ergonomics counselling is beneficial in employees with moderate levels of pain intensity and pain-related disability. 21 More specifically, baseline pain intensity, diagnosis localized to muscle (rather than other structures) and stress-induced lack of muscle relaxation were found to be prognostic factors for clinically relevant improvements in pain intensity. 21 Pain-related disability was predicted mainly by baseline pain and pain-related disability and passive coping. 21
In accordance with the literature, we hypothesized that baseline levels of pain and disability, and a depressed mood will be predictive of outcome in both pain intensity and pain-related disability, in the remote myofeedback group as well as the control group. In addition, as fear avoidance and endurance related coping responses have been found to play a role in the maintenance of chronic pain 22–24 these factors might also play a role in the diminishing of pain and disability as a result of interventions. Research on technology acceptance in telemedicine suggests that patient characteristics like gender and age are related to technology acceptance and to the intention to use technology. 25–27 Based on this we expect that these factors may also be related to outcome after the myofeedback intervention.
Methods
A randomized controlled trial was performed assessing the effects of myofeedback-based teletreatment compared with usual treatment. 9,10 Three different groups of participants were included. The first study sample consisted of female employees performing predominantly computer work. 9 The second study sample consisted of female patients suffering from grade II or III whiplash-associated disorders, and the third study sample consisted of female pain patients suffering from chronic non-specific neck and shoulder pain. 10
The present study investigated prognostic factors for treatment effects in the myofeedback-based teletreatment service. Analyses were also performed within the control intervention in order to be able to elucidate whether the prognostic factors identified in the teletreatment intervention were specific to this intervention, or were generic factors that influenced the effect of treatment in general.
Measurements concerning prognostic factors, pain, and disability were completed before the start of the intervention (baseline) and at follow-ups immediately after the end of the intervention (T0) and after 3 (T3) and 6 (T6) months.
Participants
In all, 139 participants were included in the present study. Half of these received remotely supervised myofeedback training (33 computer workers, 27 whiplash disorder patients, 10 non-specific pain patients), and the other half were included in the control intervention (32 computer workers, 29 whiplash disorder patients, 8 non-specific pain patients). During the intervention 27 participants dropped out of the study (18 intervention and 9 control), at 3-month follow-up, 30 additional dropouts had occurred (12 intervention and 18 control), and at 6-month follow-up, 21 additional dropouts had occurred (10 intervention and 11 control). All participants were female with a mean age of about 42 years. Analyses investigating prognostic factors are based on the subjects who responded in both baseline and follow-up measurements, i.e. in the intervention group n = 52 for analyses focusing on T0, n = 40 for analyses focusing on T3 and n = 30 for analyses focusing on T6, and in the control group n = 60 for analyses focusing on T0, n = 42 for analyses focusing on T3 and n = 31 for analyses focusing on T6.
Intervention
The telemedicine service consisted of a mobile health-care application using surface electromyography (sEMG) of the trapezius muscle. The myofeedback system consists of a garment with dry sEMG electrodes, and a vibration unit that provides tactile feedback (a vibration that alerts the participant of insufficient muscle rest) as well as a personal digital assistant (PDA) providing visual feedback about muscle activation and relaxation. This system is worn by the participant under her usual clothes during her daily activities (e.g. at home or at work). From the PDA, the muscle activity data are sent to a web-based portal via a wireless connection. The therapist (physiotherapist, psychologist or occupational therapist) has access to this portal and can examine the muscle activity data.
Participants in the intervention group took part in 4 weeks of remotely supervised myofeedback training. The participants were asked to wear the system as much as possible; 8 hours distributed over at least 2 days a week was considered a minimum. During the first meeting (face-to-face) with the therapist, each participant was taught how to operate the myofeedback system and shown possible reasons for an alarm being activated (e.g. the muscles of the neck and shoulder were not relaxed enough). They were also given instructions on how to relax and achieve muscle rest. During the intervention period remote (telephone and/or email) consultations took place at least once per week. Essential information in these consultations was the diary provided by the participant and the EMG data which was available at the server.
From an ethical perspective it was considered unacceptable to ask participants to discontinue any on-going treatment aimed at alleviating pain or symptoms in order to take part in the intervention. Instead, information on additional treatment being received when entering the study was recorded at baseline by means of questionnaire items covering the use of analgesics, physiotherapy, acupuncture and different kinds of physical training. At baseline, 67% of the participants in the intervention group reported receiving additional treatment, most commonly consisting of pain-killers (44%), physiotherapy (41%) and other unspecified measures (21%). For additional information, see Sandsjö et al. 9 and Kosterink et al. 10
Control
Participants in the control group did not receive any intervention, but continued their conventional care practice (if any). Information about conventional treatment and/or medication received for neck and shoulder pain during the control period was recorded by means of questionnaires. At baseline, 61% of the participants in the control group reported receiving treatment for their neck and shoulder pain, most commonly consisting of pain-killers (33%), other measures (28%), physiotherapy (25%) and relaxation training (20%). For additional information see Sandsjö et al. 9 and Kosterink et al. 10
Measures
Self-reported pain intensity (ache, pain) in the neck and shoulder region was assessed using a Visual Analogue Scale (VAS). 28 Participants were instructed to indicate the average level of ache or pain experienced during the previous week, using a 10 cm horizontal line with ‘no discomfort at all’ and ‘as much discomfort as possible’ at the endpoints. A cut-off point for clinically relevant improvement was set as ≥13 mm change in the VAS score. 29–31
Self-reported pain-related disability was assessed using the Pain Disability Index (PDI) 32 (α = 0.92) that measures the impact of pain on the ability to participate in different activities. This index contains seven items, for family and home responsibilities, recreation, social activity, occupation, sexual behaviour, self-care and life-supporting activities. For each item there are 11 fixed response alternatives ranging from ‘not disabled’ (0) to ‘fully disabled’ (10). The variable pain-related disability was constructed by deriving the mean score for these seven items, with high values indicating a high level of disability. A cut-off point for clinically relevant improvement was set as 10% of the maximum total (mean) score, 31 i.e. ≥1 unit of change on the mean PDI score.
Fear-avoidance and endurance related coping responses to pain were assessed using the Avoidance-Endurance Questionnaire (AEQ). 23 Cognitive fear-avoidance related responses were assessed using the factors catastrophizing thoughts (3 items, α = 0.90) and help-hopelessness (9 items, α = 0.92). Cognitive endurance related responses were assessed using the factor thought suppression (4 items, α = 0.78). Affective fear-avoidance related responses were assessed using the factors anxiety/depression (7 items, α = 0.91) and affective endurance related responses were assessed using the factor positive mood despite pain (3 items, α = 0.90). Fear-avoidance related behavioural responses were assessed using the factors avoidance of social activities mild pain (6 items, α = 0.89) and severe pain (6 items, α = 0.93) and avoidance of physical activities mild pain (5 items, α = 0.80) and severe pain (5 items, α = 0.82), and endurance related behavioural responses were assessed using the factor behavioural endurance mild pain (12 items, α = 0.70) and severe pain (12 items, α = 0.69). Each of these items had 7 fixed response alternatives on a scale 0–6. These coping variables were constructed by deriving the mean values for the items within the respective factor, with high mean values indicating high values for the respective coping response.
Depressive symptoms were assessed using the Beck Depression Inventory (BDI-II), 33 which is a self-report measure where the respondents for different symptoms (e.g. sadness, pessimism, energy, sleep) are asked to choose among a number of fixed response alternatives the one that best describes how they have been feeling during the previous two weeks. The variable depressive symptoms (21 items, α = 0.90) was constructed by deriving the mean value for these items, with a high mean value indicating a high level of depressive symptoms.
Statistical analysis
In order to investigate potential prognostic factors for outcome (clinically relevant improvement yes/no) in pain intensity and pain-related disability, univariate logistic regression analyses were performed using a standard package (SPSS version 16). In addition, multiple logistic regression analyses were performed in order to investigate the proportion of explained variance for a model for each outcome variable (improvement in pain at T0, T3 and T6, and improvement in disability at T0, T3 and T6) including all the independent variables significant in univariate analyses. Percentage of explained variance was assessed using the McFadden pseudo R2. 34 Differences between the myofeedback and control interventions in baseline exposure to potential prognostic factors were investigated using t-tests. Differences in logistic regression coefficients between the myofeedback and control interventions were investigated using the test for investigating group differences in logistic regression models described by DeMaris. 35
Results
Among the subjects receiving teletreatment, 19 participants (37%) showed clinically relevant improvement in pain intensity at T0, 17 participants (43%) had improved at T3, and 15 participants (50%) had improved at T6. For pain-related disability, 16 participants (31%) showed clinically relevant improvement at T0, 9 participants (23%) had improved at T3 and 13 participants (43%) had improved at T6. The percentages in improvement were not significantly different in the control intervention (for pain intensity 43% at T0, 33% at T0, 45% at T6, and for disability 23% at T0, 29% at T3, 36% at T6).
Baseline levels of the potential prognostic factors in the myofeedback and control interventions are summarised in Table 1. Catastrophizing thoughts at baseline were higher in the control group (mean 0.86, SD = 1.23) than in the intervention group (mean 0.40, SD = 0.78). No other differences in baseline values for the potential prognostic factors were found between the interventions.
Baseline levels of potential prognostic factors in the myofeedback (n = 70), and control interventions (n = 69). For the coping strategies ‘M’ denotes mild pain and ‘S’ denotes severe pain
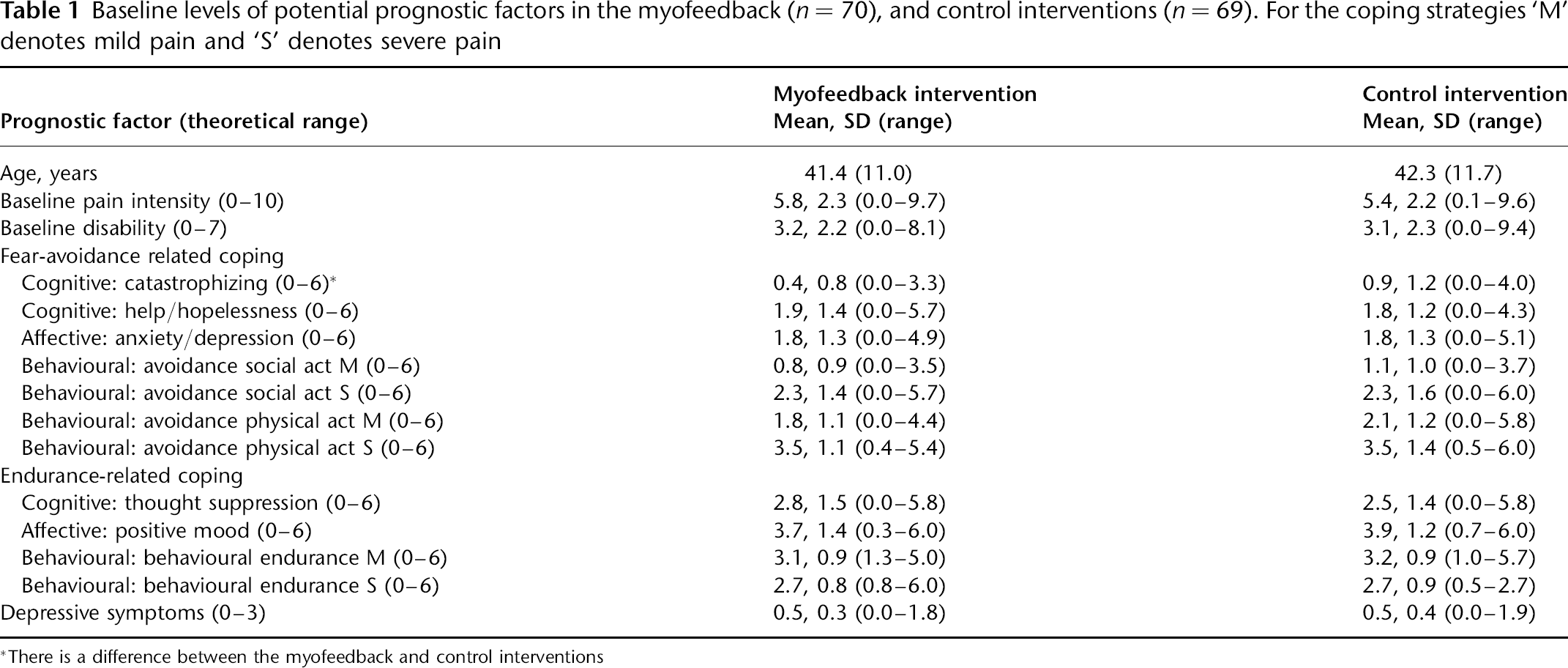
*There is a difference between the myofeedback and control interventions
Prognostic factors for improvement in pain intensity
The results from crude univariate logistic regression analyses investigating potential prognostic factors for outcome in pain intensity are summarised in Table 2. For participants in the intervention group, baseline pain intensity was related to clinically relevant improvement in pain intensity at short-term (T3, but not T0) and long-term (T6) follow-up, such that the higher the baseline pain intensity the higher the odds for improvement (for T3 OR = 1.73, 95% CI 1.20, 2.49, and for T6 OR = 1.64, 95% CI 1.12, 2.39). None of the other proposed prognostic factors significantly influenced the odds for clinically relevant improvement in pain intensity after teletreatment. The percentage of pseudo-variance explained for a model including baseline pain intensity was about 21% at T3 and 22% at T6.
Myofeedback intervention. Crude bivariate odds ratios (OR) with 95% confidence intervals (CI) for clinically relevant improvement in pain intensity between baseline (before the start of the intervention) and T0 (directly after four weeks of intervention) (n = 52), between baseline and T3 (three months after the end of the intervention) (n = 40), and between baseline and T6 (six months after the end of the intervention) (n = 30). Significant ORs are marked in boldface. For the coping strategies ‘M’ denotes mild pain and ‘S’ denotes severe pain
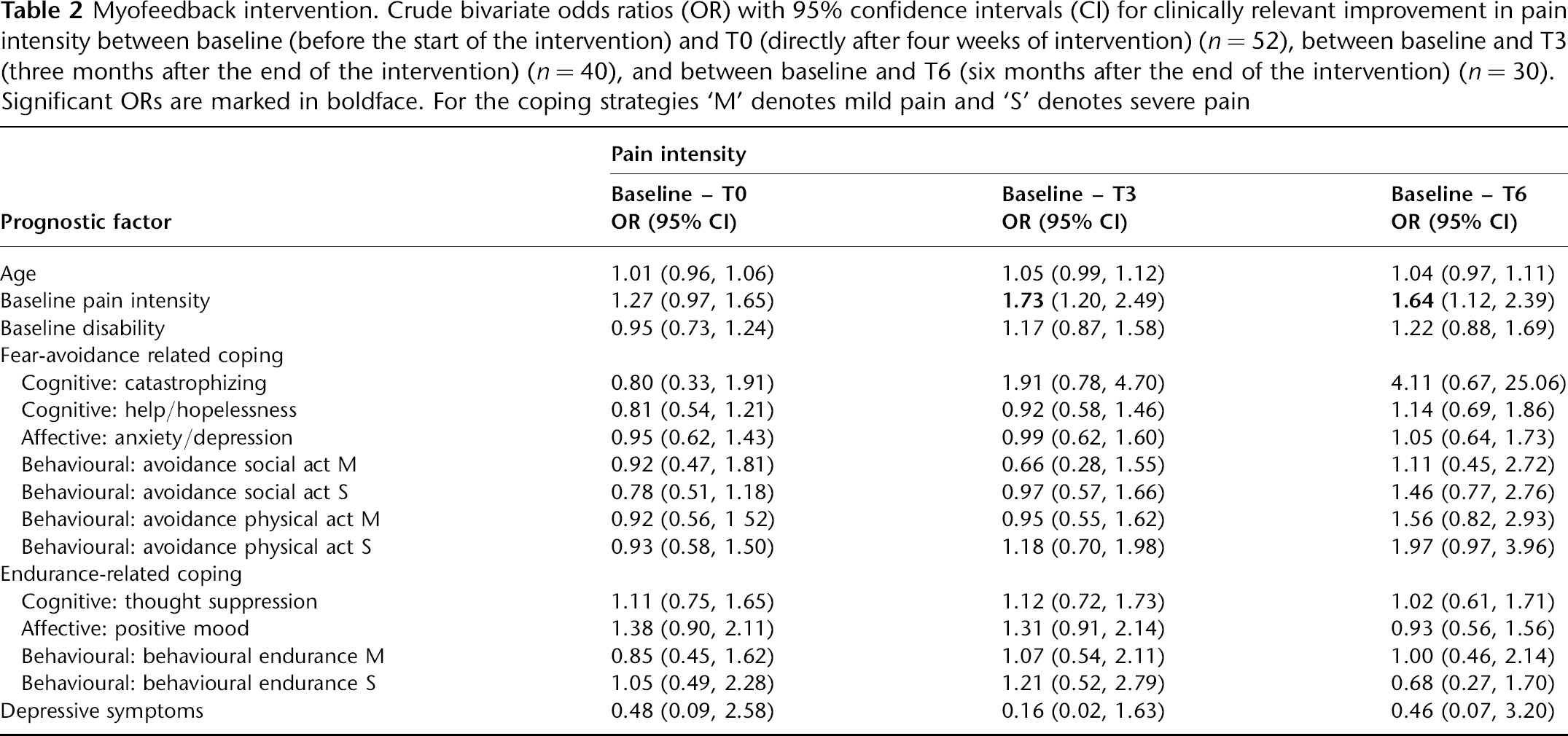
The only prognostic factor found for improvement in pain intensity for participants in the control group was catastrophizing thoughts, with participants reporting a high amount of catastrophizing thoughts showing larger odds for improvement at long-term (T6) follow-up (OR = 3.04 95% CI: 1.03, 9.00).
Prognostic factors for improvement in pain-related disability
Results from crude univariate logistic regression analyses investigating potential prognostic factors for outcome in pain-related disability after teletreatment are summarised in Table 3. In the intervention group, baseline pain intensity was related to clinically relevant improvement in disability at short-term (T0 but not T3) and long-term (T6) follow-ups, such that the higher the pain intensity at baseline the higher the odds for improvement (for T0 OR = 1.53, 95% CI 1.10, 2.12, and for T6 OR = 1.44, 95% CI 1.03, 2.02). Similar effects were found for baseline pain-related disability, with higher baseline disability being related to higher odds for improvement at both short-term (T0 but not T3) and long-term (T6) follow-ups (for T0 OR = 1.90, 95% CI 1.27, 2.86, and for T6 OR = 1.59, 95% CI 1.08, 2.35). Aspects of fear-avoidance related and endurance related coping were related to clinically relevant improvement in disability at short-term (T3) follow-up. Participants with higher perceived help/hopelessness showed higher odds for improvement (OR = 1.75, 95% CI 1.00, 3.05), and participants with higher positive mood despite pain showed lower odds for improvement (OR = 0.52, 95% CI 0.28, 0.97) after the telemedicine intervention. Fear-avoidance related coping also influenced the odds for improvement at long-term follow-up (T6), with participants scoring high on avoidance of social and physical activities showing higher odds for improvement (avoidance of social activities; mild pain OR = 4.83, 95% CI 1.20, 19.41, avoidance of social activities; severe pain OR = 3.34, 95% CI 1.37, 8.82, avoidance of physical activities; mild pain OR = 2.47, 95% CI 1.15, 5.31). The percentage of pseudo variance explained for the models including the significant prognostic factors found in the univariate analyses at each follow-up (baseline pain intensity and disability at T0, help/hopelessness and positive mood at T3, baseline pain and disability, avoidance of social and physical activities at T6) was about 24% at T0, about 15% at T3, and about 29% at T6.
Myofeedback intervention. Crude bivariate odds ratios (OR) with 95% confidence intervals (CI) for clinically relevant improvement in pain-related disability between baseline (before the start of the intervention) and T0 (directly after four weeks of intervention) (n = 52), between baseline and T3 (three months after the end of the intervention) (n = 40), and between baseline and T6 (six months after the end of the intervention) (n = 30). Significant ORs are marked in boldface. For the coping strategies ‘M’ denotes mild pain and ‘S’ denotes severe pain
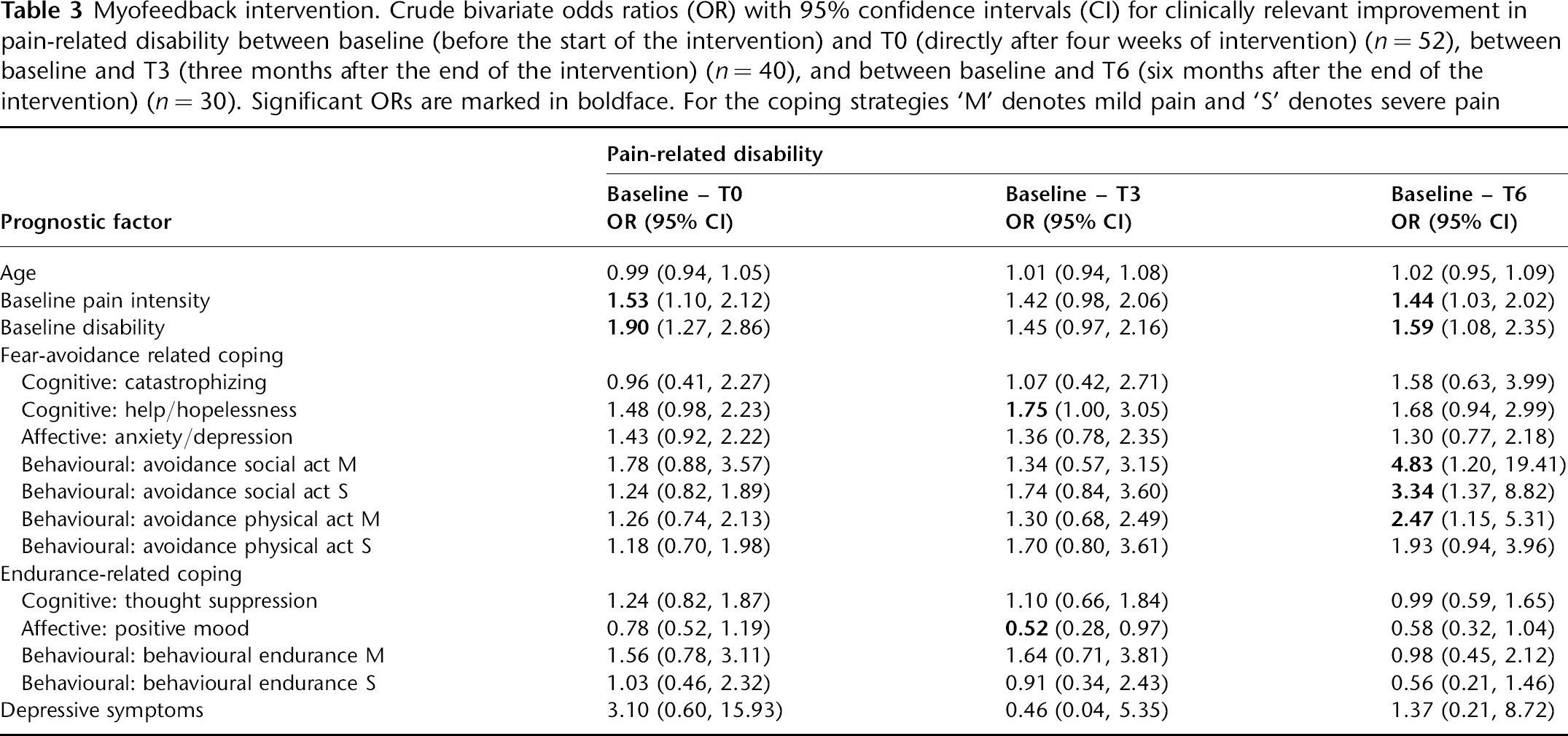
In the control group baseline pain-related disability was related to clinically relevant improvement in disability at short term (T0 and T3) and long term follow-ups, with participants with higher levels of disability showing larger odds for improvement (for T0 OR = 1.54, 95% CI 1.14, 2.09, for T3 OR = 1.47, 95% CI 1.07, 2.03, and for T6 OR = 1.62, 95% CI 1.09, 2.40). Behavioural endurance was related to improvement in disability at T3 follow-up, such that participants with higher scores on behavioural endurance (mild pain) showed lower odds for improvement.
Discussion
The aim of the present study was to identify factors that influence the effects of the teletreatment service, in order to identify patients who are likely to benefit by using this treatment for their neck and shoulder pain. A previous study of prognostic factors for myofeedback treatment (not including the telemedicine component) effects among female computer users found participants with moderate to high levels of pain intensity at baseline to benefit more from the intervention than participants with low baseline pain. 21,36 Similar results were found in the present study, where moderate to high baseline pain was predictive of a positive outcome in pain, and moderate to high levels of baseline pain and disability were predictive of a positive outcome in disability.
Previous research indicates that passive coping is associated with higher pain severity and disability, while active coping (e.g. pain control and diverting attention) seems to be associated with less disability. 37–39 A passive coping style has been found to be related to slower or less complete recovery in patients with whiplash-associated disorders. 15 We have previously noted that participants with work-related neck and shoulder pain who use passive coping to deal with their symptoms benefit more from myofeedback in combination with ergonomics counselling in terms of reduced disability than other participants, both at short- and long-term follow-ups. 21 In the present study, the focus was on fear-avoidance related and endurance related pain coping responses, rather than on passive and active coping. The reason for this is the fact that fear avoidance and endurance related coping have been found to play a role in the maintenance of chronic pain, 22–23 and therefore might also play a role in the diminishing of pain and pain-related disability.
High endurance coping can be indicative of a muscle overuse that leads to chronic pain via overload of physical structures. 24 We therefore hypothesized that an intervention aiming to reduce physical overload would be most effective in reducing pain symptoms in patients showing moderate to high endurance responses. High endurance coping responses at baseline were expected to predict a positive outcome in pain symptoms after the teletreatment because participants who overuse damaged muscles would be made aware of this overuse and its potential consequences during the myofeedback training. We further hypothesized that pain symptoms in the intervention group would be most effectively reduced in patients showing moderate to high baseline fear-avoidance. In contrast, in a control group that did not receive specific muscular training, we hypothesized that high endurance and high fear-avoidance related coping responses at baseline would be associated with lower odds for improvement after the intervention.
The hypotheses that endurance coping responses would serve as prognostic factors for outcome in pain intensity were not supported in the present study. High endurance coping did however serve as a prognostic factor for improvement in disability for both interventions. For the intervention group, positive mood despite pain (an aspect of endurance coping) was related to outcome in disability, with participants with a high initial positive mood despite pain at baseline showing lower odds for improvement after the intervention. This seems to be a specific prognostic factor, since it did not influence outcome in the control group (the difference between the interventions was significant (P < 0.05). For the control intervention, on the other hand, a high behavioural endurance (another aspect of endurance coping) was related to outcome in disability, such that participants with high behavioural endurance showed lower odds for improvement.
The hypothesis that fear-avoidance coping responses would influence outcome in pain-related disability after remotely supervised myofeedback training was supported since aspects of this coping response pattern (help/hopelessness, avoidance of social and physical activities) served as prognostic factors for the intervention effects on disability in the present study. Participants who reported high levels of help/hopelessness and who tended to avoid social and physical activities showed higher odds for improvement than participants who scored low on these coping responses. In promoting active coping strategies (changing the environment and changing the behaviour) the intervention has a focus on reducing feelings of help/hopelessness, and of decreasing avoidant behaviour. After the four weeks of teletreatment, feelings of help/hopelessness had significantly decreased (P < 0.01). Avoidance of social activities (severe pain) and avoidance of physical activities (severe pain) had also significantly decreased (P < 0.05 and P < 0.05, respectively). It is therefore possible that participants high on fear-avoidance related coping benefited more from the teletreatment because their fear-avoidance beliefs and behaviour were reduced during the intervention. These aspects of fear-avoidance related coping were not related to improvement in the control intervention, and therefore seem to be treatment-specific rather than generic prognostic factors. It should however be noted that the differences between the intervention and control treatment for these aspects were significant only for the factor avoidance of social activities (for mild pain P < 0.05 and for severe pain P < 0.05), and not for help/hopelessness (P < 0.10) or avoidance of physical activities (severe pain) (P < 0.10). In teletreatment in general, feedback has the function of making participants aware of their health status and motivating them to take action to improve their health. 40 It is possible that the continuous and intense monitoring and feedback provided by the myofeedback-based teletreatment service lead to increased motivation and perceived self-control, which, in turn, can diminish fear-avoidance beliefs when participants successfully become more physically active (without decreased muscle relaxation) during the course of the intervention.
A recent review of prognostic factors for neck pain in whiplash-associated disorders found depressed mood to be associated with a slower or less complete recovery. 15 In the present study however, depressive symptoms did not seem to influence the effect of myofeedback-based teletreatment, i.e. this intervention seems to be equally efficient among participants with low and moderate levels of depressive symptoms. The level of depressive symptoms was however rather low in the present study, meaning that the potential effect of high levels of depression on intervention effect could not be investigated.
Research on technology acceptance in telemedicine suggests that factors such as gender and age may be related to technology acceptance, 25–27,41 and that they may influence outcome after the myofeedback teletreatment. Gender effects could not be evaluated in the present study since the sample consisted only of women. The results did not show an age effect on outcome after the intervention. However, the age range in the present study may have been too small to detect potential age effects, although another explanation may be that the equipment was easy to use 42 and did not constitute a barrier for elderly people.
In summary, the only prognostic factor found in the present study for myofeedback-based teletreatment effects on pain intensity was pain intensity at baseline. For the myofeedback-based teletreatment effect on disability, also baseline disability and a few of the pain coping strategies served as prognostic factors. The amounts of explained variance however were fairly low (15–29%), which suggests the omission of important prognostic factors. The remotely supervised myofeedback training intervention is based on the theory that introduction of periods of muscular relaxation reduces the risk of cell damage, and, in the long run, development of chronic pain, by increasing the opportunities for recovery of low threshold motor units. 4 Consequently, participants with pain syndromes located in muscle rather than other structures (i.e. with the clinical diagnoses of tension neck syndrome, cervicalgia or trapezius myalgia) would be expected to respond better to myofeedback treatment than subjects with other diagnoses. 21 From this, theoretical basis for the myofeedback training also follows the hypothesis that participants with a low amount of muscle rest at baseline will benefit more from the intervention than those with a high amount of muscle rest, since for these participants there is a need for increased muscle rest. 21 These hypotheses were supported in a previous study of prognostic factors for myofeedback intervention effects where it was found that participants with diagnosis localized to muscle, and with stress-induced lack of muscular relaxation benefited more from the intervention. The omission of these potential prognostic factors must therefore be acknowledged as a weakness in the present study.
It has been suggested that psychosocial work-related factors such as employer reactions and inadequate co-worker support may affect treatment results in back pain. 11 Also in technology acceptance models, social influence processes are considered important in relation to the intention to use technology applications. 43 Such processes might also be important to consider when studying factors influencing the effect of remotely supervised myofeedback training in the workplace, e.g. it may be difficult to introduce workstation modifications or to respond to myofeedback alarms by taking short breaks when the workload is too high, and when managers and co-workers do not support these changes. 21
Conclusions
The results of the present study suggest that myofeedback-based teletreatment is an useful intervention especially for participants with moderate to high levels of pain, high perceived help/hopelessness, or those who tend to deal with their pain by avoiding social and physical activities. The sample size of the present study was fairly small, and only fairly small amounts of the variance in clinically relevant improvement in pain intensity and pain-related disability could be explained by the prognostic factors investigated.
Footnotes
Acknowledgements
This work was undertaken with financial support from the EC (grant eTEN, no. 046230). We thank Tom Barbe, Christer Knutsson and Tobias Marecek for their contributions. Dr Larsman was supported by a grant from the Swedish Council for Working Life and Social Research. The Swedish Council also supported the Swedish participation.