
Abstract
We explored the feasibility of engaging young black men in a 12-week text messaging programme about HIV prevention. There were two non-randomized groups of 30 young men each. The participants were aged 16–20 years, self-identifying as black or African-American, sexually active, who owned a mobile phone and lived in Philadelphia. They received three text messages per week for 12 weeks. People in the intervention group received text messages about HIV prevention, while those in the control group received text messages about nutrition. The intervention participants showed trends in increased monogamy at follow-up compared to controls. Awareness of sexual health was significantly higher in the intervention group. Condom norms were significantly higher for the control group. There were no differences in the proportion of protected sex acts. The participants embraced the project, and were enrolled and retained in numbers that suggest such an intervention is worth examining for efficacy.
Introduction
Using computers and the Internet to deliver prevention messages can have significant effects on behaviours that reduce HIV risk. 1–3 The popularity of the mobile phone with text messaging capability offers intriguing options for HIV prevention, particularly among young black males. In the USA, approximately 75% of adults have mobile phones and 62% use them for text messaging, email, taking pictures, recording video or looking up information. 4 Recent reports suggest that using mobile phones for health promotion may be helpful. A meta-analysis of 14 programmes using mobile phones to promote smoking cessation, physical activity, diabetes and asthma self-management, and adherence to hypertension medication shows that delivery of text messages via mobile phones has positive short-term behavioural effects. 5 Another review of 25 studies using mobile phones demonstrated positive effects in behavioural outcomes associated with smoking and with changes in biomedical outcomes such as reduced HbA1c and lower cholesterol. 6
In these meta-analyses, only two studies focused on HIV. One study was an assessment of a smoking cessation intervention for the HIV-positive population, 7 while the other showed increases in adherence to HIV medication among persons with memory impairment. 8 Other work is emerging showing the feasibility of using mobile phones for prevention of HIV- and other sexually transmitted disease (STD)-related risk behaviours. Lim et al. reported on the use of mobile phones to improve communication between STD clinic patients and providers, to improve and facilitate contact tracing, and to offer reminders for medication adherence related to reproductive health. 9 Levine and colleagues reported on a programme to offer sexual health information via text messaging to persons who sent inquiries to SexInfo, a mobile phone service with a library of pre-programmed text message responses. 10 Vodaphone and the United Nations have published information promising mobile phone-based health promotion efforts for HIV prevention in developing countries. 11 The emerging work in sexual health promotion and HIV prevention via mobile phones is promising, but at present there is no evidence for the efficacy of this approach.
We have conducted a pilot test of mobile phone text messaging for HIV prevention among young black men in Philadelphia. The study was designed to (a) test the feasibility of recruiting and retaining men in the 12-week programme and (b) assess the programme's effects on HIV-related risk behaviours.
Methods
The study was approved by the appropriate ethics committee. The programme development and enrolment processes have been described elsewhere. 12,13 The 60 participants were young men aged 16–20 years, who lived in Philadelphia, owned a mobile phone and self-identified as black or African-American. There were two non-randomized groups, each comprising 30 men. Men were recruited from seven community-based organizations. We purposively assigned the organizations to intervention or control status in order to avoid contamination — if a young man in one organization enrolled in the programme, he could potentially discuss his involvement with another participant accessing services at the same organization.
The text messages sent to participants were created with advice from 16–20-year-old black men participating in formative focus groups in Philadelphia. 12 The intervention messages focused primarily on increasing condom use and reducing the number of sexual partners. The messages were designed to increase positive outcome expectancies, norms, self-efficacy and intentions for condom use, based on evidence that such matters affect actual condom use in practice. 14–17 Examples from the library of text messages and the outcomes intended are provided in Table 1.
Example text messages
People in the intervention group received text messages about HIV prevention, while those in the control group received text messages about nutrition. All participants completed baseline assessments at the time of enrolment, and were invited to complete a follow-up assessment at three months and a second follow-up at six months. After completing each survey, participants were given $40 to help cover the payments for their mobile phone and the increased cost of receiving and sending additional text messages for the study. Participants received text messages of 160 characters or less three times each week for 12 weeks during the intervention period. We sent at least one quiz per week, asking participants to text their response back to us, in order to assess their engagement with the programme.
We measured demographics (age, education and income), HIV risk awareness, attitudes towards using condoms (both positive and negative), condom norms (perceptions of how normative it is for friends and peers to use condoms), self efficacy (confidence in using condoms in diverse settings and circumstances), intentions for condom use and condom use behaviour. Measures for attitudes, norms, self-efficacy and intentions were based on those developed and validated from previous research. 18–20 We asked factual questions about sexual health including questions on HIV epidemiology and transmission. The behavioural outcomes included assessment of partner monogamy in three months; experience with coerced sex; experience with arrest or incarceration; experience with being drunk or high during sex; having had male sex partners; and having a partner who tested positive for STD or HIV. We also assessed the proportion of protected sex acts in 90 days.
Statistical analysis was conducted using a standard package (SAS version 9.2). We compared baseline values for attitudes, norms, self-efficacy, intentions and behavioural risk factors for each group to determine if there were any group differences. At the three- and six-month follow-ups we assessed any changes by group. We then adjusted outcomes, controlling for age (treated as a class variable). Additional statistical adjustments were not possible (e.g. reliability corrections to adjust for measurement error found in non-randomized groups) due to the small sample size. We reconsidered if group assignment had any effect on behavioural risk factors with age adjustment.
Results
The study recruitment, enrolment and retention are summarised in Figure 1. The intervention group was significantly older than the comparison group (median 19 years versus 17, P < 0.0001). This was probably because recruitment for the intervention group took place in organizations where there was a larger proportion of men aged 18–20 years. All participants were male. Most were enrolled as students (77%) and the rest had graduated from high school or technical school. Approximately three-quarters of the participants lived with a parent or guardian.
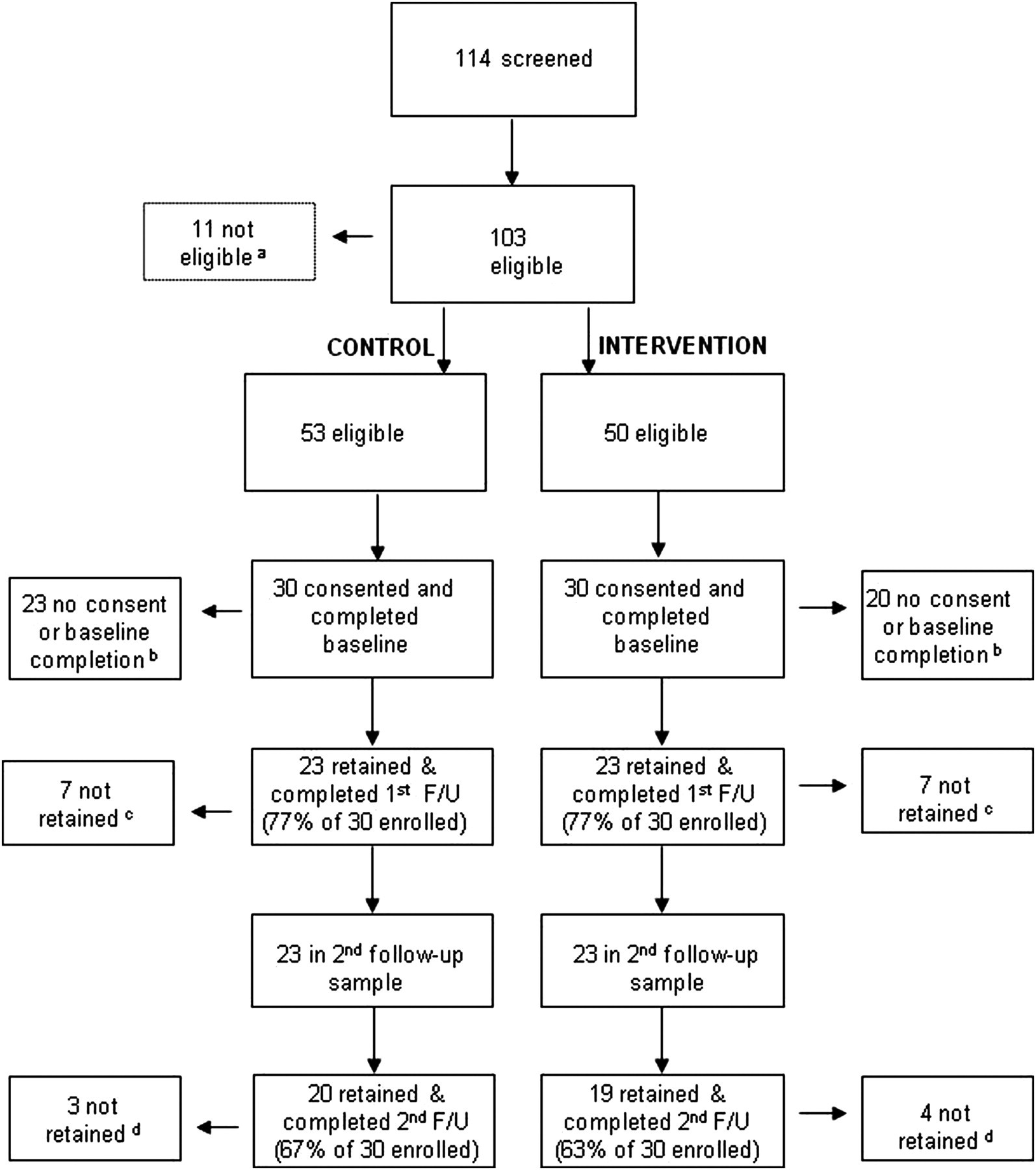
Recruitment, enrolment and retention. a11 not eligible because they had never had sex; b43 did not consent; c14 did not complete follow-up; d7 did not complete second follow-up
Equal numbers of men from the control and intervention conditions completed the three-month follow-up. At the six-month follow-up, 65% of those initially enrolled were retained. There were no significant differences in demographics between those who did and did not complete follow-up assessments. Participants in the control group responded to 49% of the quizzes and those in the intervention group responded to 65% of the quizzes.
There were significant changes or trends in three key outcomes: condom norms (Figure 2), sexual health awareness (Figure 3) and practising monogamy (Figure 4). Condom norms were higher for the control group versus the intervention group at all time points, even after adjusting for age (Student's t-test, and generalized linear modelling to control for age). This finding could be confounded by increased levels of monogamy, which is usually associated with lower levels of condom use. There was higher awareness of sexual health in the intervention group at all time points compared to the control group (Student's t-test, and generalized linear modelling to control for age). There was a significant increase in awareness of sexual health in the intervention group at three and six months compared to baseline (paired t-test). However, awareness was not significantly higher than in the control group.
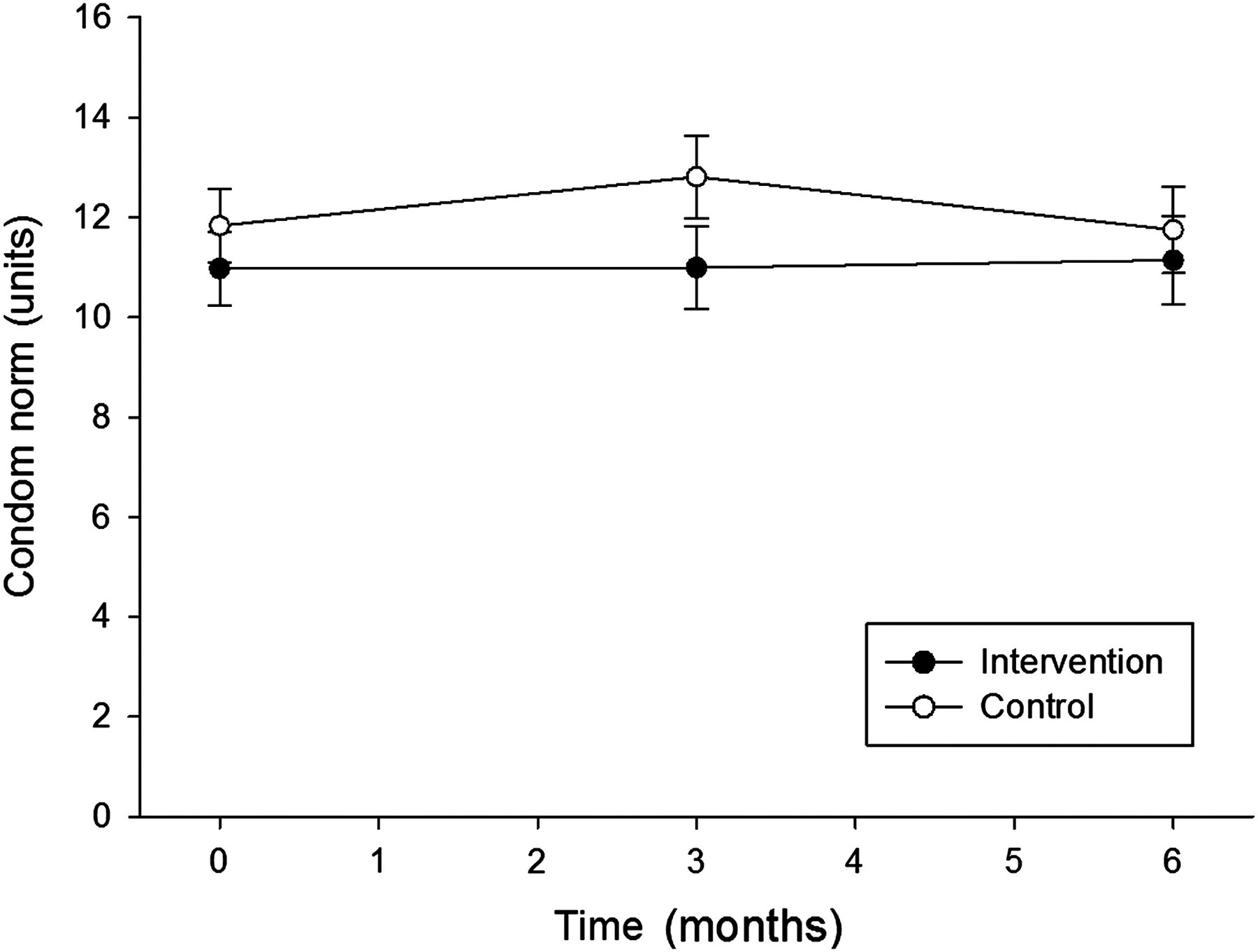
Condom norms, measured on a scale from 1 = no acceptability to 15 = complete acceptability. The error bars represent 95% confidence limits

Sexual health awareness, measured on a scale from 1 = no knowledge and 10 = completely knowledgeable. The error bars represent 95% confidence limits
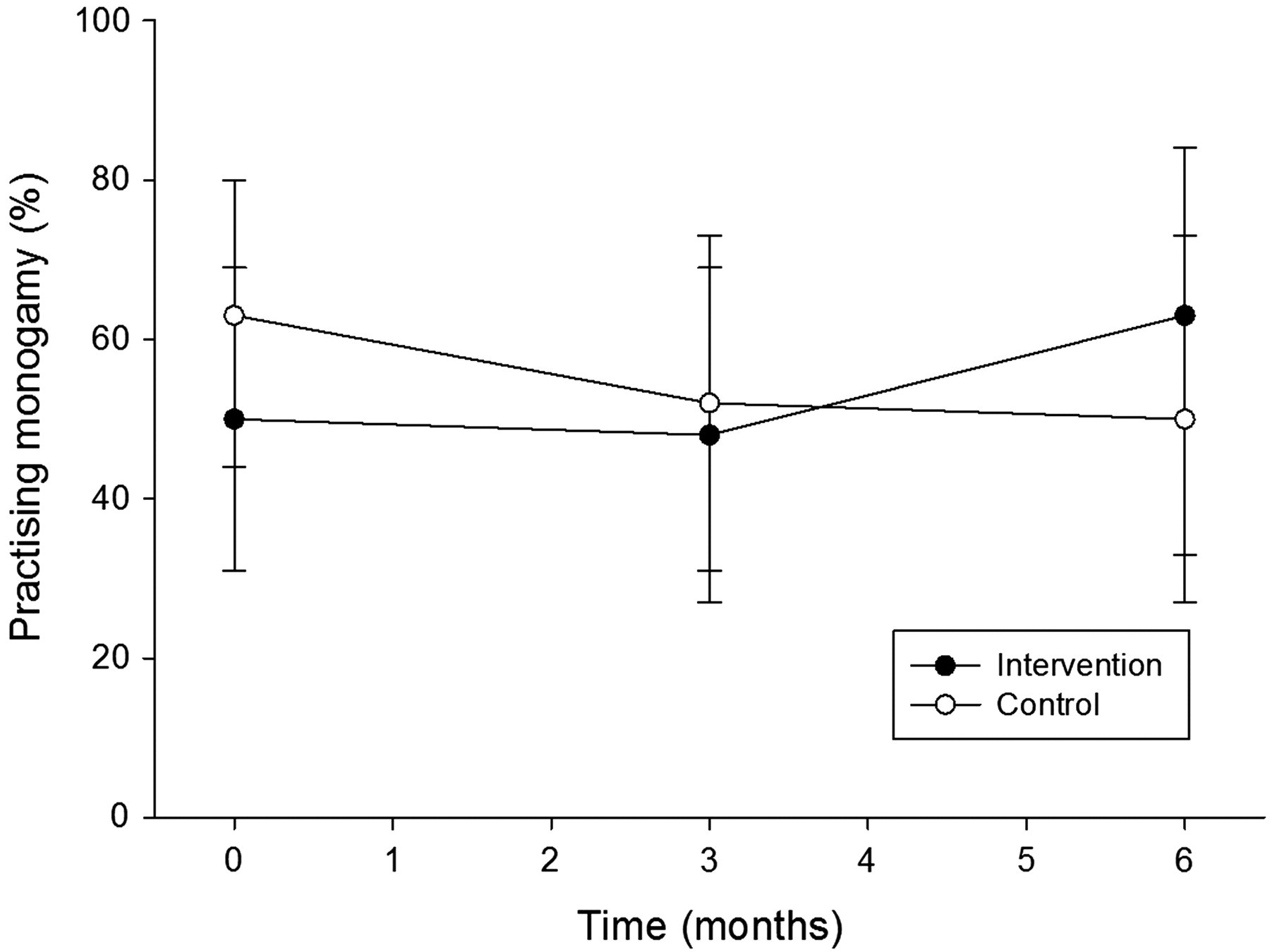
Proportion who were practising monogamy. The error bars represent 95% confidence limits
There were no significant changes in:
Condom intentions; Age of sexual debut; Experience with coerced sex; Experience with arrest or incarceration; Experience with being drunk or high during sex; Had male sex partners; Had a partner who tested positive for HIV; Proportion of sex acts protected by condoms in 90 days.
Discussion
The findings in the present study are promising, and warrant further work such as a randomized controlled trial. We have no explanation for the counter-intuitive finding that control subjects had higher condom norms than our intervention participants. This did not appear to translate into higher condom use for control participants.
We acknowledge some important limitations to this work. The intervention and control participants were not randomly assigned, and the sample size was quite small. Although we observed no change in condom use, we consider that this finding could be confounded by increased levels of monogamy, which is usually associated with lower levels of condom use. However, the study objectives were to determine if the delivery of text messages about HIV prevention was feasible and if it showed promise in a small sample of young black men. The participants embraced the project, and were enrolled and retained in numbers that suggest such an intervention is worth examining for efficacy. The next step is to conduct a large randomized controlled trial.
Footnotes
Acknowledgements
We thank the National Institute of Mental Health for financial support (Grant R21 MH083318). We are grateful to the community organizations in Philadelphia who helped with recruitment of study participants.