
Abstract
We developed an interactive mobile-phone based application, SmartDiet, that analyzes daily nutrition intake and patterns of daily exercise. It provides a personalized diet profile and promotes knowledge about nutrition using a diet game. We evaluated the effectiveness of the SmartDiet application in terms of acquiring dietary information, weight control and user satisfaction. A case-control study was conducted over a six-week period, with 19 people in the intervention group and 17 people in the control group. During the study, a total of 235 successful data transmissions were performed from the mobile phones and there was a mean of 12.4 transmissions per participant. The three body composition measures (fat mass, weight and body mass index) decreased significantly after the intervention in the intervention group, but there were no significant changes in the control group. In a questionnaire survey at the end of the study, the majority of the participants responded that the system was useful for obtaining information and managing the diet process. The SmartDiet mobile weight management application appears to contribute to weight loss in obese adults.
Introduction
Cardiovascular disease, obesity and lack of physical fitness are increasingly common and damage people's health. In Korea, more than a quarter of people had a body mass index (BMI) greater than 25 kg/m2, which is considered to represent obesity (33% of men and 29% of women). 1,2 Obesity is related to a metabolic syndrome and therefore obese people are at a greater risk of developing cardiovascular disease.
Several studies have shown that computer-game software can provide nutrition knowledge, and facilitate and reinforce dietary management for weight loss. 3,4 The board-game Kaledo increases food variety in healthy children with problems of food refusal, and was demonstrated to be effective in providing nutrition knowledge and promoting a healthy dietary behaviour for children from three middle schools in Naples, Italy. 5 MetaKenkoh, a web-based activity-contingent game, also showed potential to facilitate increased physical activity in children. 6 MOPET is a wearable system that supervises a physical fitness activity based on alternating jogging and fitness exercises in outdoor environments. It provides knowledge elicited from sports physiologists and professional trainers. 7 An automatic transcript of spoken dietary records (SDRs) facilitated the provision of real-time dietary records. 8
In addition, a web-based therapy management system with mobile phone access has been developed for obese patients to support weight management. After users logged in and entered their personal information, automated feedback with recommendations was provided. 9 Educating overweight people about healthy eating through modern play-based educational tools appears more likely to succeed than food prohibitions or conventional teaching.
The use of mobile phones can provide a real-time dietary record, and therefore increase the potential advantages for accessibility, ease of use, and options for near-instantaneous transfer of dietary information. 10 One of the main advantages of a mobile phone is its ability to connect wirelessly to a central computer, thus enabling the centralization of individual nutrition and physical activity information, in contrast to wired systems which are constrained to the location where the connection exists. In Korea, about 70% of the population are mobile Internet subscribers, who use the technology as a communication network for everyday life such as mobile shopping, banking and advertising. 11
We developed the SmartDiet, a mobile phone-based weight control system that tracks an obese patient's daily nutrition intake, and also has games that users can play to learn about weight control. The SmartDiet is different from previous dieting applications because users can download and implement personalized dietary information onto their personal mobile phones, rather than having to access the mobile Internet browser every time they want to access the diet program. The present study evaluated the effectiveness of the mobile phone application SmartDiet with respect to acquiring dietary information, weight control and user satisfaction.
Methods
The SmartDiet is composed of two modules: a Diet Planner which provides the personalized nutrition information for food and activity, and calculates the proper calorie and exercise level; and a Diet Game which provides a game-style learning tool about how to control nutritional intake and exercise. We developed it with the JBuilder software for JAVA script programming and the SKVM communication protocol (developed by SK Telecom) using a screen size of 240 × 320 pixels. We developed SmartDiet using a PC emulator with a fixed 240 × 320 pixel screen size. The emulator creates a mobile phone environment on a PC screen.
Unlike other studies on mobile phone applications for weight control, 9,12 we used the server to download the SmartDiet program onto mobile phones and receive information from the mobile phones, maintaining and updating a large calorie database, storing user information, and maintaining and updating the Diet Game. Answers in the Diet Game (100: general dietary quiz, 101: quiz on food intake, 102: quiz on exercise) and the calories calculated by the SmartDiet application on the mobile phone (200: food intake, 201: exercise) were sent to the server (see Figure 1). Due to the limitation of the mobile phone's memory space, information on food intake and exercise could not be stored in the mobile phone for a long period of time and were sent to the server once a month.

Server data from the Smart Diet application
Diet planner
User management
The user could enter demographic information via the user management screen, except sex and blood type which were downloaded from the server (Figure 2). Gender information was included in the server because the recommended calorie intake, which was calculated by the server, varies according to the gender. We also included the blood type because most Koreans believe that it affects individual lifestyle and health. Lifestyle information and purpose of use were also entered via the user management screen. In the present study, we defined regular eating as having a meal within one hour of the average meal time. Based on this information, a three-dimensional image representing the user was displayed on the screen in the form of an Avatar. There were three types of Avatar: skinny, normal and fat. The Avatar could be altered according to the weight changes, enabling the user to virtually simulate their current and future body shape.
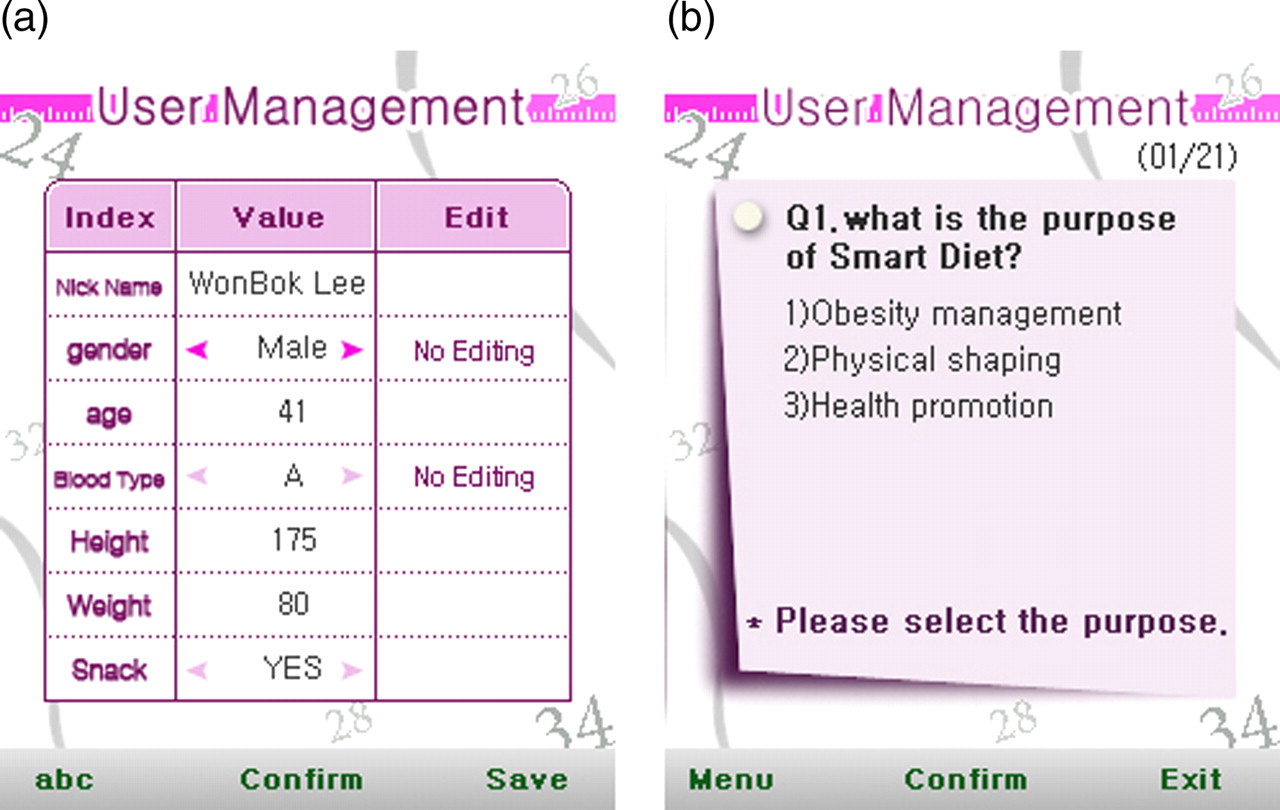
User management screen. (a) User information; (b) Purpose of SmartDiet
MyPage
The MyPage application recorded the daily calorie intake and consumption. The application automatically calculated the essential (or suggested) calories, based on the demographic and lifestyle information, and displayed the calorie information for the present, previous week and previous month (Figure 3). If the calorie intake was less than the calorie consumption, it meant that more body fat was used than stored. If intake was greater than consumption, a lower calorie intake was recommended. This function can help people to develop a diet plan and manage their own weight.
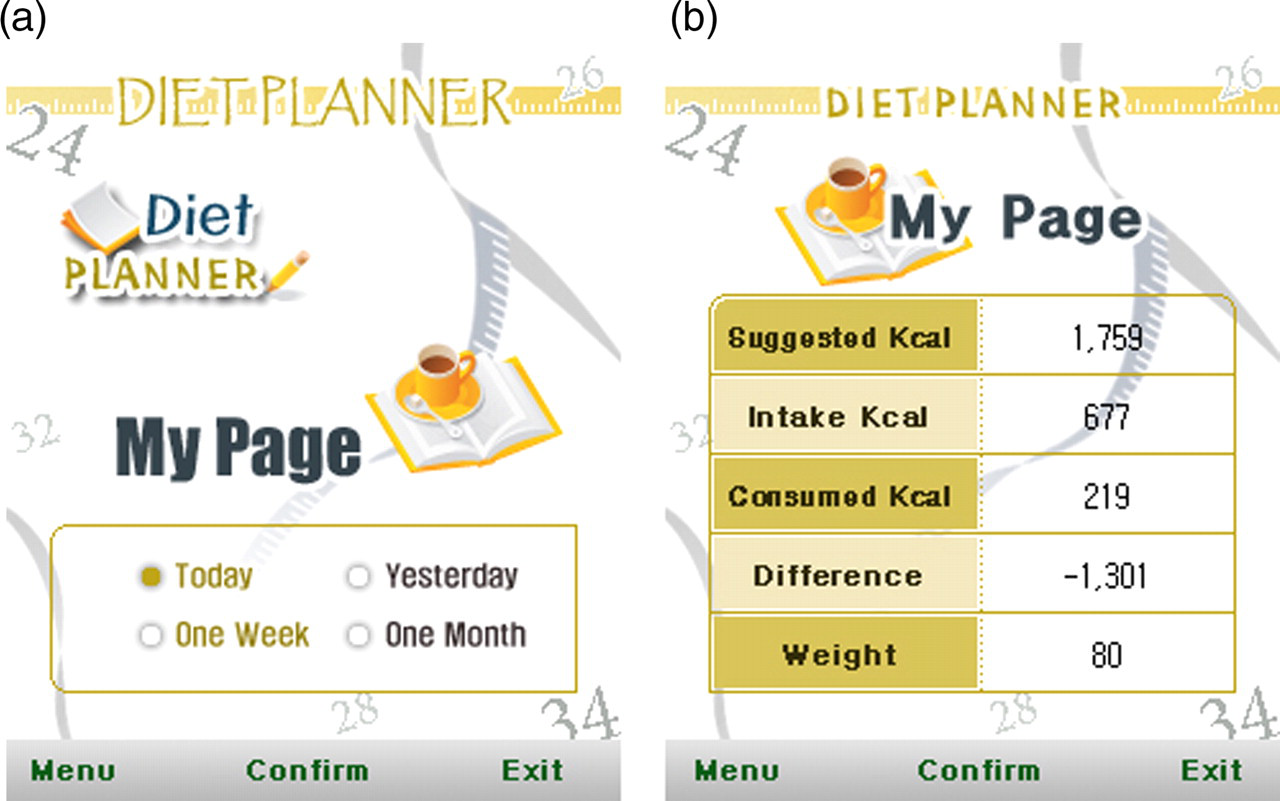
Screenshot from the MyPage application. (a) Planning period; (b) Assessment of calorie intake for the period
Meal assessment
The calorie intake and consumed calories for each meal were calculated based on the information from the food and exercise database which contained information about 600 kinds of foods and 100 types of exercise. The database was developed using the dietary recommendations and standards based on the book by Han. 13 The suggested calorie content for each meal, actual calorie content, and the difference between the two were displayed on the Meal assessment screen (Figure 4).

Screenshot from the meal assessment function of the Smart Diet application. (a) Calculation of calorie intake for the meal; (b) Assessment of daily diet
Exercise plan
Calorie requirements for exercise could be calculated either manually or automatically using a stop-watch function in the mobile phone. For example, when the user selected the stop-watch function and began walking, the calories consumed were calculated and displayed when he or she finished walking.
Diet Game
The Diet Game provided a quiz-based learning tool for recommended exercise type and intensity. It used simple true/false quiz or multiple choice questions for exercise, nutrition and life style. It contained three types of questions, based on life style, calories consumed and calories digested (Figure 5). The user could set the target weight and could simulate a proper diet profile over a period of six months. The target weight reduction was less than 4 kg a month to stay in a healthy condition. The contents of the Diet Game were obtained from information in the books by Han 13 and Yoo. 14 After the SmartDiet application was developed, it was pre-tested by nutritionists and nurses at the obesity clinic.
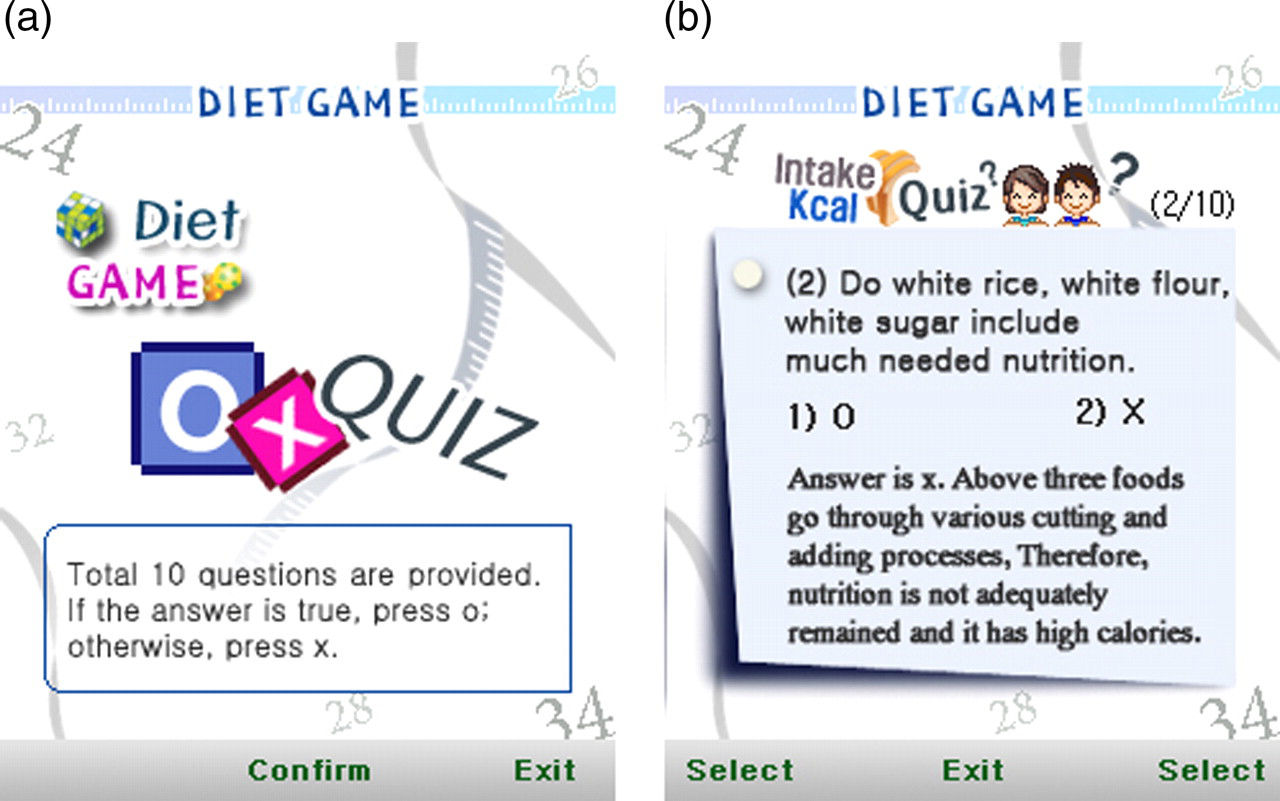
Screenshot from the Diet Game application. (a) Title page of the Diet Game; (b) Diet quiz for nutrition
Study design
The effectiveness of the SmartDiet application was evaluated based on a case-control design. A total of 19 subjects were assigned to the case or intervention group, and 17 subjects were assigned to the control group. They were all voluntary participants from the obese clinic at the fitness centre in Seoul and all of them signed an informed consent form before the intervention. All subjects were told about the study prior to the intervention process. They were informed about the intervention process, functions of the SmartDiet program, how to use it and the communication costs. However, they had to pay for the communication, which was about $1.30 for downloading the SmartDiet program and about $0.20 for sending the meal and exercise information to the server. They were allowed to access the SmartDiet game through the mobile phone Internet connection for six weeks starting in April 2008. Body composition for each participant was measured at the beginning and the end of the intervention in order to assess the changes in body composition at the clinic by using an analyzer called the Inbody system. The demographic characteristics and lifestyle information was surveyed on the first day of the intervention.
Differences in demographic characteristics and lifestyle between the intervention group and the control group were analyzed using a chi-squared test. The changes in body composition before and after the intervention for both groups were compared by a paired t-test.
Results
The average ages of those in the intervention and control groups were 28.2 and 29.5 years, respectively. The difference was not significant (Table 1). There were more office workers in the intervention group (42%) than the control group (29%). There were fewer participants without a job in the intervention group (32%) than the control group (41%). Most of the participants in both groups had at least a college education. There were more participants with a monthly income of over $4000 in the intervention group (79%) than in the control group (59%). However, none of these differences between the groups was significant.
Demographic characteristics. Values shown are the number of subjects (%)
The percentages may not add up to 100% due to rounding errors
Lifestyle
Percentages of participants who did not exercise were 47% for the intervention group and 35% for the control group; and percentages of participants who exercised more than three times a week were 26% for the intervention group and 18% for the control group (Table 2). Participants in the intervention group tended to eat more regularly than those in the control group. The percentages of participants who had never eaten irregularly were 32% for the intervention group and 24% for the control group; the percentages of participants who often ate irregularly were 26% for the intervention group and 29% for the control group. Participants in the control group ate less when they felt stress (21%) than the participants in the control group (24%). The percentages of participants who had never smoked were 90% for the intervention group and 77% for the control group. The percentages of participants who drank more than once a week were 26% for the intervention group and 29% for the control group. However, these differences in lifestyle were not significantly different between the two groups.
Lifestyle information. Values shown are the number of subjects (%)
The percentages may not add up to 100% due to rounding errors
Data transmission
A total of 235 successful data transmissions were performed. The mean number of transmissions was 12.4 per patient. Of these, 62 transmissions were related to the Diet Game (47 for the general dietary quiz, 9 for the quiz on food intake and 6 for the quiz on exercise) and 173 transmissions were related to the Diet Planner (134 for calories on food intake and 39 for calories on exercise).
Body composition
The three body composition measures (fat mass, weight and BMI) were significantly decreased for the intervention group, but none of the measures in the control group were significantly decreased after the intervention (Table 3).
Body composition before and after the intervention
*P < 0.05
SmartDiet
The majority of the participants thought that the SmartDiet application was useful for obtaining information (58%) and managing the diet process (50%) (see Table 4). In particular, 83% and 67% of participants in the intervention group responded that the system was useful for checking calories and consumed calories. Therefore, the mobile application was useful for obtaining dietary information.
System usefulness (n = 12)
System effectiveness
Of the participants in the intervention group, 58% agreed that the system was easy to use and the contents were interesting (Table 5). The cost to transmit data to the server was about $1.5 and the participants thought it was reasonable. All participants agreed that the system was easy to access. Therefore, the system was judged to be very effective in terms of content, cost and access. Fifty-eight percent of the participants intended to use it in the future and 67% of them stated that they would recommend the system to others. In addition, most of the participants (75%) used the system once a week and 8% used it every day.
System effectiveness
Discussion
Obesity is closely related to various diseases, such as cardiovascular diseases, diabetes and hyperlipidaemia. Previous studies have shown that dieting is effective in reducing weight and preventing obesity. The present study addressed whether the mobile phone application, SmartDiet, could help people to lose weight by the provision of immediate access to a caloric database, the function of calorie calculation, and the Diet Game which is a quiz-based learning tool for recommending exercise type. The results of the present study suggest that mobile phones have the potential to contribute to dietary management and that people perceive the system as being useful and effective in controlling their weight.
Mobile and wireless communication for health care represents the evolution of telemedicine from desktop to wearable technologies. 15 There have been several attempts to use the mobile phone to send text therapy messages to obese patients and diabetes patients. Morak et al. 9 developed a web-based management system with mobile phone access and conducted a pilot study with obese patients. Joo et al. 12 used short text messages for sending therapy messages to community residents and found a reduction in their waist sizes and weights. The changes in body weights and the BMI for obese patients from Morak's study were 2.4 kg and 0.78 kg/m2; and 1.6 kg and 0.6 kg/m2 for community residents from Joo's study, respectively. While our results (fat mass reduced by 1.2 kg, body weight reduced by 2.0 kg and BMI reduced by 0.75 kg/m2) were not significant, perhaps because of a short intervention period and because many subjects were not obese, these changes were similar to those from other studies.
In the present study, a total of 235 successful data transmissions were performed and the mean number of transmissions per participants was 12.4. These figures were slightly lower than those in Morak et al.'s study (361 transmissions and 14.4 per patient). Istepanian et al. 16 evaluated the effectiveness of a mobile phone monitoring system for glycaemic control in patients with diabetes. While these studies found that mobile phone applications were effective in controlling obesity and diabetes, they used simple text messages or required the subjects to use a mobile Internet browser every time they wanted to access the dieting program.
In our approach, we developed a dietary therapy program with a therapy database, which can be installed on individual mobile phones. Once the SmartDiet program was installed onto the user's mobile phone, it was easier to access therapy information than by using a mobile web browser every time the user wanted to retrieve dietary information. This resulted in increased user satisfaction. In addition, we used a case-control design to control for socio-demographic factors that might have affected the body composition measures. The findings of our study add to those of earlier studies that reported the effectiveness of text messaging for body composition reduction and metabolic variables.
There were, however, some limitations to our study. Only 19 people participated in the intervention and therefore it is difficult to generalize the results. In addition, we encouraged the participants to enter their food intake at every meal time and how much they exercised at every exercise session, in order to examine the effects on weight. However, only 8% of participants followed the instructions every day and 75% of participants used the system about once a week. Since they were all voluntary participants, we could not force them to use the system every day. In future, a more effective way to encourage them to use the system will be required. Moreover, the intervention period was limited to six weeks and therefore we were unable to measure the long-term effects. In addition, only subjects using SK Telecom mobile phones with a 230 × 240 pixel screen were used in the study. Since the SmartDiet program can be used by other mobile phones after a simple conversion for screen size and communication protocol, it should be tested more widely in future.