
Abstract
We studied the effect of telephone-linked computer (TLC) communication in patients being treated with home enteral nutrition. A total of 290 patients were enrolled in the study which compared two groups of patients who were recruited at different times (control: 193, TLC: 97). At baseline there were no significant differences in characteristics or clinical practice between the two groups. Over a three-month period, 823 automatic telephone calls were dialled out to the TLC patients and in 787 of the calls (96%) there were complete responses to all questions. A total of 205 alert messages were generated for the 823 calls. Less than 10% were false alerts. All health outcome measures, the EQ-5D and three components of the SF-36 improved slightly with time in both groups, but there was no significant difference between the groups. The patients' body mass index increased slightly in both groups, but the change was not significant. Home enteral nutrition prevented weight loss and improved some components of the QOL scores. The TLC system detected a high number of abnormal nutritional symptoms.
Introduction
Home enteral nutrition has been used for almost 20 years. Side-effects are frequent at the beginning, but vary widely from one centre to another. 1,2 Regular clinical assessment is needed in order to prevent undesirable symptoms and to avoid inappropriate behaviours from the patient. Therefore procedures for data collection, analysis and providing responses need to be systematic and efficient.
Telephone-linked computer (TLC) communication has been developed to support communication between caregivers and patients with various diseases. However, TLC has not been used in home enteral nutrition. 3 The purpose of the present study was to assess the effect of TLC on the symptoms, quality of life (QOL) and bodyweight of patients.
Methods
A comparative prospective study was conducted. In the first period, from 2002 to 2005, 200 patients formed a control group. In the second period, from 2005 to 2008, 97 patients formed an intervention group.
Patients and health-care providers
Any adult patients starting home enteral nutrition with the Nestle Home Care service were eligible. The inclusion criteria were: informed consent from the patient, or from the family if the patient was unable to use a touch-tone telephone. The exclusion criteria were: planned re-admission at a hospital within one month, impossible to follow up or a refusal.
Physicians' investigators enrolled the patients. All dieticians were specially trained in home enteral nutrition and worked for Nestle networks. Patients received an educational programme at discharge and at home about the enteral nutrition.
TLC system
After the patient was registered they were given a personal PIN code. A computer automated telephone call then asked the patient a set of questions about key nutritional symptoms. Patients answered by pressing the touch-tone keys on their telephone. Six multiple choice questions were asked twice a week during the first month and then weekly for two months (Appendix 1). After the call, the results could be assessed immediately on a website by the physicians and dieticians in charge of the patient. Messages could be sent by the patient to the TLC system with a toll free number if they expected not to be present at the time of the call or if they had a change in symptoms. The patients were asked to call a 24-hour emergency number in case of emergencies, in case of loss or clogging of the feeding tube or hyperthermia with abdominal pain.
Alert and interventions procedures
In the intervention group, preset thresholds were determined by a panel of experts. Symptoms that met a preset threshold for severity generated an email notification of the patient's symptom pattern to the physician and care-givers (Appendix 2). The dietician had to decide the appropriate response to any alert: a telephone advice call, a home visit or a medical advice.
Home visit
A 24-hour ‘hot line’ was available to both groups of patients. The dietician's first systematic visit was done on day 1 and then subsequently in months 1 and 3.
Ethics
The system used a password and PIN code with no patient's name being stored. Consequently, the agreement of the national informatics council (CNIL) was not required. The study was approved by the appropriate ethics committee.
Outcome measures
The primary outcome measure was an expected improvement of 10% in one component of the SF-36 health status survey 4 or a 10% improvement of the EQ-5D version of the Euro QOL instrument. 5 The estimated number of patients to treat was 97 in the intervention group. In addition, patients were asked about house, social, professional and sexual activities, their relation with their surroundings, their physical and psychological wellbeing, and the role of home enteral nutrition. These items were also analysed at 1 and 3 months. In addition, they were asked to give their opinions about home enteral nutrition and the TLC system.
Opinion survey
On the third month, or as soon as a patient abandoned the study protocol, a multiple choice questionnaire was completed about satisfaction with TLC and nutrition. Four months after the end of the study, home-care providers completed a multiple choice questionnaire about satisfaction with the TLC system.
Statistical analysis
Statistical analysis was performed with standard software (SAS 8.2, SAS Institute, NC, USA).
Results
Five French university hospitals participated and each centre had similar numbers of patients. The general and nutritional characteristics and associated therapies are summarised in Tables 1 and 2. The two populations were similar for all variables. Causes of disruption and complications are summarized in Table 3 and patient disposition in Figure 1.
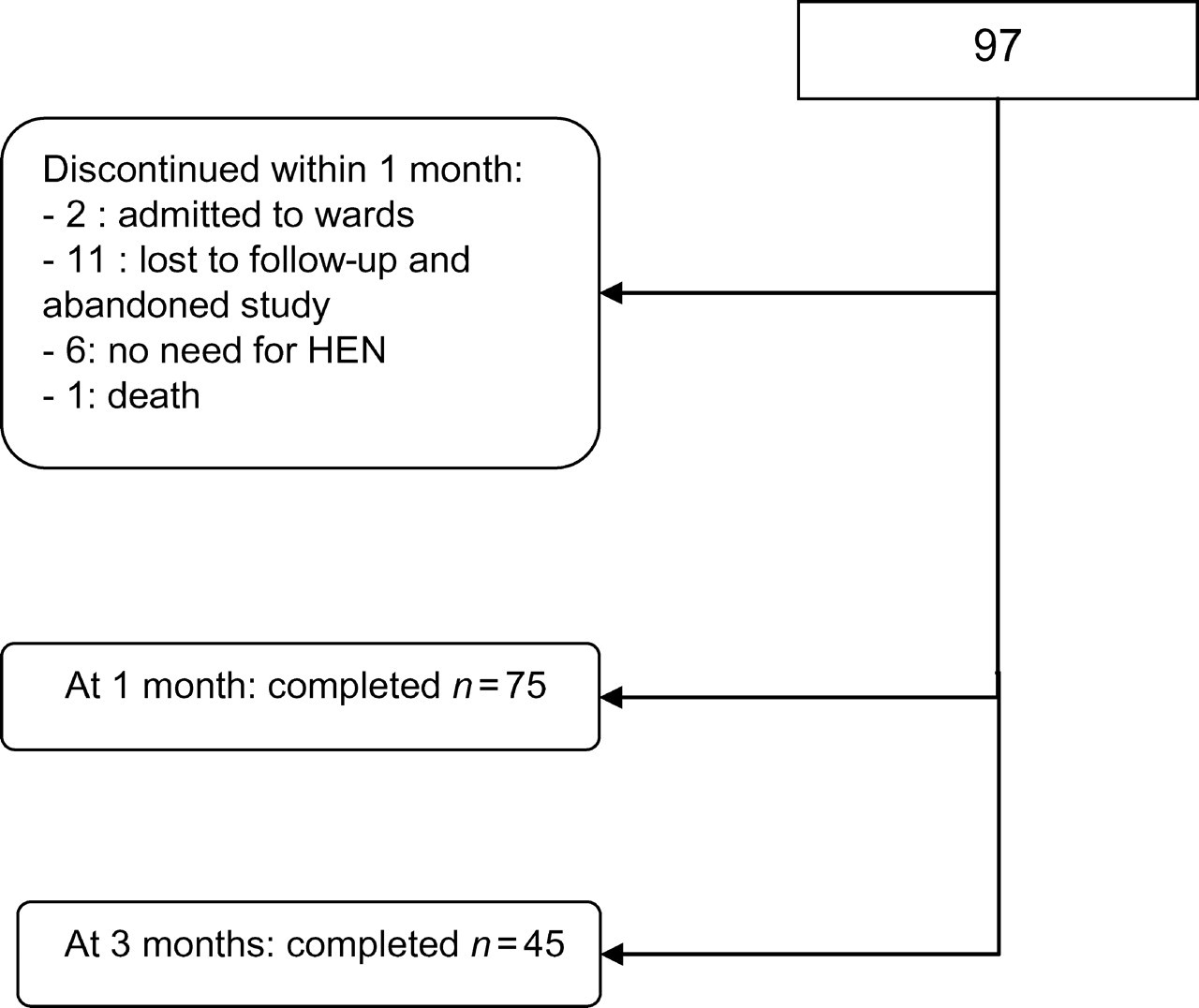
Disposition of the patients
Characteristics of the patients. There were no significant differences between the groups (P ≥ 0.05)
Enteral nutrition characteristics. There were no significant differences between the groups (P ≥ 0.05)
Nutritional and general complications. Percentage of patients with complications
*P < 0.05 between both groups
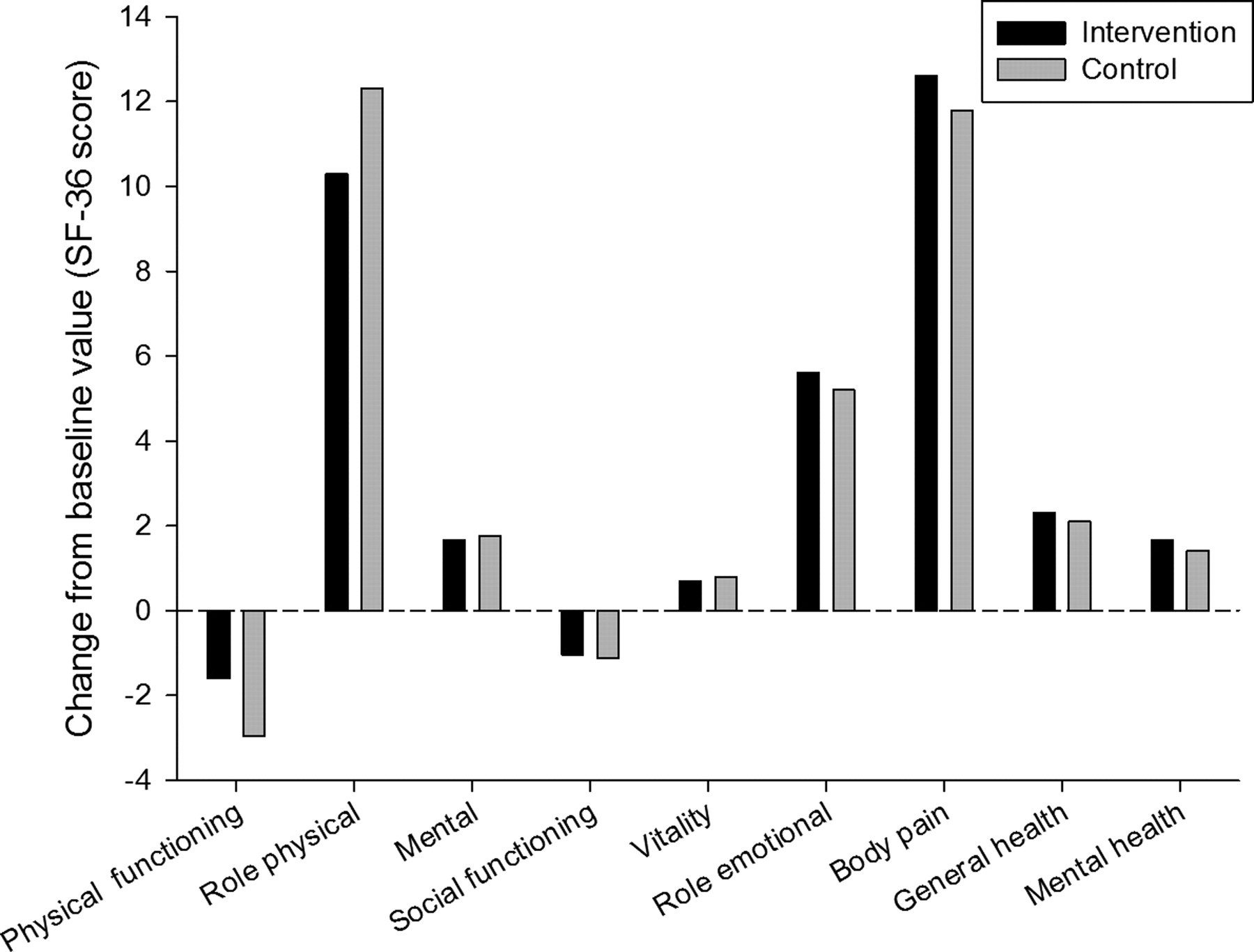
All health outcome measures, the EQ-5D (Table 4) and three components of the SF-36 (Table 5 and Figures 2 and 3) slightly improved with time in both groups, but there was no significant difference between the groups. The house, social, professional and sexual activities, relation with surroundings, and physical and psychological wellbeing did not differ between the groups.
Changes in the SF-36 scores from baseline values at 1 month

Changes in the SF-36 scores from baseline values at 3 months
Mean values (SD) of the EQ-5D index in the two groups
Mean baseline values for SF-36 in the two groups
The patients' body mass index slightly increased in both groups, but the change was not significant. In the TLC group the mean values were 19.8 kg/m2 (SD 4.2) at inclusion, 20.3 kg/m2 (SD 3.7) in the first month and 20.1 kg/m2 (SD 2.2) in the third month. There was no difference between the groups at 1 and 3 months (P > 0.05).
Automated calls and responses
A total of 823 automatic telephone calls were dialled out to patients and 787 patients completed the responses to all questions (96%). After one month, 75% of the patients had answered the telephone calls and 87% of the calls had responses. Fifty percent of the patients had answered calls in the second month but only 17% by the end of the study.
Alerts
A total of 205 alert messages were generated for the 823 automatic calls. Only 16 were wrong answers, mainly because of mistakes in the touch-tone phone numbers, i.e. there were 189 real alerts (23% of the total answered calls). A hundred alert messages were identified when the repetition of the alert in consecutive calls was taken into account. Sixty-three percent of the patients experienced at least one symptom that was severe enough to generate a symptom-alert email message. A summary of the real alerts is shown in Table 6 and a summary of the types of alert in Table 7.
Percentage of alert messages in the answered calls (n = 787)
Number of calls for each type of alert
One third of the patients had vomiting (versus 3% in control) and 13% had diarrhoea (versus 3%). Diarrhoea was more frequent in patients with digestive diseases, chemotherapy and jejunostomy (P = 0.005, P = 0.012, P = 0.012, respectively). Eighteen percent had abdominal pain at least once or discomfort related to the feeding tube, especially in ENT or oesophageal cancers (P < 0.05). Eighteen percent of the patients experienced a feeding tube clogging. Six tube exchanges were needed in the control group (five nasogastric and one percutaneous endoscopic gastrostomy) versus one in the intervention group (P > 0.05). Thirty-two percent of the patients generated at least one nutrition bag intake alert when diarrhoea (P = 0.036), pain (P < 0.001), tube clogging (P = 0.02) occurred or when chemotherapy was administered (P > 0.05).
Responses to alerts occurred in less than 48 hours for all alerts except for one (persistent nausea). Seventy percent of the patients received advice by telephone and 8% had a home visit from the dietician. The complications are summarised in Table 3 and Figure 1 shows the causes of discontinued study in the group.
Opinion survey
The opinion survey found a high degree of user satisfaction. Only 4% of the patients reported that nutrition and the TLC system was not beneficial. However, those who abandoned the study were not questioned. On an analogue scale from 0 to 10, home-care providers reported an average satisfaction of 7.8 (SD 0.8) in using the system.
Discussion
The aim of the study was to assess prospectively the effect of close automatic follow-up of home enteral nutrition on QOL, symptoms and weight. We did not conduct a randomized controlled trial, and this may weaken the conclusions that can be drawn. Between 2002 and 2005 the impact of enteral nutrition on the QOL was measured. The TLC system was implemented between 2005 and 2008 in order to improve the efficiency of home enteral nutrition. There were no significant differences for clinical practice between the populations studied (Tables 1 and 2). We did not change the nutritional device, products or materials. This suggests that there is a weak probability of confounding factors during the six-year study period.
Telemedicine has been employed successfully in various chronic diseases, but not in home enteral nutrition. 6,7 Our data provide objective incidence and symptom quantification using a numerical scale. The TLC system detected high numbers of side effects, perhaps because the patients were questioned frequently.
Because of early detection and rapid responses, most of the alert-symptoms did not last for more than two consecutive telephone calls. TLC was associated with decreased nausea and vomiting, pneumonia, and tube exchange by clogging or migration, although the differences were not significant (Table 3).
Education of the patient plays a major role in home enteral nutrition. For example, most of the patients did not reduce nutrition flow, but simply stopped the administration when symptoms occurred. A teaching programme was conducted at discharge in the institution and at home with the dieticians. This programme included general information about nutrition, the nutritional device and how to cope with a problem. However, it was not standardized among the institutions and the patient feedback was not assessed.
In the first part of our study (i.e. the control group) implementing home enteral nutrition stabilized weight and improved some components of the QOL scores, at least moderately. In the second part (i.e. the intervention group) adding the TLC system improved early management of nutrition related symptoms, but did not significantly improve QOL. The results showed that few patients linked incidents to the nutrition bags, but rather to other therapies (chemotherapy, radiation therapy, pain killers and antibiotics). Also, a high satisfaction and feeling of security were associated with home enteral nutrition. However, the feeding tube represents a strong negative component of QOL and one-third of the patients had pain or were embarrassed by it. In addition, chemotherapy and radiation therapy severely altered speech, eating, pain and physical function, which are major components of the patients' QOL. 8,9 Our study shows that the early detection and management of the side-effects of nutrition are feasible, but this seems to have only a minor role in health outcomes.
In some studies, patients who benefited from home enteral nutrition had long term neurological disease. 10,11 Our population faced cancers that were mostly more life threatening. The body image is changed and the capabilities are altered by disease and therapies. The impact on the social, emotional and cognitive components and therefore on QOL is stronger than in long-term chronic diseases. 12 The baseline QOL scores of our population were lower than in most other studies. 9 Many patients benefited from the voice system and high satisfaction scores were noted, although for some fragile patients (i.e. Karnofsky index <50), the TLC system may not be appropriate. It may be perceived as a ‘cold and inhuman procedure’ when the patient is experiencing psychosocial distress and needs a warm relation with supportive care-givers. In a preliminary multivariate analysis (data not shown), we found some items that could predict responders and non-responders. These were a baseline Karnofsky score of over 60, age under 65 years, no chemotherapy or radiation therapy. A future prospective study is required to confirm the categories of patients who can benefit the most from enteral nutrition with TLC at home.
Footnotes
Acknowledgments
The research was supported by Nestle Home Care and Nestle Clinical Nutrition. We thank Nicolas De Sagazan, Jean Marie Plaze and Julien Gautry.
Appendix 1 Voice messages in the automatic telephone calls
‘Good morning, you have agreed to participate in the “nutrivigilance” study and we thank you for that. Now press your personal pincode number.’
If correct: ‘Thank you. At the end of each question press a single number to answer, from 0 to 9. Remember that in case of an emergency related to nutrition, you should phone the Doctors or the Nestle Home Care 24 hour Hot Line service (toll free number): 0800 820 820. Now here are six questions.
Question 1: Do you have repeated vomiting? Press 1 if yes, Press 0 if not.
Question 2: How many liquid or non-solid stools do you have in a day? Type from 0 to 9 (if more than 9 a day, type 9)
Question 3: What is your pain score (or discomfort score) related to the feeding tube? Press from 0 (none) to 9 (the most severe pain or disagreement)
Question 4: Concerning the feeding tube, what is your degree of difficulty passing the nutrition bags by this one? Press 1 no difficulty, 2 rather easy, 3 rather difficult, 4 difficult.
Question 5: Concerning nutrition bags, how many do you take per day? All of them: press 1; about 75% of the total, press 2; about half of the total: press 3; less then half or nothing: press 4.
Question 6: What was the date of your last stool? Type 0 if today, 1 if yesterday, 2 if 2 days ago and so on.
Thanks for your answers. Have a nice day’.
Appendix 2 Preset threshold for an email alert
Q1. Response 1 for vomiting (1).
Q2. Number of faeces
Q3. Response
Q4. Response 3 or 4 for tube clogging (3, 4)
Q5. Response 3 or 4 for nutrition intake (3, 4)
Q6. Response